
Abstract
Introduction:
To examine racial variations in access to postacute care (PAC) and rehabilitation (Rehab) services following elective total knee arthroplasty and whether where patients go after surgery for PAC/Rehab is associated with 30-day readmission to acute care facility.
Materials and Methods:
Sample consisted of 129 522 patients discharged from 169 hospitals in the State of Pennsylvania between fiscal years 2008 and 2012. We used multinomial regression models to assess the relationship between patient race and discharge destination after surgery, for patients aged 18 to 64 years and for those aged 65 and older. We used multivariable (MV) regression and propensity score (PS) approaches to examine the relationship between patient discharge destination after surgery for PAC/Rehab and 30-day readmission, controlling for key individual- and facility-level factors.
Results:
Lower proportions of younger patients compared to those older than 65 were discharged to inpatient rehabilitation facilities (IRFs; 5.8% vs 12.6%, respectively) and skilled nursing facilities (SNFs; 15.2% vs 32.7%, respectively) compared to home-based Rehab (self-care; 23.3% vs 14.2%, respectively). Compared to whites, African American patients had significantly higher odds of discharge to IRF (age < 65, odds ratio = 2.04; age ≥ 65, odds ratio = 1.64) and to SNF (age < 65, odds ratio = 2.86; age ≥ 65, odds ratio = 2.19) and discharge to home care in patients younger than 65 years (odds ratio = 1.31). The odds of 30-day readmission among patients discharged to an IRF (MV odds ratio = 7.76; PS odds ratio = 8.34) and SNF (MV odds ratio = 2.01; PS odds ratio = 1.83) were significantly higher in comparison to patients discharged home with self-care.
Conclusion:
African American patients with knee replacement are more likely to be discharged to inpatient Rehab settings following surgery. Inpatient Rehab is significantly associated with 30-day readmission to acute care facility.
Keywords
Introduction
Total knee arthroplasty (TKA) is widely regarded as a safe and highly successful treatment option for end-stage osteoarthritis (OA) of the knee. As the US population ages, use of TKA is expected to accelerate. 1 In 2015, the number of annual TKAs performed in the United States is projected to exceed 1 million procedures. 2 This figure marks a 2-fold increase in TKA utilization over the past decade and an increase in annual hospital charges from US$7.42 billion in 2005 to US$40.8 billion in 2015. 2,3 As Medicare is the single largest payer for these procedures, the Centers for Medicare and Medicaid Services (CMS) has implemented a series of cost-containment changes to its reimbursement policies. These include the Inpatient Prospective Payment System (IPPS) and the Hospital Readmissions Reductions Program (HRRP). Beginning in fiscal year (FY) 2015, CMS will impose reimbursement penalties through the HRPP—up to 3% of total Medicare billings—on IPPS hospitals found to have “worse than expected” TKA readmissions.
According to the latest data from the Healthcare Cost and Utilization Project, approximately 120 000 (4.8%) TKA procedures resulted in early readmission in 2009 to 2012. 4 Prior research suggests 30-day readmission rates for TKA have steadily increased since the early 1990s, 5 with at least 1 study reporting the most dramatic rise among minority, and in particular African American (AA) patients: from 6% higher than white patients in 1991 to 24% in 2008. 6 Often, these readmissions signal inadequate discharge planning or poor care continuity between hospital clinicians and postacute care (PAC) or rehabilitation (Rehab) service providers, 7 yet little is known about racial variations in the patterning of PAC/Rehab care after surgery. Furthermore, PAC/Rehab encompasses a wide range of processes, locations, and intensities of care, 8 and despite growing demand for these services, little research on hospital readmission has been reported for patients according to rehabilitation setting.
Thus, our study sought to answer 2 questions with implications for efforts to reduce avoidable TKA readmissions: First, are there racial differences in where elective primary TKA recipients receive PAC/Rehab services? Second, is the location of PAC/Rehab services (discharge destination) associated with the likelihood of all-cause 30-day readmission to an acute care hospital?
Methods
Study Sample and Data Set
We used the Pennsylvania Health Care Cost Containment Council (PHC4) database to identify a cohort of patients who underwent elective primary TKA performed in the State of Pennsylvania in the 12 fiscal years (Fys) 2001 to 2012. Cases with TKA were identified using the International Classification of Diseases, Ninth Revision (ICD-9) code 81.54 for primary TKA.
