
Abstract
Keywords
Introduction
Osteoporotic vertebral compression fractures (OVCF) frequently occur in elderly patients following a minimal trauma or spontaneously, particularly in postmenopausal women.1,2 It is commonly characterized by varying degrees of local pain associated with the fracture site, primarily axial back pain.3,4 Conservative observation can be considered when no neurological complications or OVCF are stable. However, in the lower lumbar legion, patients occasionally complained of both axial and radiating pain following an OVCF. In some cases, delayed onset of radiculopathy is observed after conservative therapy for OVCF due to advanced vertebral collapse. 5
Generally, percutaneous vertebroplasty or kyphoplasty is recommended as a minimally invasive procedure for rapid pain relief through mechanical stabilization. 6 Intervertebral fusion is a reasonable method to treat vertebral fractures, but this type of surgery is invasive for elderly patients and complications are not uncommon. Because OVCF occurs based on osteoporosis, even in the case of vertebral screw fixation, subsequent adjacent segment vertebral fractures often occur.
The transforaminal full-endoscopic lumbar foraminoplasty and/or discectomy (FELFD) for lumbar disc herniation and lumbar stenosis obtained good clinical results produced from diverse review and meta-analysis articles.7,8 In the present study, the surgical strategy for patients with radiculopathy caused by foraminal stenosis following a compression fracture of the lower lumbar spine is described. Our surgical route of transforaminal FELFD is proposed as an effective treatment option for frail patients with lumbar compression fracture, including those with severe osteoporosis and elderly.
Materials and Methods
Patient Population
This retrospective study has been approved by the Institutional Review Board (IRB) of the authors’ affiliated institution. Informed consents were approved by the IRB and obtained from all patients. A total of 15 consecutive patients underwent transforaminal FELFD due to radiculopathy after OVCF in the lumbar spine between May 2015 and November 2019. Surgical indications for the selected 15 patients were single-level injury and presence of unilateral radiating leg pain with/without a history of vertebroplasty or kyphoplasty. Patients who complained about back pain and local kyphotic changes underwent vertebroplasty or kyphoplasty. Patients with kyphotic change with instability underwent posterior lumbar fusion. All patients reached a minimum of 12-month follow-up. All surgeries were performed by one senior spine surgeon and under local anesthesia.
Patient data, including sex, age, index level, symptom duration, bone mineral density (BMD; T-score), Charlson comorbidity index (CCI), American Society of Anesthesiologists (ASA) score, operative time, and complications were obtained. Clinical outcomes, rated using the Visual Analog Scale (VAS) and the Oswestry Disability Index (ODI), were recorded preoperatively and at 12 months postoperatively. MacNab criteria were used to evaluate patients' satisfaction. The cross-sectional area of foraminal (CSAF) was measured in computed tomography (CT) sagittal cut using an imaginary line around the neural foramen on symptom sides at preoperative, immediately after surgery, and 1-year after surgery.
Surgical Technique
The surgical technique was similar to those reported in the literature for vertebroplasty or kyphoplasty 9 and posterior lumbar fusion. 10 The transforaminal FELFD surgical technique was similar to that of our previous report. 11
The procedure was performed under local anesthesia in prone position on the radiolucent table in all 15 patients. All the procedures were performed by a single senior surgeon. The skin entry point was generally 10–14 cm from the midline. An 18-gauge spinal needle was inserted along the planned trajectory line under fluoroscopic guidance. Thereafter, the guide wire, obturator, and the final working sheath were inserted in accordance with the staged dilation procedure. The bevel working channel was docked firmly between the inferior pedicle and superior articular process. An endoscope (SPINENDOS GmbH, Munich, Germany) was introduced through the working channel. The surrounding fatty tissue and blood vessels were sealed by a radiofrequency coagulator (VANTAGE BIOTECH CO., LTD., Taoyuan, Taiwan). Expanding the foramen and sacrificing only a small part of the superior articular process using the cutting and diamond burrs (VANTAGE BIOTECH CO., LTD., Taoyuan, Taiwan), we removed the bony fragment from the posterior wall below the pedicle, and additional discectomy was performed if necessary. Then the nerve root was identified and decompressed. The working channel and endoscope were removed, and the wound was closed without drainage.
