
Abstract
Purpose:
We propose that geriatric comminuted intra-articular distal humerus fractures can be effectively treated with a limited fixation approach aimed at achieving varus/valgus stability with columnar fixation, but allowing intra-articular comminution to heal by secondary congruency against an intact olecranon, thus avoiding an olecranon osteotomy.
Methods:
Fifty-six elderly patients with AO 13-C type fractures, who underwent surgical fixation with ≥12-months of follow-up were retrospectively reviewed. Thirty patients were treated with intra-articular open reduction internal fixation (ORIF) with an olecranon osteotomy and 26 patients were treated with our limited fixation (L-ORIF) approach. Outcomes were range of motion (ROM), complications, additional surgery, and patient-reported outcome measures (PROMIS).
Results:
At final follow-up, the average elbow ROM was 97° (40°-155°) in the ORIF group and 86.5° (20°-145°) in the L-ORIF group. There was a trend toward more complications and additional surgery in the ORIF group. PROMIS scores for pain were 53.1 and 52.14, and PROMIS functional scores were 41.7 and 41.4 in the ORIF and L-ORIF group respectively. No differences in outcomes were statistically significant.
Conclusion:
A limited fixation technique based on achieving varus/valgus stability with columnar fixation, demonstrated equivalent outcomes in elderly patients with intra-articular distal humerus fractures when compared to intra-articular ORIF with an olecranon osteotomy
Introduction
Intra-articular distal humerus fractures with trochlear comminution in the elderly are disabling injuries which are commonly treated with open reduction internal fixation (ORIF) via an olecranon osteotomy. Acute total elbow replacement is also an option. Additionally, in select older patients who are medically unwell, non-operative treatment, often referred to as the “bag of bones” approach, 1 can facilitate early rehabilitation without the risks of operative intervention, though this method can be associated with poor functional outcomes, instability, pain, distorted distal humerus geometry, and joint dysfunction. 2 -10
ORIF and total elbow arthroplasty can achieve good results with regard to final elbow range of motion, function, and pain for elderly patients with intra-articular distal humerus fractures. Formal open reduction and internal fixation can be challenging in the geriatric population where poor bone quality and fracture comminution can make achieving and maintaining anatomical reduction of the joint surface difficult at best. An olecranon osteotomy also disrupts the extensor mechanism of the elbow and creates an iatrogenic fracture plane that can go on to delayed healing or non-union. This complication could further preclude total elbow arthroplasty as a future salvage option. Additionally, olecranon hardware has a high rate of hardware prominence and pain, often requiring a second procedure for removal. 11 While initially thought to be a good option for comminuted distal humerus fractures, acute total elbow arthroplasty in this patient population has also been shown to be associated with a high rate of failure and re-operation. 12
This study aims to compare outcomes of elderly patients with intra-articular distal humerus fractures treated in 2 different ways: a) with traditional ORIF of the distal humerus with an olecranon osteotomy and an effort to treat any trochlear comminution with intra-articular anatomic reduction and fixation, and b) a limited fixation technique focused on achieving varus/valgus stability by columnar fixation only through a paratricipital approach without an olecranon osteotomy for anatomic joint reconstruction. This limited fixation approach allows intra-articular comminution to heal in secondary congruency to an intact olecranon, without open reduction of the frail articular fragments in these osteoporotic patients. Our hypothesis was that there would be no significant clinical differences with regard to pain, function, or final range of motion between the 2 groups.
Materials and Methods
Approval to conduct this study from our Institutional Review Board was obtained prior to subject enrollment. The design was a retrospective cohort study to evaluate the clinical outcomes of patients (≥ 65 years old) with humeral AO/OTA 13-C type fractures, who were treated with ORIF. Patients who underwent surgical fixation with a traditional ORIF with an olecranon osteotomy or with our limited fixation technique over a 12-year period from July 1st, 2005 to July 1st, 2017 at a single orthopaedic trauma center were eligible for enrollment. Patients had a minimum of 12-months of follow up.
