
Abstract
Introduction:
Thoracolumbar spine fractures are common osteoporotic fractures among elderly patients. Several studies suggest that these fractures can be treated successfully with a nonoperative management. The aim of this study is to evaluate the conservative treatment of elderly patients with a vertebral fracture.
Methods:
This study is a retrospective cohort study, which included all patients with an age of 65 years and older, who were diagnosed with a vertebral fracture and where therefore admitted to the Geriatric Fracture Center over a period of 2 years. Primary outcome was the level of functioning 6 weeks and 3 months after admission.
Results:
We included 106 patients with 143 vertebral fractures, of which 61 patients were evaluated after 3 months. In our population, 53% of the patients had a fracture involving both middle and anterior columns. The majority of the patients functioned sufficiently 6 weeks and 3 months after admission. Analysis showed that age <80 years is an independent predictor of a sufficient level of functioning after 6 weeks.
Discussion:
The nonoperative treatment of elderly patients with a vertebral fracture leads to a sufficient level of functioning 6 weeks and 3 months after admission. In our population, only age <80 years is an independent predictor for a sufficient level of functioning 6 weeks after admission. The level of functioning at 6 weeks predicts the level of functioning 3 months after admission. On comparison, the level of functioning after early ambulation is equal to the level of functioning after immobilization. Where immobilization may lead to complications, early ambulation was not associated with new complications or neurological damage. Based on these advantages, the treatment of elderly patients with a fracture involving both middle and anterior columns may be altered from immobilization to mobilization in the future.
Introduction
Vertebral fractures are, together with proximal femoral and wrist fractures, the most common osteoporotic fractures among elderly patients. The number of fractures detected in people older than 55 years of age on radiological examinations is 15.970 annually. The incidences of the fractures are 2 of 1000 in males and 7 of 1000 in females. 1
The majority of these fractures are situated in the thoracolumbar spine, from the 10th thoracic vertebra to the 4th lumbar vertebra. 2 Previous research showed that vertebral fractures are associated with an increased level of morbidity and mortality. 3 –5
Isolated fractures of the anterior column are usually treated by early ambulation. At this moment, no clear guidelines exist for fractures which also involve the middle column. 6 Previous research showed that a nonoperative treatment gives the same result with regard to the level of mobility compared to an operative treatment. 7 –13 Several studies also suggest that a nonoperative treatment, immobilization, followed by delayed ambulation with the use of a brace when necessary, is a safe and successful treatment for fractures involving the middle column. 7 –9
Damage to the middle column is crucial to determine the treatment strategy, immobilization in case of damage to the middle column, and mobilization when only the anterior column is involved. It has been established that the computed tomography (CT) scan is the appropriate device to detect damage to the middle column. 14,15 Therefore, the detection of middle column damage on CT images is crucial in the diagnostic process and determines the type of treatment.
In our practice, we observed that immobilization is accompanied with problems such as pneumonia, which is a potentially lethal complication. These problems often force us to a change in treatment from immobilization to early mobilization, apparently without negative side effects. We want to investigate the consequences of these changes regarding the level of mobility and the occurrence of neurological and other complications. Furthermore, we want to explore which factors contribute to a level of mobility after hospital treatment for vertebral fractures among the elderly patients.
The aims of this study are to evaluate the conservative treatment of elderly patients with a thoracolumbar spine fracture and to identify factors that influence the level of mobility after treatment.
Methods
Study Design
This study is a retrospective cohort study, which included all patients with an age of 65 years and older, who were diagnosed with a vertebral fracture and were therefore admitted to the Geriatric Fracture Center (GFC). The GFC is part of the Surgical Department of the hospital ZGT, Almelo, the Netherlands.
All patients were recruited between January 1, 2009, and December 31, 2010. Exclusion criteria were cervical spine fractures, fractures that needed operative treatment, and patients who were transferred to another hospital. The indication for surgical treatment was made after consultation of an expert center. Decisions were made based on the radiologic imaging, that is, a 3-column fracture was an indication for operative treatment. Although vertebroplasty is an operative procedure, we did regard it not as an operative procedure for meeting our exclusion criteria but as a less invasive instrument to facilitate mobilization. The duration of the follow-up varied from 6 weeks to 3 months after admission. Patients lost to follow-up were excluded from the analysis, regarding functional outcomes at the respective moments of follow-up.
