
Abstract
Introduction:
Longer-term outcomes of patients with geriatric type II odontoid fracture nonunion remain unclear.
Methods:
Thirty-four consecutive geriatric patients (>70 years old) with minimally displaced (<50% displacement) type II odontoid fractures were treated 24 hours a day for 12 weeks with rigid collar immobilization between the years 2003 and 2011. Radiographic and medical record reviews were performed on all 34 patients. Additionally, 7 patients were available for clinical longer-term follow-up (>4 years).
Results:
In all, 30 (88%) of the 34 patients had nonunion after 12 weeks of treatment, 2 (6%) patients had union, and 2 (6%) patients died during the first 12 weeks. Twenty-one of the 30 patients with nonunion had a displaced or mobile nonunion (70%), and 4 (12%) patients were lost to follow-up. At longer-term follow-up, 23 (68%) patients had died. The average time death occurred was 3.8 years with a range of 0.17 years to 9.42 years postinjury. Twenty of the 23 deaths were attributed to medical comorbidities not related to the patient’s odontoid nonunion. We were unable to determine the cause of death in 3 patients. None of the patients who died had identifiable clinical myelopathy prior to their death on chart review. Of the 7 patients who were alive, all were determined to have odontoid nonunion, of which 5 (70%) were mobile odontoid nonunion. Visual Analog Scale (VAS) and Neck Disability Index (NDI) scores were low (VAS averaged 0.57 and NDI averaged 6.9%) and treatment satisfaction was high (averaged 9.7 of 10). Scores for pain and function did not differ significantly when compared to age-matched controls (P = .08, t test).
Conclusion:
Rates of odontoid nonunion are high in patients with geriatric odontoid fractures that are treated with continuous rigid collar for 12 weeks. The majority of patients with nonunion appear to achieve high functional outcomes. In this study, mortality did not appear to be related to adverse neurologic events after treatment.
Introduction
Fractures of the odontoid account for 7% to 14% of all cervical fractures and are the most common cervical spine fracture in the geriatric population. 1 –4 Type II odontoid fractures, as described by the Anderson and D’Alonzo classification, 5 are fractures that occur at the junction of the odontoid process and the base of the second cervical vertebrae. Geriatric type II odontoid fractures (GOFs) are the most common type of odontoid fracture in the elderly patients. Geriatric type II odontoid fractures are attributed to degenerative changes, commonly occur from ground-level falls, and are increasing in incidence due to an aging population. 1,3,4,6 –12 Longer-term outcomes from odontoid nonunion have not been defined by the literature to this point.
Methods
Institutional Research Review Board approval was obtained. Thirty-four consecutive patients previously treated during a study period of 2003 through 2011 by a fellowship-trained spinal trauma specialist (RWM) were included. 13 Patients were older than 70 years at the time of their diagnosis and had minimally displaced fractures (<50% displacement) that were treated with 12 weeks of continuous (24 hours a day) rigid cervical collar use with aggressive early mobilization. Mobilization was undertaken with physical therapy and occupational therapy consultations and evaluations on hospital day zero. Patients received therapy twice daily during their hospitalization.
Of the 34 patients, 16 were male and 18 were female. The average age at the time of injury was 83 years with a range of 71 to 99 years. Thirty-two of the 34 patients were identified as having medical comorbidities, with the average number of comorbidities equaling 4.3 with a range of 0 to 10 comorbidities, as described previously in this patient cohort. 13
Hospital and outpatient charts were reviewed, and living patients were contacted for follow-up. Seven patients were located, and of these, 5 were available for an office visit with open-mouth and flexion-extension radiographs taken and interpreted by the senior author (RWM) to confirm odontoid nonunion. The remaining 2 patients were unavailable for an office visit but had previously performed radiographs that were reviewed and demonstrated odontoid nonunion. Functional outcomes were assessed using the Neck Disability Index (NDI) score, Visual Analog Scale (VAS) pain score, and treatment satisfaction score. The 2 patients who were unavailable for an office visit completed the NDI, VAS, and treatment satisfaction questionnaire via telephone.
Neck Disability Index scores were compared with that of 35 age-matched controls who had no history of cervical disorder (control group). There were 18 females and 17 male controls with an average age of 78 years with a range from 70 to 89 years (Table 1). The age-matched control group consisted of geriatric participants who were randomly selected from a busy multispecialty orthopedic clinic waiting room setting being seen for other orthopedic complaints not related to cervical spine pathology.