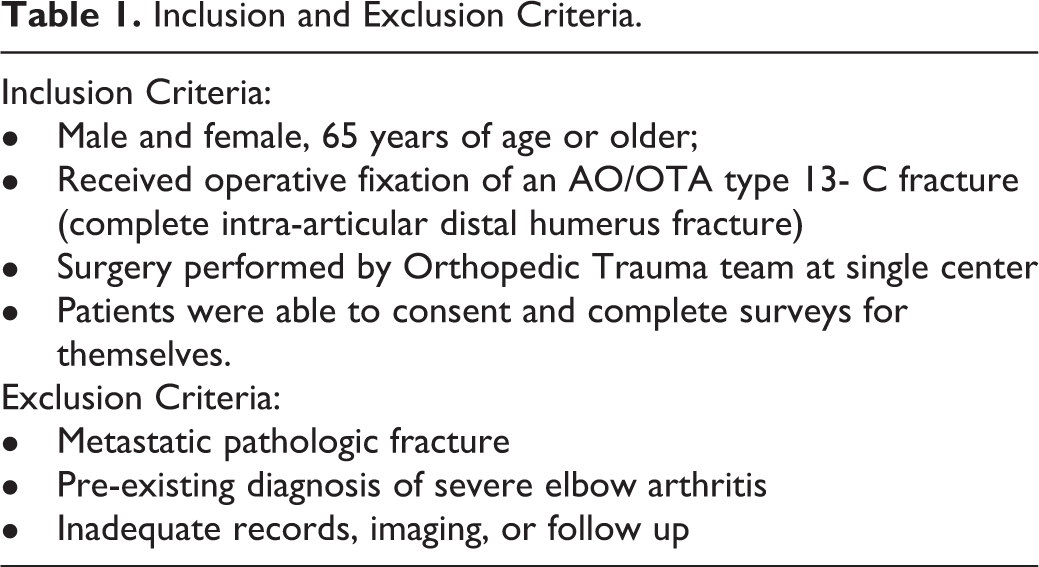
Patients in the ORIF group were treated with intra-articular ORIF with an olecranon osteotomy, patients in the limited fixation (L-ORIF) group were treated with columnar plating without an olecranon osteotomy. Table 1 outlines the inclusion and exclusion criteria for the study and Table 2 summarizes the baseline demographic and injury characteristics. Within the study period, a total of 56 patients met inclusion criteria and were enrolled. Thirty patients made up the ORIF group and 26 patients were in the L-ORIF group. The 2 groups were not statistically different (p < 0.05) with respect to any demographic variables listed in Table 2.
Inclusion and Exclusion Criteria.
Summary of Baseline Demographics and Injury Characteristics.

BMI = Body mass index, ASA = America Society of Anesthesiologists
Surgical Technique
In all cases, patients were positioned in the lateral-decubitus position, with the injured side up, utilizing a triangle on a mayo stand to support the operative extremity. The anesthetic modality was general anesthesia with or without block supplementation. Preoperative blocks were offered to facilitate general anesthesia and offer post-operative pain control. Without use of a tourniquet, a midline posterior approach to the elbow was utilized. Full-thickness skin flaps were created medially and laterally. The ulnar nerve was identified, transiently transposed, and repositioned to its anatomic location at the end of the case.
For ORIF with an olecranon osteotomy, the olecranon was pre-drilled and tapped to accept a 6.5 mm screw to repair the olecranon at the end of the case. A standard chevron, osteotomy was then performed. The articular surface was addressed by either reconstructing the entire articular distal humerus first and then attaching it to the metaphysis, or by building and restoring 1 column (medial or lateral) to the distal humerus metaphysis followed by restoration of the second column. Detailed articular reconstruction was achieved and maintained with 1.25 mm, 1.6 mm Kirschner wires, and 1.5/2.0/2.7/3.5 mm screws as needed. Pre-contoured distal humerus locking plates were then applied in parallel or orthogonal orientation, for final fixation of the distal articular segment to the shaft. 13 In a small number of cases, only a single columnar plate was used (See Table 3). A combination of cortical and locking screws were used proximally to the fracture and the olecranon was anatomically reduced and fixed with a 6.5 mm intra-osseous screw reinforced with a tension band reinforcement. We do not use plates at our institution to repair simple fractures or surgical osteotomies of the olecranon due to cost, unnecessary biomechanical need, and frequent need for hardware removal.
Plating Configurations and Operative Time.