Study Measures
The primary study outcome was the type of PAC to which the patient was discharged. This was defined using the patient’s discharge destination according to the setting in which services were delivered. The categories were home with routine self-care (home-self), home under care of organized home service (home care), skilled nursing facility (SNF), and inpatient rehabilitation facility (IRF). The primary exposure of interest was patient race. Because of the clustered nature of the data, and in order to account for distinct associations between patient-level (within-cluster) race and facility-level (between-cluster) race, we specified both patient- and facility-level measures and included both in our primary analyses. 9 Facility-level race was defined as the proportion of AA patients at each facility. Patient race was specified as the difference between the patient race indicator and the facility mean proportion of AA patients. Other patient-level variables examined as potential confounders were gender, age (categorized as 18-44, 45-64, 65-84, and 85 and older), insurance type (categorized as Medicaid, Medicare/government, or private), and the occurrence of any of the following major complications during the index stay: venous thromboembolism, myocardial infarction, surgical wound infection, and prosthetic device complication. These individual complications were identified using ICD-9 codes (see Appendix A).
Facility-level rural status was assigned based on rural–urban commuting area codes. 10 Facility procedure volume was determined for each study year based on the number of TKA procedures performed that year. We categorized facility procedure volume into 3 levels: low (less than 200), medium (200-400), and high (more than 400 TKAs performed). Patient comorbidity was summarized using the Elixhauser comorbidity index, a modification of the Elixhauser comorbidity index that combines the 30 Elixhauser indicators into a single numeric score. 11 We also examined readmission within 30 days, defined as an inpatient admission within 30 days of discharge from the index surgical hospitalization. The study was approved by the Institutional Review Board at the Philadelphia VA Medical Center.
Data Analysis
Descriptive statistics for patient demographic and clinical characteristics were calculated for the study sample overall, by race, and by Rehab destination. Comparisons of these characteristics in the study cohort were tested using chi-square tests after stratifying the sample by age (<65 years old and
We examined the association between Rehab destination and 30-day readmission. Unadjusted associations between 30-day readmission and Rehab type were estimated with mixed effects logistic regression models, with random facility intercepts. Multivariable mixed effects models also included patient gender, age, race, type of insurance, presence of in-hospital complications, Elixhauser score, facility-level race, facility rurality, and facility procedure volume.
In order to further reduce bias due to nonrandomized procedure for patient referral to type of Rehab service, we conducted a propensity score (PS) analysis. 12 We first developed a logistic regression model for discharge to each PAC or Rehab type (IRF, SNF, or home care) relative to home self. We included patient-level race, gender, age, type of insurance, an interaction of age with insurance type, Elixhauser indicators, in-hospital complications, and facility procedure volume and rural status and estimated a propensity score for each Rehab type for each patient. After evaluating and confirming that observed characteristics were adequately balanced within PS quintiles, 13 associations between type of Rehab service and 30-day readmission were estimated within PS strata. We report the pooled within-strata comparisons, 12 expressed as odds ratios (OR) for readmission, for each of the Rehab types (IRF, SNF, and home care) relative to home-self. Standard errors and 95% confidence intervals (CIs) were determined using the bootstrap method with 1000 bootstrap samples. Associations between where patient went for PAC or Rehab and 1-year mortality were not determined due to the very low mortality rate. All analyses were performed using SAS 9.3.
Results
Baseline Characteristics of the Study Sample
We identified 322 912 primary TKA procedures performed at 192 hospitals in the state of Pennsylvania between FYs 2001 and 2012. All TKA records indicating a discharge to a nonstudy Rehab destination (n = 1388), patient race not white or black (n = 15 086), or where the index surgery was primary bilateral knee replacement (n = 27 410) were excluded from the analysis. Additional exclusions are detailed in Figure 1.

Study sample flow and construction of the analytic sample.
In 2004, eligibility criteria for inpatient rehabilitation, commonly referred to as the 75% rule, were revised by CMS.