Control Participants.

Abbreviations: M, male; F, female; NDI, Neck Disability Index.
Three patients who were not located via telephone or follow-up notes were searched via online search engines and obituaries were found. Causes of death for the remaining study patients were determined from caregivers, family members, old records, and primary care physicians. Four patients were lost to longer-term follow-up, and living status was unable to be determined.
Statistical analysis was performed using a 2-tailed student t test to determine any statistical significance between the treatment group and the age-matched controls. The differences in functional outcomes between the control group and the study group was not found to be statistically significant.
Results
A total of 23 (68%) patients died during the review period. Of these, 3 (9%) deaths were for unknown causes. Table 2 outlines the patients who died at longer-term follow-up. Twenty (87%) of the 23 patients died from medical comorbidities not directly related to the odontoid fracture. Four (12%) patients were lost to follow-up.
Deceased at Longer-Term Follow-Up.
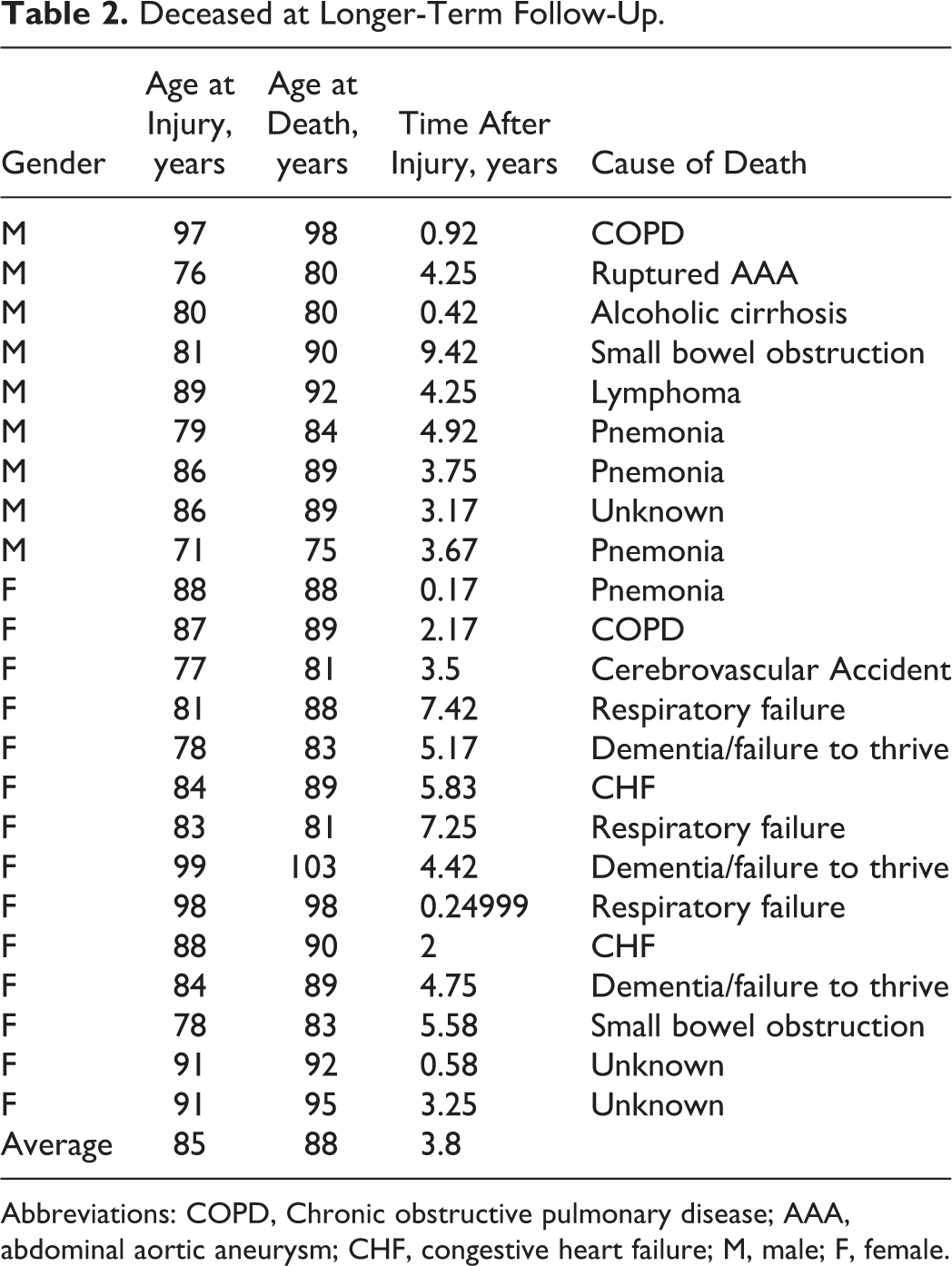
Abbreviations: COPD, Chronic obstructive pulmonary disease; AAA, abdominal aortic aneurysm; CHF, congestive heart failure; M, male; F, female.