Case Presentation
Case (A), preoperative magnetic resonance imaging (MRI) sagittal view shows fracture in lower L4 vertebral body; (B) preoperative computed tomography (CT) shows the bone fragment compressed intervertebral foramen space; (C), preoperative MRI shows the fragment covered in a fibrous film of the posterior wall of fractured vertebral body compressing L4 root from the front at the foramen (red ring); (D), preoperative MRI axial view shows severe foraminal stenosis at the L4-L5 right side (yellow ring); (E andF), introduced endoscopy and performed foraminoplasty using the drill; (G), well decompressed nerve root; (H), resected the superior articular process and removed bone fragment (blue ring). Anterioposterior and lateral X-ray films after kyphoplasty.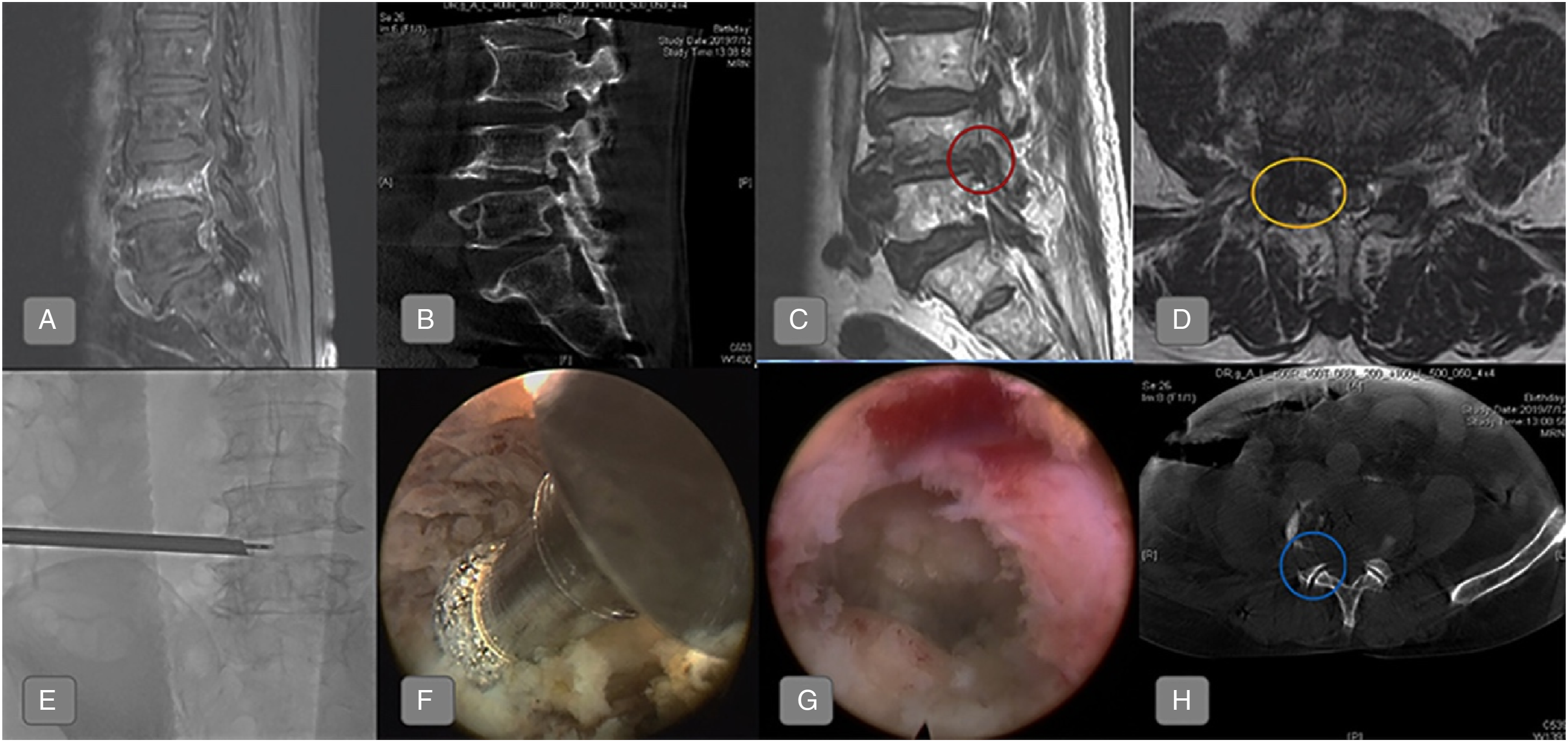

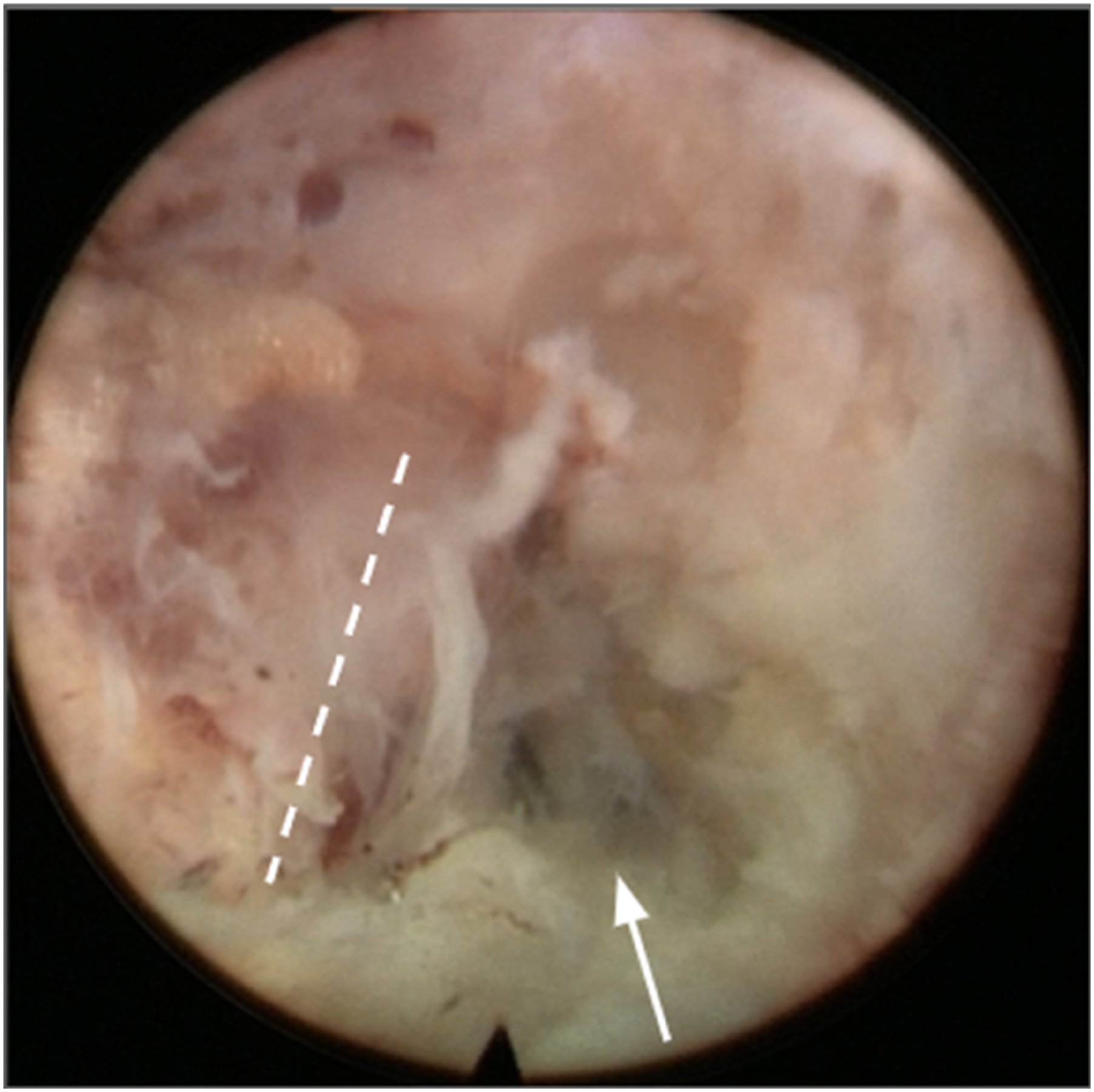
Case (A), preoperative lumbar spine X-ray shows wedge shape deformity of L4 vertebral body with bone cement injection (white arrow); (B), preoperative magnetic resonance imaging (MRI) revealed protruded L4-L5 disc herniation with upward migration (white