This study took place in the GFC. We provide multidisciplinary care, registered in clinical pathways, from admission until the follow-up in the outpatient clinic, which has proven to result in fewer complications, a significant decrease in readmissions, and gets patients in a better condition at the moment of discharge. 16,17
Variables
We registered the following demographic variables of all patients: age, gender, comorbidity based on the Charlson Comorbidity Index (CCI), and number and location of the fractured vertebras. 18,19
The CCI is an index, which scores the burden of comorbidity based on different conditions. Each condition has his own score, based on the relative mortality risk in 1 year, and the CCI is an accumulation of these scores. The relative risk of mortality in 1 year can be classified as low, intermediate, and high based on the CCI. A CCI of 3 or more is considered to be a high risk of 1-year mortality.
Patients were initially treated by either immobilization with strict bed rest or early mobilization. Mobilization took place with or without a brace depending on the level of the fractured vertebra and comfort of the patient. When a patient went from immobilization to ambulation, this was regarded as a change in treatment policy.
Neurological examination was performed at admission, on daily basis at the ward visits and when the patient was discharged. The examination was carried out by emergency residents, surgical residents, or nurse practitioners.
Our primary outcome is the level of mobility 6 weeks and 3 months after admission. The level of mobility is determined by the New Mobility Score developed by Parker and Palmer. 20 A score of 0 indicates the impossibility of mobilizing independently, while a maximum score, 9, indicates a complete independent state of functioning. A score of ≥6 indicates a sufficient level of mobility of an independently living patient.
Our secondary aim is to identify factors that influence the level of mobility. To identify these factors, we registered the type of treatment, involvement of the middle column, compression rate of the vertebral body, diameter of the spinal canal, existing comorbidity, and the level of mobility at admission. The involvement of the middle column, compression rate, and spinal canal diameter were determined by a trained radiologist using CT imaging of the spine.
Statistical Analysis
Factors related to a sufficient level of mobility, the ability to function independently after a vertebral fracture, where identified using a univariate analysis with use of the chi-square (χ2) test. To identify factors predicting a sufficient level of mobility, we performed a multivariate analysis (logistic regression), including all factors related to the level of mobility with a P < .10 in the univariate analysis. Analysis was performed with the use of SPSS for Windows version 17.0 (SPSS Inc., Chicago, IL, USA). The level of significance in all analyses was P < .05.
Results
From January 1, 2009, until December 31, 2010, 117 patients with a vertebral fracture were admitted to our hospital. We included 106 of them in our study. The inclusion is shown in Figure 1.

Inclusion scheme.
Demographics
Baseline characteristics of the patients are shown in Table 1. We included 106 patients with 143 vertebral fractures. Most of these fractures, 77%, were located in the thoracolumbar junction and the range of vertebra involved is shown in Figure 2. Majority (76%) of the fractures were due to a low-energy trauma. In 5%, a high-energy trauma caused the fractures, and 21% of the patients developed a fracture without any prior trauma. The majority (72%) of the patients had a sufficient level of mobility at admission. In 3 patients, a preexistent isolated nerve peroneus lesion was present at the time of admission. There were no new neurological deficits in any of the patients.

Distribution of involved vertebrae
Baseline Characteristics.

Abbreviations: CCI, Charlson Comorbidity Index; NMS, New Mobility Score.
a Based on the Charlson Comorbidity Index. 18
b Based on the New Mobility Scale. 20
c After changes during the admission.
A complication was registered in 67% of the patients. Most common complication was the development of a delirium (17%). Other complications were pulmonary complications (9%), urinary tract infections (9%), and surgical site infections (7%).
During our study, the in-hospital mortality was 2%. The 30-day mortality reached 6%. During the 3-month follow-up, 12 (11%) patients died with a 1- year mortality of 14%. The cause of death was unknown in most cases, 1 patient died of a cardiac arrest and 1 patient died on the consequences of a polytrauma.