The average age at the time of injury was 83 years with a range of 71 to 99 years. In patients who were deceased at longer-term follow-up, there were 9 males and 14 females. The average age at the time of death following an odontoid fracture was 88 years with a range of 75 to 103 years. The average time death occurred after an odontoid fracture was 3.8 years with a range of 0.17 years (2 months) to 9.42 years.
Of the 7 patients who were alive at longer-term follow-up, the average time since injury was 5.75 years with a range of 4.67 to 6.67 years. There were 5 males and 2 females at longer-term follow-up (Table 3). Most recent radiographs confirmed odontoid fracture nonunion in all 7 patients (Figure 1), with 5 (70%) of the 7 having a mobile odontoid nonunion. The 2 patients who achieved a fibrous union were male. Average NDI and VAS scores indicated only mild disability (6.9% and 0.57, respectively). Patient satisfaction with treatment outcomes was high for all patients averaging 9.7 of 10 (Table 3 and Figure 2).

Flexion (A) and extension (B) views 6.17 years after injury in an 86-year-old male with odontoid nonunion. NDI = 28% (mild disability); VAS = 1; satisfaction = 10 no clinical signs of myelopathy. NDI indicates Neck Disability Index; VAS, Visual Analog Scale.
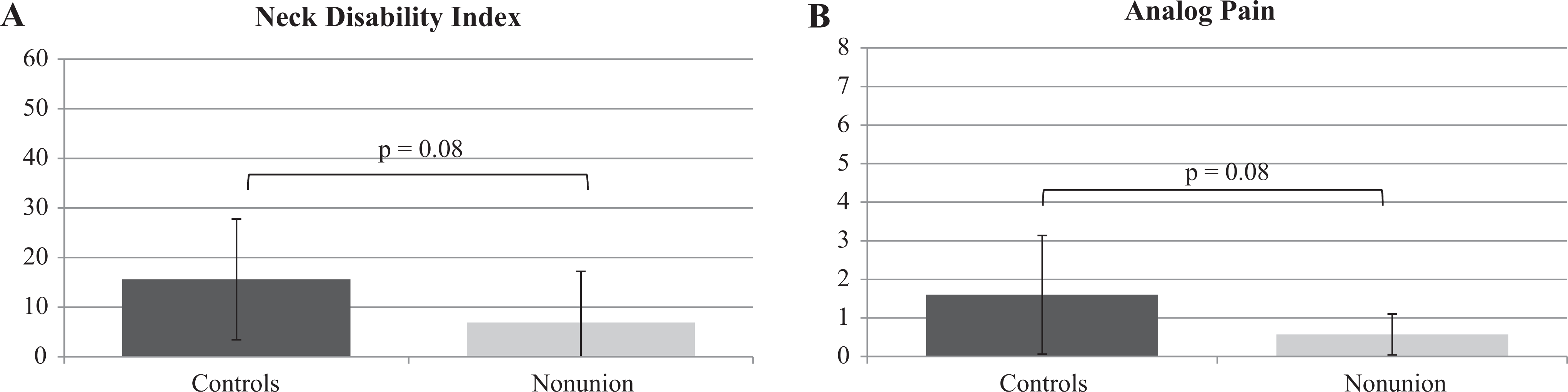
Functional outcomes measured with NDI (A) and VAS (B) at longer-term follow-up compared with age-matched controls. NDI indicates Neck Disability Index; VAS, Visual Analog Scale.