arrowhead); (C and D), MRI axial view shows severe foraminal stenosis at the left L4-L5 level (asterisk). After resecting the superior articular process, partial inferior articular process and removing bone fragment, compressed exiting nerve root of L4 and upward herniated disc were exposed. The nerve root was decompressed by removing the disc fragment with the forceps or a hook. Decompressed nerve root was indicated by white dash-lines and resected herniated disc was pointed out by white arrow.
Statistical Analysis
Quantitative variables were calculated as means ± standard deviations, and qualitative variables as numbers. Two-sample t-tests were performed for continuous variables. A P-value of <.05 represented a statistically significant difference.
Results
Summary of detailed information of all 15 cases of radiculopathy after osteoporotic vertebral compression fractures.

ASA: American Society of Anesthesiologists; CCI: Charlson comorbidity index, PKP/VP: Percutaneous kyphoplasty/vertebroplasty.
Clinical and Radiological Data of all 15 Cases.
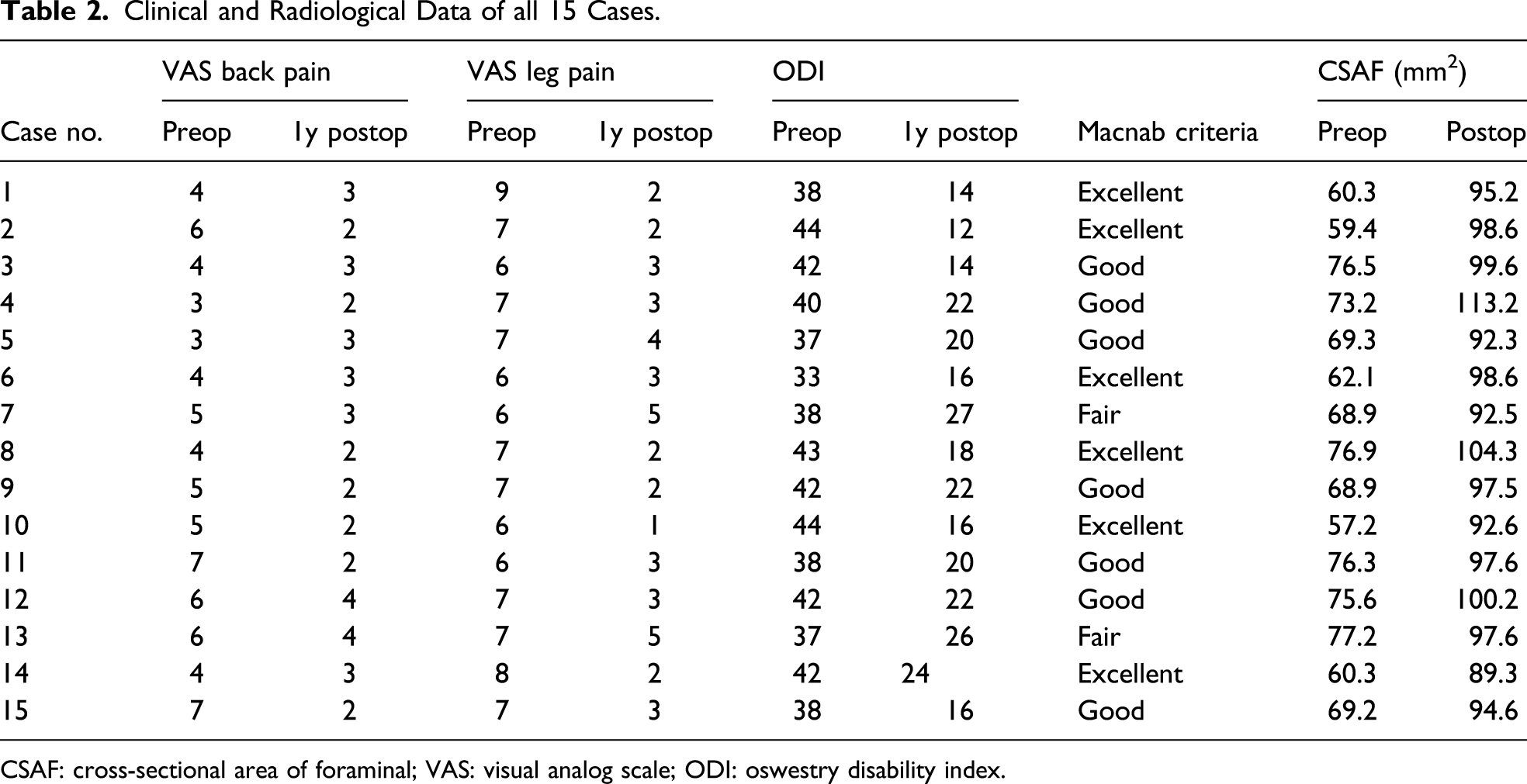