A total of 18 (17%) patients did have a history of osteoporosis prior to the fracture; all patients were treated for the osteoporosis. Treatment of osteoporosis is part of the treatment for vertebral fractures. Therefore, all patients who were not evaluated for osteoporosis prior to the fracture did get an invitation for osteoporosis screening and dual-energy x-ray absorptiometry scan.
A total of 67 patients responded to this invitation. The T-scores varied between −4.9 and +2.0, range −2.9. Based on the National Guidelines Osteoporosis (revised version 2011), all patients aged 50 years and older, with a vertebral fracture detected in the x-ray at the emergency department, were treated with calcium, vitamin D, and a bisphosphonates. Accumulating screening prior or after fracture, 85 (81%) patients underwent screening and treatment for osteoporosis.
Radiological Characteristics
In our population, 53% of the patients had a fracture involving both middle and anterior columns. A CT scan was performed in 78% of the patients. From the patients who did not underwent a CT scan, 3 patients underwent a magnetic resonance imaging. The other patients underwent evaluation by conventional x-ray images. An additional CT scan was not performed because the fracture existed a couple of days, patients delay on visiting the emergency department, and only a very minimal impaction of the anterior column on the x-ray evaluation.
In most cases, the anterior wedge was more than 30%. In 50% of the patients, the central depression was more than 30%. The posterior depression was relatively small, less than 15% in the majority of the patients. The Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification following the AO Spine guidelines was an A-type fracture in all cases. Most of the patients with isolated anterior column damage did have an A0 or A1 fracture. In patients with both anterior and middle column evolvement, A2 and A3 fractures were present. 21 A complete overview of all radiological measures is shown in Table 2.
Radiological Characteristics.a
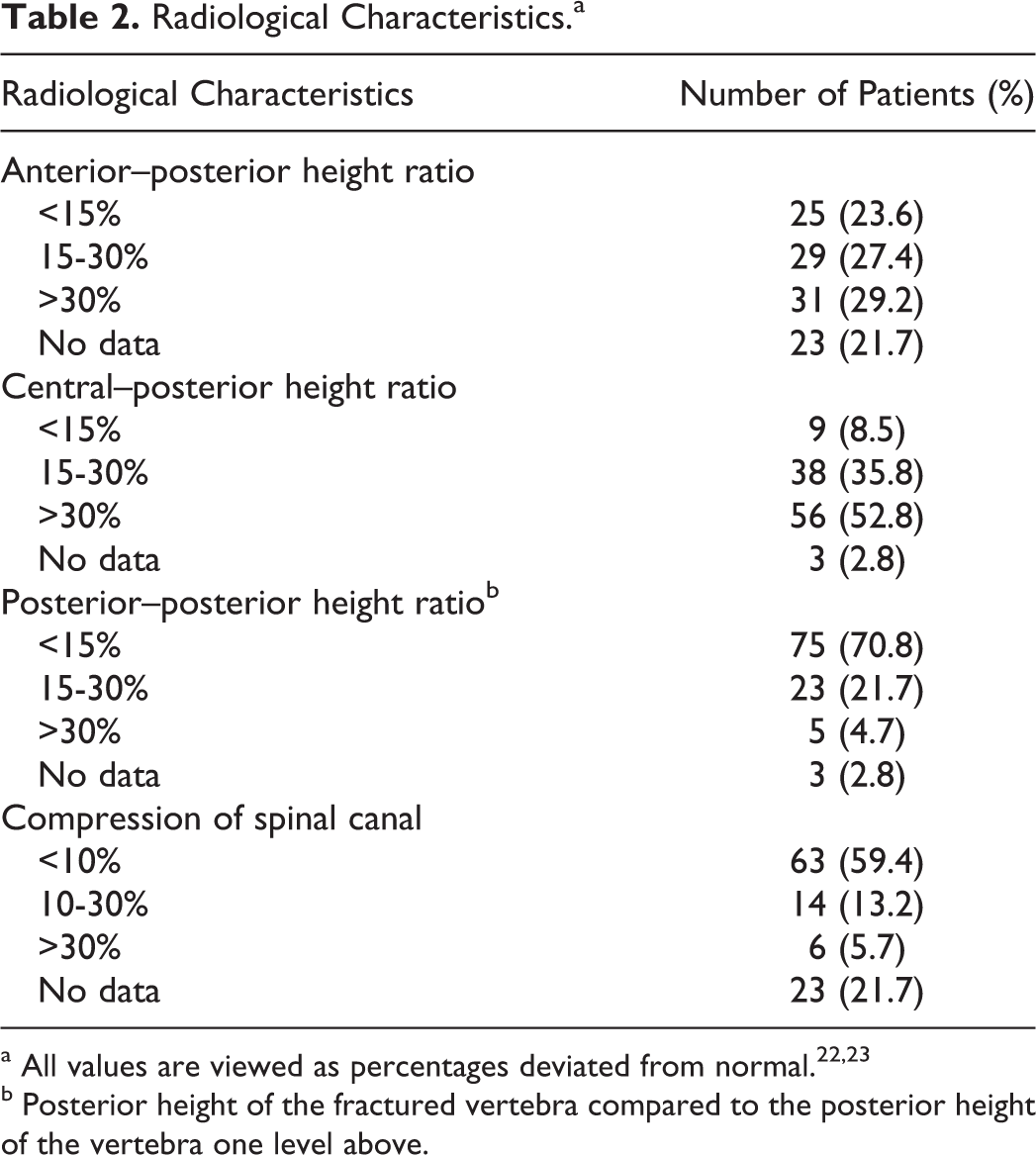
b Posterior height of the fractured vertebra compared to the posterior height of the vertebra one level above.
Changes of Policy
In general, our policy is early ambulation in patients with an isolated anterior column fracture. Early ambulation is defined as quick mobilization facilitated by use of pain medication and support of a physical therapist. This was applied in most of the patients, 60%. For the other patients, the initial treatment was immobilization, used as a temporary measure for further analysis of the fracture. In 14 of the 19 patients, the immobilization was changed to early ambulation when diagnostic results became available. Early ambulation was applied to 88% of the patients with an isolated anterior column fracture.