None = columnar screws and wires only
In the limited fixation technique, medial and lateral paratricipital dissection allowed for some visualization and limited reduction of the articular surface while preserving the triceps insertion. Single column or bicolumnar (medial and lateral, orthogonal or parallel) locking plates were then applied to secure the articular segment to the humerus and address varus and valgus instability. In 3 cases, sufficient fixation was achieved with columnar screws and wires alone. Anatomic reduction of the intra-articular comminution beyond that allowed by this limited exposure was not attempted.
In both groups, a posterior splint was maintained for 7-14 days allowing free motion of the wrist and digits. Formal elbow physical or occupational therapy was implemented after the first post-operative visit at 2 weeks. At this time, the splint was discontinued and all patients were encouraged to start passive, active assisted, and gentle active ROM as tolerated but without resistance. By week 4, therapists were instructed to advance motion with gentle stretching and patients were encouraged to use the arm for daily activities without lifting heavy objects or pushing. By week 8, ROM stretching was unrestricted and patients started gentle resisted active exercises. By week 12 all restrictions were lifted.
The senior author performed the majority of procedures with the remainder of procedures performed by 2 other trauma fellowship trained orthopedic surgeons at the same institution. Patients were not randomized and the choice of the procedure was at the discretion of the treating surgeon. Generally, indications for the limited fixation technique can be summarized as: a) need for ORIF as may occur secondary to an open fracture, grossly unstable injury, injury compromising skin integrity if left without stability, vascular injury, other acute need for open intervention; b) presence of trochlear comminution and an intact olecranon in osteoporotic bone in addition to a); and c) an injury in a geriatric patient with significant medical comorbidities in addition to a) and b) as above.
The primary outcomes of this study were final elbow range of motion (in the coronal plane), complications, and the need for additional elbow surgery. Secondary outcomes included patient-reported pain and function, via outcome measurement tools, which were obtained in clinic or administered remotely. The Patient-Reported Outcomes Measurement Information System (PROMIS) were used for pain interference (PI) (version 1.0) and physical function (PF) (version 1.0). PROMIS instruments, which when scored, result in T scores standardized to a normative US population, have been validated in prior studies to reliably measure their intended outcomes in orthopaedic patients. 8,14 -16 The mean score for each T score distribution is 50 and the average standard deviation is 10 points. Inherent to the PROMIS measures, a higher PF score signified increased function and a higher PI score indicated increased pain.
All patients had at least 12 months of follow up and documented final elbow range of motion, complications, and any additional surgeries except for 1 patient who had follow-up care in another state where she lived. Medical record review revealed 20 patients were deceased at the time of phone survey and 12 patients were prohibitively demented. Seventeen patients of a possible 24 completed the patient-reported outcome measurement tools, leading to a response rate of 70.8%. None of the deaths during the follow-up period were due to the distal humerus fracture or operation.
Means were calculated for all continuous variables, and groups were compared using 2-sided independent samples t-tests (with α < 0.05). Calculations were performed in REDCap (Vanderbilt University, Nashville, TN) or in Microsoft Excel (Microsoft Corporation, Redmond, WA).
Results
The average patient age for the ORIF with osteotomy group was 76.9 and for the limited fixation groups was 79.8 years. The mean follow-up duration for the study was 15.2 months (range 12-97 months). The average final elbow range of motion in the coronal plane was 97° (40°-155°) in the ORIF with osteotomy group and 86.5° (20°- 145°) (p = 0.231) in the limited fixation group (Table 4). The average final elbow extension (degrees short of full extension—0°) was 22.5° (0°-45°) in the ORIF w/ osteotomy group and 26.9° (0°- 90°) in the limited fixation group (p = 0.539) (Table 4).
Outcomes for Treatment Groups.

In the ORIF w/osteotomy group, there were 11 types of complications in the follow-up period in 11 patients (36.7%), and 10 patients underwent additional surgery (33.3%). In the limited fixation group, there were 2 types of complications in 4 patients (15.4%), and 4 underwent additional surgery (15.4%) (Table 5). There was a trend to more complications (p = 0.073) and additional surgery (p = 0.122) in the ORIF w/ osteotomy group compared to the limited fixation group but this did not reach statistical significance.
Complications and Additional Surgeries.