14
This policy modification resulted in significant shifts of Rehab utilization—reducing use of IRF and increasing use of SNF between 2004 and 2007. Trends in use of Rehab services types stabilized and remained relatively constant between 2008 and 2012, suggesting that implementation of the policy revision was complete. Therefore, our analysis focuses on the cohort of patients who underwent surgery between 2008 and 2012. We identified 129 522 primary TKAs performed at 169 nongovernmental (ie, non-Veterans Affairs) acute care hospitals in the state of Pennsylvania between FYs 2008 and 2012. The final analytic sample consisted of 121 449 (94%) TKA procedures performed on white patients and 8073 (6%) performed on AA patients. Procedures were stratified by patient age (n = 56,575 [43.7%] < 65 and n = 72,947 [56.3%]
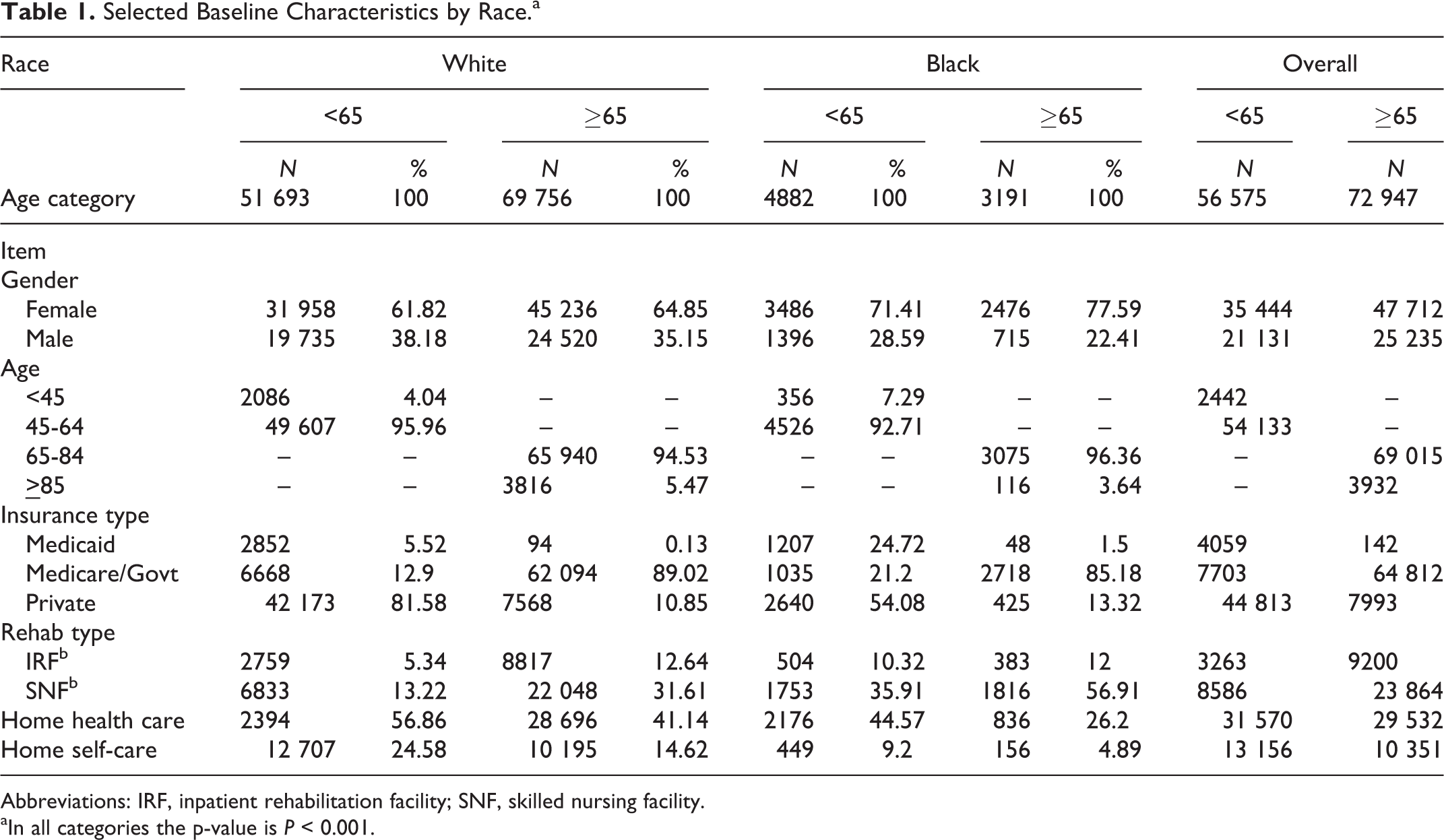
Selected Baseline Characteristics by Race.a

Abbreviations: IRF, inpatient rehabilitation facility; SNF, skilled nursing facility.
aIn all categories the p-value is P < 0.001.