In our population, patients with an anterior and middle column fracture, 96% was initially treated with immobilization. In this group, a change in the treatment occurred in 83% of the patients. The treatment was changed from immobilization to early ambulation. Early ambulation as final treatment was applied to 84% of the patients. Reasons to change the treatment policy were results of additional analysis proving the fracture to be stable, second opinion, or complications related to bed rest. There were various reasons not to treat patients with early ambulation instead of immobilization such as preexistent pulmonary or cardiologic impairment or patients who were immobile at the time of admission.
In 3% of the patients, a vertebroplasty was performed to facilitate mobilization. Progressive kyphosis requiring surgical intervention was not recorded. No patients underwent operative procedures regarding the vertebral fracture during the 3-month follow-up.
The majority of the complications we registered occurred in patients who were treated with immobilization (80%). After the change to early ambulation, no new complications occurred, and no neurological damage was registered.
Primary Outcome: Level of Mobility
We determined the level of mobility at 6 weeks and 3 months after admission. The majority of the patients showed a sufficient level of mobility at these times. The results are displayed in Table 3.
Level of Mobility and Factors Predicting the Level of Mobility.

Abbreviations: CI, confidence interval; NS, nonsignificant (P > .05); RR, relative risk UV: univariate analysis, MV: multivariate analysis (cox regression).
Factors Related to a Sufficient Level of Mobility
Univariate analysis showed that age, level of comorbidity, immobilization, and level of mobility at admission are related to the level of mobility after 6 weeks. Multivariate analysis showed that age <80 years is an independent predictor of a sufficient level of mobility after 6 weeks.
For the level of mobility after 3 months, a sufficient level of mobility 6 weeks after admission predicts a sufficient level of mobility. No independent predictor was found in multivariate analysis. All significant factors included in the analysis are shown in Table 3.
Discussion
The nonoperative treatment of elderly patients with a vertebral fracture leads to a sufficient level of mobility 6 weeks and 3 months after admission. In our population, only age <80 years old is an independent predictor for a sufficient level of mobility 6 weeks after admission. The level of mobility at 6 weeks predicts the level of mobility 3 months after admission.