PROMIS scores for pain were for 53.1 and 52.14 in the ORIF w/osteotomy and limited fixation groups, respectively (p = 0.867) and PROMIS function scores were 41.7 and 41.4, respectively (p = 0.957). The average operative time was 168 minutes in the ORIF w/ osteotomy group and 135 minutes in the limited fixation group, a difference of 33 minutes which was statistically significant (p = 0.041).
Discussion
In this retrospective study, patients over age 65 with intra-articular distal humerus fractures treated with a limited fixation technique had comparable outcomes, with regard to pain, function, and final range of motion, to patients who underwent ORIF of the distal humerus with an olecranon osteotomy and with anatomic joint reconstruction. We propose that in select geriatric patients, a limited fixation approach as described (Figure 1 –3), minimizes complications and surgical time while achieving similar clinical results. While we refer to our approach as a limited fixation technique to differentiate it from an approach with an olecranon osteotomy, we believe it remains stable and appropriate fixation to provide valgus and varus stability while avoiding unnecessary disruption of trochlear comminution that may be non-reconstructable.

An 83 year-old female sustained a comminuted intra-articular distal humerus fracture after a fall from standing with an associated radial head fracture. Initial lateral (A) and oblique (B) radiographs, and representative sagittal (C) and coronal (D) computed tomography images, demonstrate significant intra-articular comminution of the fracture. Post-operative radiographs 3 months after surgery, utilizing a limited fixation technique, demonstrate the preserved overall geometry of the distal humerus and ulnohumeral joint space on lateral (E) and anterior-posterior (F) radiographs. After fracture healing, her medial plate was removed due to discomfort, and at the time of final follow up at 14 months, she was pain free with a total-arc elbow range of motion (combined flexion-extension) of 105°. Final radiographs demonstrate preserved alignment, fracture union, and maintained ulnohumeral joint space on lateral (G) and anterior-posterior (H) radiographs.

A 74 year-old female sustained a comminuted intra-articular distal humerus fracture after a fall from standing with an associated ipsilateral distal radius fracture. Initial lateral (A) and anteriorposterior (B) radiographs, demonstrate significant intra-articular comminution of the fracture and unstable valgus deformity. Post-operative radiographs at the time of surgery, utilizing a limited fixation technique, demonstrate joint congruency with fixation through the plates without the need of an olecranon osteotomy, lateral (C) and anterior-posterior (D) radiographs. At 9 months from surgery, she was pain free with a total-arc elbow range of motion (combined flexion-extension) of 90°. Final radiographs demonstrate preserved alignment, fracture union, and maintained ulnohumeral joint space on lateral (E) and anterior-posterior (F) radiographs.

A 76 year-old male hairdresser sustained a comminuted intra-articular distal humerus fracture after a fall from standing in the context of an associated prior ulnar pseudoarthrosis and dysplastic elbow changes with pre-existing limitations in pronation. He underwent fixation to preserve existing function of his elbow. Initial anterior-posterior (A) and oblique (B) films and sagittal (C) and coronal (D) CT views demonstrate significant intra-articular comminution. Post-operative radiographs at healing (E and F) demonstrate fixation with lateral plates with return to baseline function allowing the patient to return to work.