CSAF: cross-sectional area of foraminal; VAS: visual analog scale; ODI: oswestry disability index.
Preoperative CSAF (mm2) increased from preoperative 68.7 ± 7.2 to 97.6 ± 5.8 during the last follow-up (P < .05; Table 2).
Except for one case(#1), there were no patients who had perioperative complications or required subsequent kyphoplasty or vertebroplasty during the follow-up period.
Discussion
With older people living more active lives, problems with fracture are rapidly increasing. With their increasing physical demands but poor medical disposition, optimizing treatment options becomes critical. 12 OVCF does not always manifest as benign lesions. It causes severe and refractory back pain or neurological complications that require surgical intervention. Although the exact prevalence of OVCF and neurological symptoms remains unknown, a retrospective research on 738 patients with OVCF showed that 5.5% of patients had neurological symptoms. 13 Spinal fixation surgery for the treatment of osteoporotic spinal fractures can cause various complications, such as blood loss, infection, longer hospitalization, and pseudarthrosis, which may be magnified in elderly patients. 14 Meanwhile, reported that vertebral BMD above the fusion segment was significantly reduced. 15 Obviously, spinal fusion strategies potentially influence the incidence of further new compression fractures for patients with severe osteoporosis. 16 In addition, poor bone fragility remains due to aging and various comorbidities, making it difficult to keep the instrument fixed to maintain the alignment of the fused spine. Moreover, transforaminal epidural steroid injection is often used in patients with radicular symptoms from spinal stenosis, and the efficacy of transforaminal epidural steroid injection has been demonstrated in previous reports.17,18 However, most patients have short-term pain relief, and lack long-term effects, which may require repeated injections of steroids. Furthermore, the efficacy of transforaminal epidural steroid injection in patients with altered anatomical stenosis and severe stenosis has not been clearly documented. Therefore, significant clinical challenges should be clearly recognized during the surgical treatment evaluation.
