
Abstract
Fragility fractures of the distal humerus in elderly patients, especially the low transcondylar fracture pattern, can be difficult to optimally manage. Although the fractures are typically low energy resulting in either extra-articular or simple intra-articular patterns, gaining fixation into the distal fragments can be difficult with open reduction internal fixation (ORIF) using traditional 90-90 or parallel plating techniques. Anatomy preserving reconstruction with ORIF is preferred over total elbow arthroplasty (TEA) if possible. In this study, 15 patients were managed with a bicolumnar 90-90 plating construct as a novel method of enhancing distal fixation in these fractures. Fourteen patients went on to radiographic union at an average of 77 days after surgery with an average arc of motion of 105°. One patient was lost to follow-up. Bicolumnar 90-90 plating of distal humerus fractures in elderly patients may represent a viable alternative to traditional ORIF or TEA.
Background
Fragility fractures of the distal humerus in the elderly patient population 1 are typically the result of low-energy trauma resulting in extra-articular or simple intra-articular variants. However, these injuries are infamously difficult to optimally manage. 1 The low transcondylar pattern with or without intra-articular extension is the typical fracture variant with or without a joint extension (Figure 1). Operative reconstruction is the standard of care for the active geriatric patient, yet it is complicated by complex native anatomy, osteopenic bone quality, and the diminutive nature of the distal fragments. 2 –4 Whether best care practice is open reduction internal fixation (ORIF) or total elbow arthroplasty (TEA) is controversial. 5 Anatomy preserving reconstruction is preferable if feasible. 2

Preoperative radiographs depicting characteristic distal humeral fracture pattern seen in geriatric population.
Open reduction internal fixation of fragility fractures involving the distal humerus presents unique operative challenges. Achieving and maintaining adequate fixation in the distal articular segment are the primary determinant for success or failure. 6 –8 Recent advancements in treatment protocols including technique and the use of minifragment implants have improved union rates but risk of hardware failure remains considerable. 3,9 –11 As such, TEA has been suggested as a viable alternative for ORIF in this patient population. 12 –14 However, complication rates with TEA are also concerning and revision options are limited. 15 –18
The purpose of this report is to present our technique for ORIF of distal humerus fractures using bicolumnar 90-90 plating. Our hypothesis was that multiple points and planes of fixation into the short distal segments will optimally maintain alignment to facilitate union and aggressive rehabilitation. Our primary outcome measures were time to fracture consolidation and elbow function.
Methods
Between 2006 and 2012, patients surgically managed at our institution for fragility fracture of the distal humerus were reviewed for inclusion in the study. Criteria for fragility fracture included age, mechanism of injury, history of osteopenia/osteoporosis, and/or diagnostic fracture pattern (ie, low transcondylar). No formal bone density measurement, however, of the patients was required for inclusion in the study.
All patients were operatively managed by a fellowship-trained orthopedic traumatologist. Posterior exposure was performed with the patient in lateral decubitus position under general anesthesia. The triceps musculature was respected in all cases using paratricipital exposures. 19 Olecranon osteotomy was only utilized in cases with extensive articular comminution. 20 Anatomic reduction was achieved in all cases using principles popularized by Dr Morrey. 21 Definitive fixation was then attained using a combination of small fragment (3.5 mm) and minifragment (2.0, 2.4, and 2.7 mm) standard and/or fixed-angle plates. Both the lateral and the medial columns were instrumented with typically 4 plates (2 on each column). Plate placement included direct medial and lateral as well as posteromedial and posterolateral creating multiple points/planes of fixation into the diminutive distal segments (Figure 2). The ulnar nerve was identified and protected, however was not routinely transposed. A bulky soft splint was applied at the end of the case and remained in place until the first postoperative visit 10 to 14 days after surgery. After suture removal, full elbow motion was allowed with a 5-pound weight restriction. Radiographic and clinical data were analyzed (Figure 3). Fracture union was defined as bridging bone on 3 of 4 cortices using orthogonal radiographs. Functional data included elbow range of motion and local symptoms. All patients were followed at least until fracture healing and uneventful rehabilitation.

Intraoperative photo demonstrating representative fixation of distal humeral fracture.

Postoperative radiographs depicting 90-90 bicolumnar plating construct for internal fixation utilized at our facility.