Geriatric intra-articular distal humerus fractures are often complex and challenging to treat, and the results can be poor. They comprise approximately 2% of fractures, often occurring in independent and active older females with an incidence that is expected to rise significantly as the population above 80 years of age increases. 6,17 -19 The goals of treatment for elderly patients are comfort, preservation of a functional range of motion (flexion arc 30°- 130°) for activities of daily living, and minimizing complications. Surgical fixation of a comminuted distal humerus fracture poses technical challenges especially in elderly patients with comminuted fractures, osteoporotic bone, poor wound-healing secondary to co-morbidities, and limited physiologic reserve. 6
Non-operative management, consisting of brief elbow immobilization followed by early range of motion is an option in patients deemed too medically unwell to tolerate an operation. This “bag of bones” approach was first described in the literature by Eastwood in 1937, who reported on 14 patients with adequate elbow function, 12 of whom returned to work (or previous functional level), after non-operative treatment of a distal humerus fracture, although a closed reduction under general anesthesia was commonly performed. 1 Recent studies have demonstrated mixed results with non-operative care which can result in pain, poor functional outcomes, instability, non-union, and distorted distal humerus geometry. 2,3,10,20,21
There is a paucity of data comparing the results of non-operative treatment to operative treatment for intra-articular distal humerus fractures. In a retrospective review in 1986, Zagorski et al. compared the outcomes of comminuted intra-articular fractures of the distal humerus in 29 patients who were treated operatively with ORIF and 13 patients treated non-operatively. 21 In this study 23 patients were treated with screw fixation only, 5 patients with plates and screws, 1 patient by multiple pin fixation, with 76% reported to have had an excellent or good result whereas only 8% of patients treated non-operatively achieved a similar outcome. Notably, this patient group was substantially younger, with a mean age of 45 years (range 17 to 82 years), compared to our present study. Higher non-union and delayed union rates with non-operative treatment were seen in an observational cohort by Robinson et al. in a study of 320 adult patients with distal humerus fractures. 18 In a non-randomized study of 28 elderly patients (mean age of 85 years) with distal humerus fractures by Srinivasan et al. in 2005, OTA grading demonstrated favorable results (3 excellent, 9 good, 7 fair, and 2 poor) in patients treated with ORIF compared with the non-operatively treated group (zero excellent, 2 good, 3 fair, and 3 poor). 22 The operatively treated group had more substantial pain relief (mild or no pain) compared to the non-operative group (52% v. 25%) along with a better mean arc of motion (75.5° v. 37.5°). Similarly, John et al. reported favorable outcomes in 49 elderly patients (mean age of 80 years) with distal humerus fractures who were treated operatively. 23 Eighty percent of patients assessed their result as either very good or good and the authors noted the incidence of implant failure, pseudarthrosis of the olecranon osteotomy, and ulnar nerve lesions were similar to younger adult populations at the time of study. We believe our limited fixation technique captures some of the benefits of a non-operative approach, by minimizing surgery and potential post-operative issues related to olecranon fixation in elderly or medically unwell patients, while achieving similar functional and pain relief outcomes as ORIF with intra-articular reconstruction.
Intra-articular distal humerus AO/OTA type C fractures are challenging fractures to treat operatively given the distal fracture lines of one or both columns, the osteoporotic bone in elderly patients, the extent of comminution of the articular surface, along with metaphyseal fragmentation of one or both columns. Options to access the ulnohumeral joint through a posterior approach to the distal humerus include, but are not limited to, triceps splitting, triceps reflecting, triceps preserving (paratricipital), and an olecranon osteotomy. 7 Through a cadaver study, Wilkinson et al. studied the percentage of the distal humerus exposed through the common posterior surgical approaches, 24 reporting 35%, 46%, and 57%, for the triceps splitting, triceps reflecting, and olecranon osteotomy approaches respectively. While the triceps reflecting approach and the olecranon osteotomy allowed the most visualization of the distal humerus, both disrupt the extensor mechanism of the elbow. With the triceps reflecting approach, the elbow is commonly immobilized for a longer period of time post-operatively to allow the triceps tendon to heal, which may lead to loss of range of motion and worse functional outcomes. With an olecranon osteotomy, an intra-articular osteotomy is made which disrupts the articular cartilage of the ulnohumeral joint and makes conversion to a total elbow arthroplasty more challenging if it is ever needed. Additionally, some surgeons may delay active extension to allow healing of the osteotomy which is fixed with hardware that is often prominent and commonly removed. 11 In contrast the triceps splitting approach leaves the extensor mechanism intact and allows for early postoperative rehabilitation, at the expense of a more limited visualization of the distal humerus articular surface. In a retrospective review of 25 patients, McKee et al. reviewed the functional results of fractures treated with ORIF through a posterior approach using the triceps splitting technique versus an olecranon osteotomy. They found no significant difference in the patients’ strength or total arc of motion, which was 108° and approximately 75% of their uninjured side, utilizing these 2 approaches. 25 As first described by Alonso-Llame, the paratricipital (or triceps sparring) approach does not split the triceps muscle nor disrupt the extensor mechanism, but rather exposes the distal humerus by working around the medial and lateral distal triceps and the respective intermuscular septa, thus allowing early postoperative rehabilitation. While visualization for anatomic fixation of AO/OTA Type C distal humerus fractures can be challenging, elbow extension to relax the triceps muscle and tendon can help with paratricipital exposure. In a retrospective review of 67 elderly patients with AO/OTA Type C distal humerus fractures, Zhang et al. compared the results of patients who underwent ORIF using the olecranon osteotomy approach (n = 36) and the triceps-sparing approach (n = 31). 26 For patients with type C1 and C2 fractures, they observed reductions in operative time, blood loss, complication rates, and significantly better Mayo Elbow Performance Score (MEPS) using the triceps-sparing approach compared to an osteotomy approach at final follow-up. In type C3 fractures, both approaches achieved similar elbow functional outcomes while operative time, blood loss, and complication rate was lower in the triceps-sparing approach. Similarly, our study found a shorter operative time of 135 minutes in our limited fixation group, 33 minutes shorter than the ORIF with an olecranon osteotomy group (p = 0.041).