The level of mobility after early ambulation is equal to the level of mobility after immobilization. Where immobilization may lead to complications, early ambulation was not associated with new complications or neurological damage.
Based on these advantages, the treatment of elderly patients with a fracture involving both middle and anterior columns can be changed from immobilization to early ambulation. Therefore, the diagnosis of middle column damage by CT scan becomes less relevant in determining the treatment policy. Consequently, a diagnostic protocol with a limited role for CT imaging in elderly patients with a thoracolumbar spine fracture may be possible.
Limitations
The most important limitation is the number of patients lost to follow-up. Of the 106 patients included in our study, 58% proceeded to the follow-up 3 months after admission. This loss is partially explained by the number of patients who died during the follow-up. A total of 15 patients died, which correlates with 30% of the people lost in the follow-up. Analysis showed that the majority of the patients lost to follow-up are the patients with the best and worst levels of functioning. Therefore, our analysis excludes the extremes of both sides of the spectrum, and our results can be applied to the average patient with a vertebral fracture. We expect that a reanalysis of our data including the patients who are lost to follow-up due to these reasons would not lead to other results.
Another limitation is the duration of the follow-up. We evaluated only the levels of functioning shortly after the admission. To draw conclusions about the effects on a longer term follow-up, a longer period is needed.
An additional restriction is the use of the Parker Mobility Scale to evaluate the level of mobility. A validated questionnaire for elderly patients with a vertebral fracture is not available but the use of a more common questionnaire could have made comparison between studies more easier.
Interpretation
We saw that a nonoperative treatment of elderly patients with a thoracic or lumbar vertebral fracture leads to a sufficient level of mobility. This observation is stated by the results from the previous studies. 7 –13 These studies have shown that nonoperative treatment gives results comparable to operative treatment with regard to the level of mobility and the degree of pain reduction. 24,25 These studies also stated that most of the people could return to work after a period of time. This is comparable with our finding that the majority of the elderly patients with a vertebral fracture return to a sufficient level of mobility. Although the majority of our patients does not have a job anymore, after the conservative treatment, they are able to return to prefracture activities of daily living.
Our finding that age <80 years predict a good level of mobility 6 weeks after admission has, as far as we are aware, not been reported in the literature before. We pointed out that the prolonged immobilization in elderly patients with a vertebral fracture with middle column damage is often changed to mobilization.
Most of the changes in treatment policy occurred with patients with immobilization. Treatment was mostly changed from immobilization to ambulation. These changes were mostly made in cases where patients had fractures through both the anterior and the middle column. The majority of these patients regained a sufficient level of mobility. The finding that early ambulation leads to results comparable to those after prolonged immobilization is also stated by the results of Cantor et al and Mumford et al. 7,8
The level of mobility after early ambulation is an important outcome. An outcome that is equally important is the safety of early mobilization of elderly patients with a vertebral fracture.
Our data showed that immobilization leads to complications. More than 50% of the patients with immobilization had a complication, mostly pneumonia or severe pain when lying down. After the change in the treatment, we did not record new complications. The complications that already existed, like a pneumonia, were treated in the same way as during the period of immobilization. The patients recovered from all existing complications during the period of mobilization.
Furthermore, we did not register any neurological deterioration. This is remarkable because a patient with middle column damage has an increased risk of nerve damage. With these findings in mind, the advantages of mobilization over the complications associated with immobilization, we suggest that early mobilization is a safe alternative for immobilization in the conservative treatment of elderly patients with vertebral fractures.
The most important use of the CT scan is to determine the stability of the fracture by determining middle column damage because fractures with involvement of the middle column are potentially unstable. 14,15
In our study population, we found that middle column damage does not have to lead to immobilization but can safely be treated with ambulation. Therefore, determining the damage to the middle column as a single parameter becomes less important. Since the value of the CT scan as we use it now seems to be restricted, the use of the CT scan of elderly patients with a thoracic or lumbar spine fracture may be changed. The integrity of the posterior wall of the vertebral column can become more important and may be the crucial point in the future to decide whether operative stabilization is needed or whether the conservative treatment, with early mobilization, may be the treatment of choice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.