Results
Of the 109 patients with a distal humeral fracture treated at our institution during the study period, 15 met our inclusion criteria for this report. There were 7 male and 8 female patients with an average age of 71 years (range 59-95). The mechanism was primarily low-energy trauma including a ground-level fall in 13 patients, a fall down steps in 1 patient, and a 6-ft fall in 1 patient. There were 3 AO-type A2, 7 type C1, 4 type C2, and 1 type C3 fractures. Two of the patients treated had open fractures. A triceps-reflecting approach was used in 10 of the 15 patients, while an olecranon osteotomy was performed in 5 patients.
All patients went on to union at a mean of 77 days after surgery (range 44-124). Average arc of motion was 105° (range 70-140). There were no cases of hardware failure. One patient developed irritation secondary hardware and was taken for removal once union was achieved. There was 1 case of an ulnar nerve palsy identified preoperatively for which the patient underwent ulnar nerve decompression at the time of index surgery and subsequently recovered function. One patient had problems with chronic pain at the elbow that was still present at most recent follow-up. These data are summarized in Table 1.
Summary of Demographic and Clinical Data for Dual 90-90 Plating Construct for Distal Humerus Fractures in Elderly Patients.
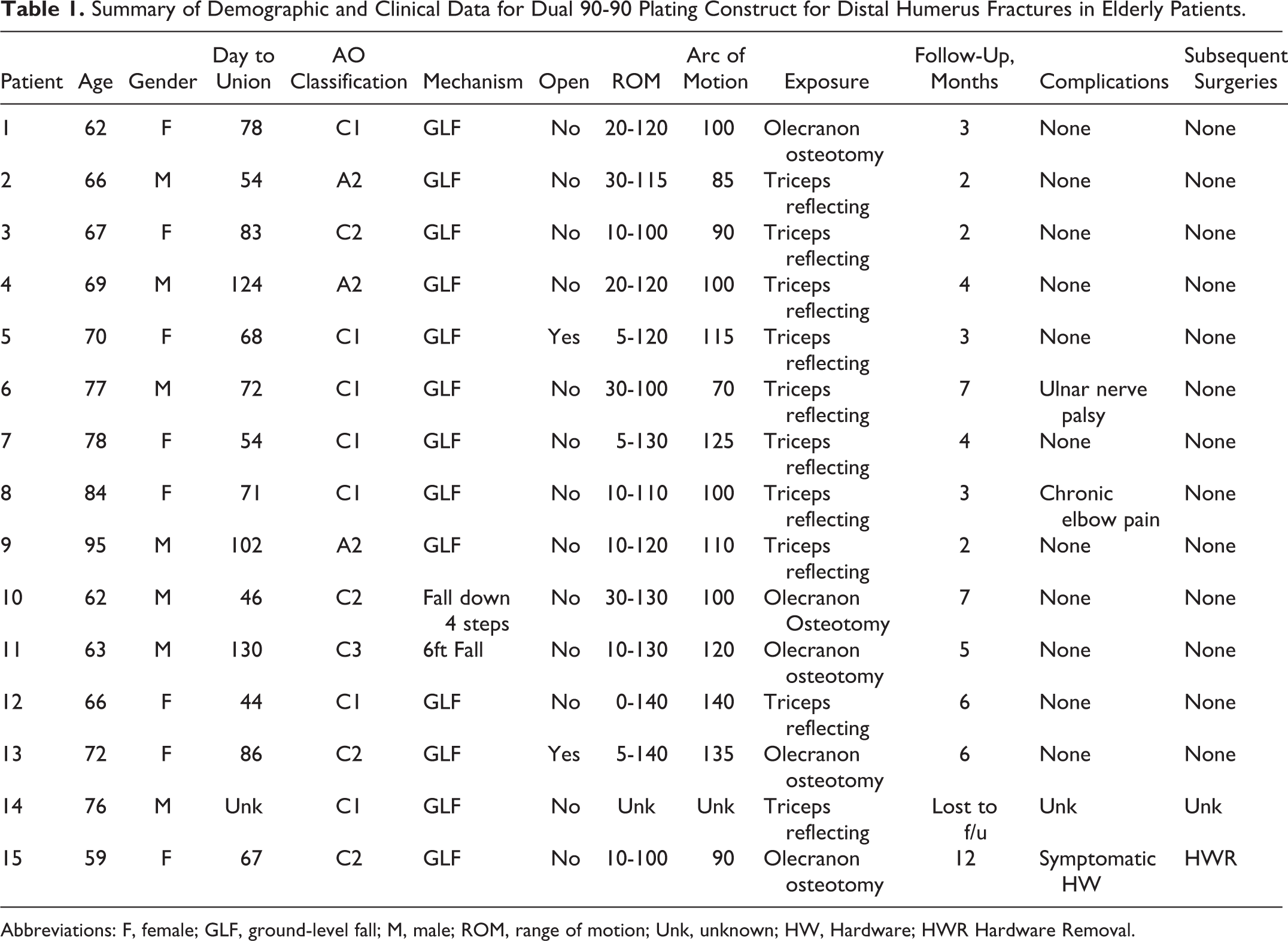
Abbreviations: F, female; GLF, ground-level fall; M, male; ROM, range of motion; Unk, unknown; HW, Hardware; HWR Hardware Removal.