Both the olecranon osteotomy approach and paratricipital approach allow dual plating of distal humerus. Dual plating is the established standard of care for most type C intra-articular distal humerus fractures and has been shown to be significantly stronger than other choices. 27 While biomechanical studies 4,28,29 have shown that parallel locked plate fixation demonstrates greater mechanical stiffness and stability compared with orthogonal locked and non-locked plating, clinically the plate orientation does not appear to affect outcomes or complication rates. Lee et al. prospectively randomized 67 patients with distal humerus fractures to fixation with orthogonal or parallel plating and found no significant differences in clinical outcomes, radiographic reductions, mean operation time, union time, or complication rates between the groups. 30
Limitations to the present study include its retrospective design and small sample sizes. The lack of difference between groups might have resulted from the small sample size of our cohort due to Type II error. However, the intent of the present study is to introduce a technical treatment option for a unique subgroup of patients and motivate a more rigorous future study delineating outcomes in a larger cohort. Additionally, due to the patient population, 32 patients (20 deceased, 12 prohibitively demented) were unavailable to participate in PROMIS scores, the study’s secondary outcomes. Patients were selected for treatment based on the attending surgeon’s discretion, thus inherently adding selection bias to the groups. Evidenced by a slightly higher ASA score (2.7 in limited fixation group versus 2.4 in ORIF w/olecranon osteotomy group), we believe the limited fixation group may have actually been more medically compromised, and hence selected for more limited treatment. Despite their medical condition, the limited fixation group achieved similar outcome scores. In this study we were unable to explore the effect of some covariates like patients’ demographics, BMI, and ASA, on the outcome. Further research with a prospective design and a larger sample size would be of interest to explore the effect of fracture pattern, bone density as measured quantitatively, heath status indicators (i.e., ASA, Charlson Comorbidity Index (CCI), Elixhauser Comorbidity Index), and functional level (as assessed by PROMIS, Disabilities of the Arm, Shoulder and Hand Score (DASH), Upper Extremity Functional Index (UEFI)), on the outcome of treatment with the proposed limited fixation technique.
In conclusion, we believe a technique of limited columnar fixation as described in this manuscript for intra-articular fractures in an elderly population is a valid treatment option with similar elbow motion, function, and pain relief at final follow-up when compared to ORIF with an osteotomy and an effort to anatomically reconstruct intra-articular comminution. By minimizing some of the more challenging technical issues associated with an olecranon osteotomy and open reduction of a highly comminuted trochlea with osteoporotic bone, this treatment option may allow for patients to be treated without referral to a tertiary level center. This could facilitate care within the patient’s community and provides access to family for these older patients. The limited fixation approach proposed offers valgus and varus stability which suffices to provide the patient with a stable elbow and thus allow the intra-articular comminution to heal by secondary congruency against an intact olecranon. This approach may be used selectively in geriatric patients who would benefit from surgical management, but may be lower functioning, medically unwell, or have such poor bone quality that anatomic reduction with an olecranon osteotomy would be difficult at best. Our approach also preserves olecranon integrity allowing for total elbow arthroplasty as a potential future option. While our conclusions from this limited series are suggestive of a potential benefit in terms of equivalency of outcome for this particular population when compared to results from more extensive surgery, our observations are to be interpreted in this context.
Footnotes
Authors’ Note
This manuscript is not based on a previous communication to a society or meeting. No benefits in any form have been received or will be received from commercial party related directly or indirectly to the subject of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.