Selected Baseline Characteristics by Discharge Destination.
Abbreviations: IQR, interquartile range; IRF, inpatient rehabilitation facility; SNF, skilled nursing facility; SE, standard error.
aIn all categories the P value is P < .001.
bCalculated using weights from van Walraven et al. 11
cReported as facility-level % black.
Race and PAC/Rehab Discharge Destination
Unadjusted odds of IRF referral versus home-self were significantly higher for AA patients compared to whites (<65, OR = 2.48 [95% CI, 2.10-2.93];

Adjusted odds of IRF, SNF, and home health care referral in African American patients by Medicare eligibility. IRF indicates inpatient rehabilitation facility; SNF, skilled nursing facility.
Postacute Care/Rehab Discharge Destination and 30-Day Readmissions
Figure 3 summarizes the reported unadjusted and adjusted odds ratios for 30-day readmission by IRF, SNF, and home care discharge destinations (referent is home-self for all models). Unadjusted analysis found the highest odds of 30-day readmission among patients discharged to IRFs (OR = 10.06 [95% CI, 9.21-10.99; P < .0001]) followed by patients discharged to SNFs (OR = 2.53 [95% CI, 2.32-2.77; P < .0001]). The strength of the observed association was marginally diminished after adjusting for patient gender, age, race, type of insurance, presence of in-hospital complications, Elixhauser comorbidities, hospital rurality, and hospital procedure volume: discharge to IRF (OR = 7.76 [95% CI, 7.08-8.51; P < .0001]) and SNF (OR = 2.01 [95% CI, 1.83-2.21; P < .0001) significantly predicted 30-day readmission. After stratifying by propensity score quintile for each PAC type, the odds of 30-day readmission among patients discharged to IRF (OR = 8.34 [95% CI, 7.5-9.3; P < .0001]) and SNF (OR = 1.83 [95% CI, 1.65-2.03; P < .0001]) were found to be significant. In both multivariable and propensity-adjusted analyses, discharge to home care following TKA did not increase the likelihood of 30-day readmission (P = .62 and P = .87, respectively).
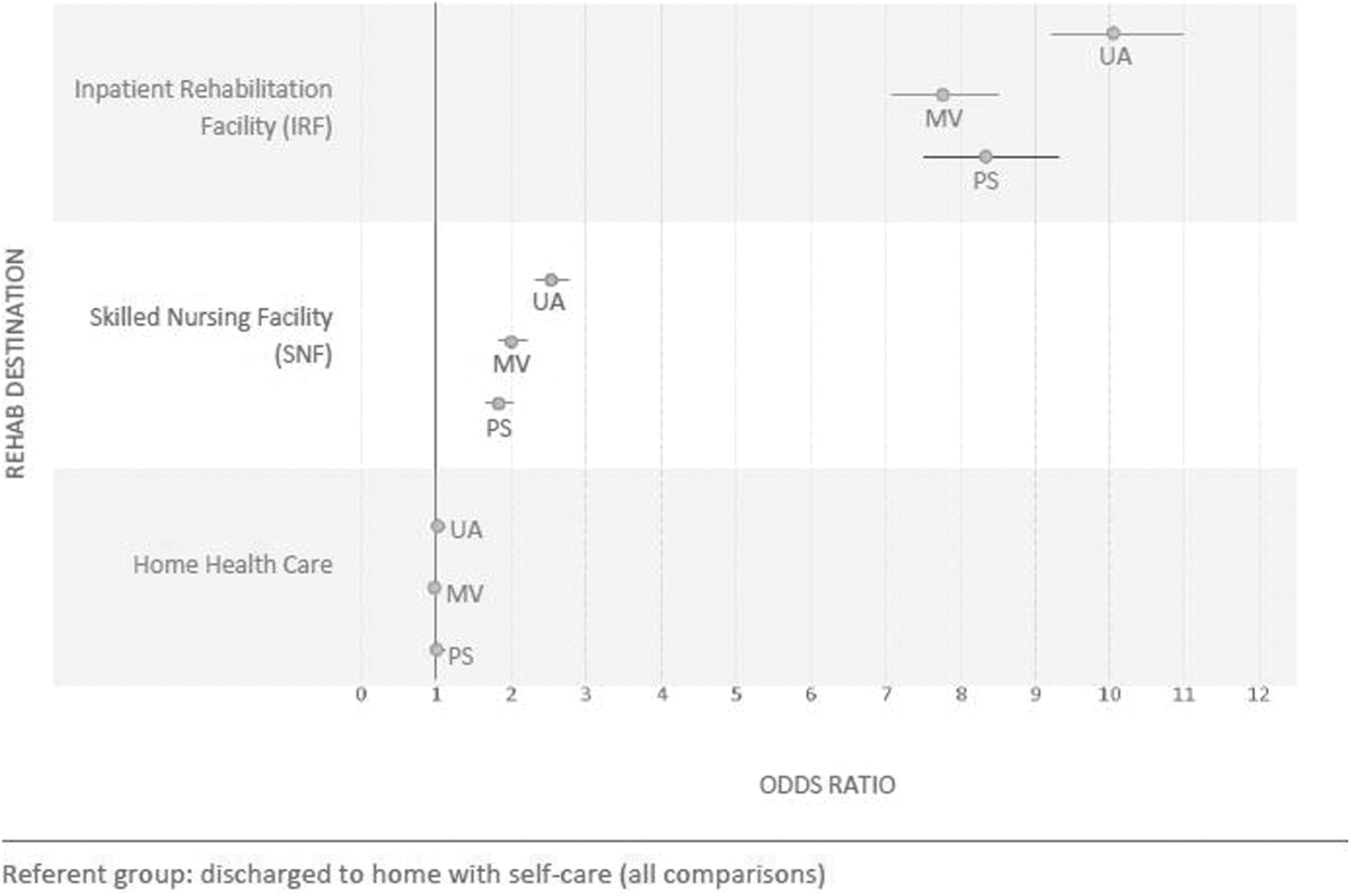
Unadjusted, adjusted, and propensity-adjusted odds ratios of 30-day readmission by rehabilation type.
Discussion