Discussion
Geriatric fragility fractures of the distal humerus can be successfully treated with bicolumnar 90-90 plating. These cases are typically low energy with the transcondylar pattern with or without simple intra-articular split being the most common. Multiple points of fixation in different planes into the diminutive osteopenic short distal segments provide optimal construct rigidity to foster uneventful fracture union and early rehabilitation. 22 Usage of both small and minifragment fixed-angle plate fixation is well suited for this anatomical location. 9
Traditionally, the care paradigm for distal humeral fracture fixation has consisted of dual column plating. 11 Either orthogonal or parallel plating has resulted in acceptable outcomes. 10,23,24 Further, both small and minifragment fixation are the implants of choice for this application. 9 The geriatric fragility fracture, however, deserves a different approach. Standard protocol is fraught with an unacceptably high rate of complications including nonunion and hardware failure. 11,25 Bone quality and fracture pattern (low transcondylar) seen in the older patient population challenge the current care paradigm, prompting the establishment of a new technique for these cases.
Korner et al studied 45 elderly patients with distal humeral fracture concluding that ORIF with traditional bicolumnar plating was unreliable as compared to younger patients with similar fracture patterns. They noted that achieving/maintaining fixation into the distal segment was challenging. They reported a “remarkably high” rate of complications including a nearly 30% rate of hardware failure or loosening due to unreliable distal fixation. 11
Morrey et al recently presented their results after surgical management of elderly patients with transcondylar distal humeral fractures. In the 11 patients treated with ORIF, the complication rate was 43% including 2 frank nonunions. They concluded that TEA should be considered in the low demand, elderly patients with very challenging fracture pattern and osteoporosis. 26
Frankle et al compared results of distal humeral fracture in women older than 65 years of age using ORIF versus TEA. The fixation failure rate in the 12 patients treated with ORIF was 25%. However, the overall complication rate after TEA was 25% as well, suggesting that best care for these injuries needs to be individualized to the host and injury pattern. 12
Considering the previously reported complications related to ORIF for fragility fracture of the distal humerus, TEA seems to be a reasonable reconstructive option. The TEA has been shown to provide significant pain relief and reasonable restoration of function in this patient population 27 ; however, devastating complications have been reported including aseptic loosening, periprosthetic fracture, and infection. 17,18,28 –31 Salvage after failed TEA is not always possible and flail elbow, arthrodesis, and amputation are often in the treatment algorithm in this scenario. Even if these complications are avoided, patients with a TEA are limited by weight-bearing restrictions of 5 to 10 lbs indefinitely. Because of these issues, acute TEA may be best utilized as a salvage procedure in fractures that are not amenable to internal fixation. 32
Given the limitation of traditional ORIF and TEA, our new technique of 90-90 bicolumnar planning may be best care for these injuries in selected patients with fragility fracture of the distal humerus requiring multiple points of fixation in the distal fragment in multiple planes. Our union rate was optimal with preserved elbow functionality. Certainly, our study has limitations including retrospective design with limited patient numbers, absence of a control group as well as selection bias. Yet, these results are promising.
Footnotes
Authors’ Note
This study is institutional review board approved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.