Longer-Term Follow-Up Patients.

Abbreviations: M, male; F, female; NDI, Neck Disability Index.
Functional Outcomes
Neck Disability Index
The NDI scores were used to assess functional outcomes for patients in each group. The NDI is scored using a point scale ranging from 0 to 50 for a raw score and then doubled to obtain a percentage score. 14 A score of 10% to 28% is considered “mild disability”; 30% to 48% is considered “moderate disability”; 50% to 68% is considered “severe disability”; and greater than 72% is considered “complete disability.” 14 The average NDI score for patients with nonunion was 6.9% with a range of 0% to 28%. The NDI scores in the 35 age-matched control group patients averaged 15.6% with a range of 0% to 52%. The 8.7% difference between the 2 groups was not statistically significant (P = .08, t test; Table 3 and Figure 2).
Visual Analog Scale
The amount of pain a patient had was scored using a VAS pain score with a range of 0 (no pain) to 10 (maximal pain). The average pain score for patients with nonunion was 0.57 points with a range of 0 to 1 points. The VAS scores in the 35 age-matched control group patients averaged 1.6 with a range of 0 to 5. The 1.03 point difference between the 2 groups was not statistically significant (P = .08, t test; Table 3 and Figure 2).
Patient Satisfaction
The degree of patient satisfaction with treatment and outcomes was evaluated using an analog satisfaction scale with a range of 0 (no satisfaction) to 10 (maximal satisfaction). Satisfaction scores for patients were high and averaged 9.7 with a range of 8 to 10 (Table 3).
Clinical examination
Seven patients were alive at longer-term follow-up, 5 were available for clinical examination while the remaining 2 had NDI, VAS, and patient satisfaction scores conducted through a phone interview. None of the available patients had any physical examination findings of myelopathy. Chart reviews on the remaining 27 patients did not reveal any diagnosis of myelopathy by any other provider.
Discussion
The incidence of GOFs and elderly cervical spine fractures is increasing due to the worlds aging population. 2,9,11 Outcomes from this injury have shown to have high rates of morbidity and mortality and a poor prognosis regardless of the treatment. 12,15 –24 Studies have described operative fixation of GOFs and have shown high rates of morbidity and mortality. 18,21,25,26 A less invasive treatment with a halo vest has been described with varying success. 11,27 –32 However, due to significant respiratory complications and increased morbidity, halo vests are not recommended in the elderly patients. 3,15,19,25,33 –37
Management of GOFs has long been controversial. 8,13,18,20,21,26,31,38 –49 A recent prospective study by Vaccaro et al 50 demonstrated significantly better NDI and SF-36v2 in patients with GOFs that were treated operatively compared to those treated nonoperatively. 50 A systematic review performed by Robinson et al 43 included 38 articles that met inclusion criteria for GOFs. 43 The researchers found a moderate quality of evidence to support that operative treatment in patients aged 65 to 85 years old improved survival. A low-quality evidence found that nonunion is not associated with worse clinical outcomes, the complication rates were found to be the same between operative and nonoperative treatment, and primary posterior fusion demonstrated the highest bone union rate. 43
Chapman and colleagues 38 performed a retrospective review on 322 consecutive patients treated at 3 different level-1 trauma centers over a 6-year period in patients aged 65 years and older. 38 The 3-month and 12-month mortality for these fractures was high for both surgical and nonoperative groups, with an overall 12-month mortality of 27%. Hospital stays, intensive care unit time, and chances or requiring a feeding tube were statistically higher in the operatively treated patients. There was a trend toward higher long-term survival for the operatively treated group of patients, but this was not statistically significant. The study concluded that surgical treatment did not negatively impact overall survival even after adjusting for age, sex, and comorbidities. 38
Harrop et al 51 performed a systematic review on the topic and found the majority of studies to be of “very low” and “low” quality. Final conclusion was a weak recommendation for operative internal fixation and immobilization for GOFs, strong recommendations for hard cervical collars when treating nonoperatively, and strong recommendations for posterior cervical arthrodesis when operatively treating these fractures.