In this sample of nearly 130 000 patients who underwent elective primary TKA in the Commonwealth of Pennsylvania, we identified several distinct trends with implications for efforts to reduce TKA readmissions. First, we found significant racial variation in discharge destination after surgery. Compared to white patients and irrespective of Medicare eligibility age, AA patients had significantly higher odds of being discharged to institutional rehabilitation (IRFs and SNFs) following TKA. Second, we found patients discharged to IRFs and SNFs were readmitted to an acute care hospital 8.34 and 1.38 times more often, respectively, than patients discharged home.
Attempts to decrease future readmission rates will require an understanding of the complex interaction of hospital processes that influence readmission and its predisposing factors within patient populations. Numerous prior studies have examined these aspects independently 15 ; however, few have ventured to examine provider practices and patient-level factors in tandem or in depth. Thus, little is known about underlying mechanisms that account for how nonclinical factors—such as racial minority status or AA patient race—serve to increase the risk of readmission following TKA.
Intuitively and from other types of health disparities research, minority status is a proxy for many underlying “root cause” aspects that lead to poorer patient outcomes 16,17,18,19 —aspects that include limited health care coverage and, in turn, limited access to specialists and Rehab services. 20,21 Instructively, most joint replacement studies that have documented racial disparities in readmission rates have used Medicare data in which such coverage-based access limitations are mitigated. 22,23 Thus, for the bulk of TKA recipients, racial differences in access to PAC/Rehab services are unlikely to sufficiently explain observed differences in readmission. The present findings offer an alternative plausible factor: racial variation in the utilization of higher level institutional PAC/Rehab services.
In a health care climate that increasingly emphasizes the importance of resource management and high-value care, 19 there is a striking absence of standardized, evidence-based criteria to help providers determine the most cost-effective and clinically beneficial modality of PAC/Rehab services. 24,25,26,27 As pressure mounts to reduce readmissions, many well-meaning providers may err on the side of higher than necessary PAC/Rehab care as permitted by adequate health care (most often, Medicare) coverage. 25 Our findings suggest that such decision making may particularly influence the trajectory of AA patients with TKA and, ultimately, may serve cross purposes, specifically to increase the risk of rehospitalization for these patients.
Our study is one of several that has examined PAC/Rehab utilization patterns after joint replacement surgery and found significant variation in the use of institutional services by race. Freburger et al, 28 in a multistate analysis of hospital discharge data, noted AA patients covered by Medicare of private insurance were more likely to use institutional PAC relative to white patients in the same coverage group (OR = 1.69). Further, among all patients receiving institutional PAC, AAs from a majority of states were more likely than whites to use SNF care as opposed to IRF care. Earlier research supports these differences: In a descriptive analysis of Medicare data, Buntin 8 reported a larger percentage of nonwhite TKA recipients received institutional PAC relative to whites. While comparisons of our findings to the previous research are complicated by the recent phase-in of the newly revised 75% rule—a time of major shifts in rehab utilization patterns—our study confirms that the increased likelihood of AA patients receiving institutional PAC/Rehab services persist in the present policy environment.
To our knowledge, our study is the first to examine both racial variation in PAC/Rehab destination and subsequent risk of readmission by PAC/Rehab setting using a single sample of TKA recipients. However, the specific contribution PAC/Rehab setting to the risk of readmission has been documented in prior joint replacement studies. Similar in part to the present analysis, articles by Bini et al 29 and Ramos et al. 30 examined readmission rates for patients who underwent primary joint replacement surgery and were discharged to either institutional or home-based rehabilitation settings. Consistent with our results, both analyses found higher risk for readmission in patients who received SNF or IRF care compared to those discharged home with healthcare services.
As noted in both Bini et al 29 and Ramos et al, 30 there is potential for PAC/Rehab readmission findings to be confounded by indication: As institutional rehabilitation facilities typically serve patients with the greatest needs for supervised care, 31 it is a reasonable expectation that IRF and SNF patients would be readmitted to acute care hospitals at higher rates than patients discharged home. A major contribution of our study is the use of propensity-adjusted analysis to balance key factors—such as patient age and comorbidity score—that were different between PAC/Rehab patient groups (in effect, mimicking the setting of a randomized, clinical trial). 12 Although administrative data do not provide adequate detailed information to examine all of what shapes clinical decisions on where patients are discharged after surgery, the marked difference in readmission rates between those who received IRF or SNF care and those who went home in our analysis cannot be entirely explained by differences in patient care needs.
There are important limitations to consider when interpreting the results of our study. First, the present analysis used a large administrative database that was designed for hospital performance assessment but contains inadequate information on potential confounding variables including body mass index, preoperative pain, function, and radiographic severity. Second, our sample consisted of only patients who underwent surgery and postacute rehabilitation in the Commonwealth of Pennsylvania. Our conclusions may not be readily extrapolated to other regions or states of the country, as there is significant regional variation regarding the rates of TKAs performed. 32 Fourth, it is conceivable that coincident geographic variation in available PAC/Rehab facilities and clustering of patient subgroups by race may play a role in the chosen level of care postdischarge. As many AA patients dwell and receive care in Pennsylvania’s large, urban metropolitan areas, it is possible that these patients consider or are offered different rehabilitation scenarios than their rural counterparts, which could affect our results. Finally, there is recent evidence which suggests that some patients (approximately 4%) 33 receive multiple levels of PAC/Rehab services during an episode of care. 34 The degree to which this potential crossover effect may have impacted our finding is unknowable yet must be considered in any interpretation of our findings.
Conclusion
The present study found that AA patients who underwent primary elective TKA across 169 Pennsylvania hospitals were more likely to utilize SNF and IRF compared to white patients and that discharge to institutional scenarios for rehabilitation entails greater odds of 30-day readmission compared to patients discharged home. Future prospective studies should evaluate the criteria currently used by providers and patients to form decisions about postacute setting after TKA and how patient race impacts this process. More work needs to be done to investigate why patients discharged home with home health or self-care are less likely than those admitted to IRF or SNF to be readmitted to an acute care hospital within 30-days after elective TKA.
Footnotes
Appendix A
Authors’ Note
No author has affiliations with or involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in this article. This article is not under consideration elsewhere. There is no conflict of interest in connection with this report. All the authors listed contributed significantly to this work and have read and approved the article. They take full responsibility for the content of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Ibrahim is supported by Grant Number K24AR055259 from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.