Fagin et al 52 performed a retrospective review over a 5-year period at a level-1 trauma center on elderly patients with odontoid fractures (age > 60 years) and found similar mortality rates in all treatment groups. Patients were divided into nonoperatively treated, early-operatively treated (<3 days), and late-operatively treated (>3 days) patients. There was no difference in the need for tracheostomy, Percutaneous Endoscopic Gastrostomy (PEG) tube placement, or in the development of Urinary Tract Infection (UTI) or pneumonia between the 3 groups. There was a significant increase in the hospital length of stay as well as the DVT rate in the operatively treated patients. 52
Woods et al 16 performed a retrospective matched cohort study over a 14-year period on geriatric patients (>75 years) with odontoid fractures (types I, II, or III) at 1 institution. Three-month, 1-, and 5-year mortality rates were investigated. There was a statistical increase in mortality in the nonoperatively treated group compared to the operatively treated group at 3 months only (33.3% vs 8.3%, respectively). However, at 1 and 5 years, both groups were found to have the similar mortality rates, specifically in the type II odontoid group. Charlson score had a significant impact on survival in both treatment groups. Of the patients treated surgically, age was significantly a predictor of 1- and 5-year survival. 16
Some literature raises the concern that myelopathy may develop in patients with odontoid fracture and with odontoid nonunion. 40,53 –56 In a retrospective institution database search by Patel et al, 57 it was found that neurologic deficit with type II odontoid fracture was as high as 9.6%. Kepler et al 56 performed a retrospective case series of 133 consecutive patients over a 5-year period with type II odontoid fractures. They found that 30% of acute fractures were actually “acute-on-chronic” injuries from an odontoid nonunion. Of these patients, 17.5% presented with a neurologic injury. The authors suggested that definitive fracture stabilization at the time of initial injury could have prevented severe neurologic injury from the secondary trauma in 17% of patients. Others have found neurologic deficits with type II odontoid fractures ranging from 3.4% to 13%, suggesting a relatively benign outcome from odontoid nonunion.” 18,40,58,59
In our series of 7 patients, there were no signs of myelopathy at longer-term follow-up on clinical examination of the 5 patients. In addition, chart reviews of all 34 patients did not reveal any diagnosis of myelopathy by other providers. These results are similar to that of Hart et al. 45 Hart et al study was a retrospective review of 5 elderly patients with chronic odontoid mobile nonunion. The average age at the time of injury was 81 years, and the average follow-up was 4 years and 7 months, with 1 patient having died from a myocardial infarction after hip fracture surgery. At long-term follow-up, none of Hart et al patients were found to have symptoms or examination findings of myelopathy or nerve injury. 45
Our results suggest that nonoperatively treated patients can have similar functional outcomes compared to age-matched controls. In addition, patient satisfaction was very high at longer-term follow-up. Cervical collar immobilization has been used in the geriatric population for upper cervical spine fractures with inconsistent results. 17,19,32,34,46,60 Reported nonunion rates with nonsurgical management of GOFs vary greatly from 35% to 85%. 13,17,39,46,59,61 –63 Our higher rate of nonunion when compared to other studies could be related to our older age patients (>70 years) or to our strict definition of union (no visible residual fracture line). No study to our knowledge exists describing the longer-term functional outcomes of patients treated nonoperatively in whom a nonunion has occurred. 3,53 Rigid cervical collars are simple to use, noninvasive, relatively inexpensive, and have few device-related complications. 13,64,65
Our study did have limitations. Our patient size was small, and long-term follow-up was difficult to obtain. This was due to the known high mortality associated with GOFs at long-term follow-up. We were also unable to determine the exact causes of death for 3 patients who were known to be died; in addition, 4 patients were lost to follow-up, comprising a total loss of follow-up of 20.6% (7 of 34 patients). Only 7 of the original 34 patients were available or alive for longer-term follow-up, demonstrating a 20.6% follow-up rate. Having such small numbers of follow-up makes statistical analysis difficult. Determining nonunion is also not an exact science when using plain radiographs, and some authors recommend using computed tomography as the study of choice to assess for nonunion. 66
Conclusion
Type II geriatric odontoid fractures are increasing in incidence with our globally aging population. Rigid cervical collar use appears to be a viable treatment option for minimally displaced fractures. Early and aggressive ambulation to minimize pulmonary and other medical complications following these fractures can be undertaken while treating these fractures nonoperatively. Odontoid nonunion is high in this treatment group. There does not appear to be any catastrophic neurologic complications in this patient population at longer-term follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.