Foraminal stenosis is usually caused by degenerative changes in the lumbar spine; in this situation, OVCF can further induce foraminal stenosis. 19 Preexisting foraminal stenosis has progressed to radiculopathy due to lumbar spine compression fracture. 20 The proposed mechanism is that the height lost in the intervertebral foramen due to the descent of the pedicle and collapsed lower lumbar vertebral body damaged the posterior wall of the lower vertebral bone fragment directly compressed on the foraminal legion and subsequent instability. One study 21 reported an 85-year-old woman with an L3 vertebral fracture who presented with back pain, bilateral radiculopathy, and weakness after 4 months of conservative treatment. The patient underwent L3-L4 foraminal decompression and fused unstable segment because of unstable index level, and the L3 vertebral body collapse leads to compressed L3 nerve root. Back pain and neurologic symptoms significantly improved postoperatively. Moreover, collapse occurred in the lower part of the vertebral body inferior to the pedicle level; therefore, spine surgeon should be aware of the foraminal stenosis feasibility. Another paper 22 described a case of an 80-year-old female patient presented severe unilateral radiculopathy following an OVCF. Computed tomography revealed that a fragment of the posterior wall of the vertebral body under the pedicle compressed the L2 nerve root. Because the patient almost had no back pain and was relatively fragile, a microendoscopic foraminal decompression was performed. Postoperatively, the pain was immediately relieved and significant clinical improvement was achieved.
So far, there have been few reports of FELFD treatment of radiculopathy after OVCF. One study 23 presented three cases of radiculopathy after OVCFs treated by transforaminal full-endoscopic lumbar discectomy and foraminoplasty. The average operative time was 60.7 (range, 57–72) mins. The mean numerical rating scale scores decreased from preoperative 9 to postoperative 2.3, and there were no postoperative complications. The expansion of the collapsed vertebral foramen is the core principle of transforaminal FELFD treatment, in which the combination of foraminoplasty, discectomy, and osteophyte removal is a key in this technique. In the present study, almost patients were elderly with severe osteoporosis and were effectively treated with transforaminal FELFD to relieve pain without the need for general anesthesia. All patients with transforaminal FELFD for radiculopathy following OVCF, six reported excellent outcomes and seven with good outcomes according to the MacNab criteria. Therefore, despite the patient’s advanced age combined with comorbidities and severe osteoporosis, our surgical strategy is considered appropriate due to less trauma and the use of local anesthesia, seems to be a potential alternative treatment for radiculopathy after OVCF.
In addition, majority of patients undergoing OVCF are elderly, and prolonged surgical stress may pose risks. The advantages of choosing local anesthesia for certain operations in the elderly are: reducing postoperative central nervous system dysfunction, reducing anesthesia complications, reducing stress response, reducing postoperative thrombosis, and maintaining stable circulation.
In this study, we propose safe algorithms to address conditions present in clinical practice, from acute insufficiency fractures to chronic unstable fractures with impending neurology. We also suggested that transforaminal FELFD indicates good outcomes in patients with unilateral radiating pain without or slightly back pain. If subsequent back pain arisen or aggravated, a vertebroplasty or kyphoplasty procedure was performed. If the patient develops bilateral radiculopathy, percutaneous endoscopic or open surgery can be selected according to the patient’s and surgeon’s preference. However, in patients with central stenosis or cord compression, open surgery was recommended. The flow chart is shown in Figure 5. Surgical management algorithm for radiculopathy due to osteoporotic vertebral compression fractures in the lower lumbar spine. FELFD: full-endoscopic foraminoplasty and/or discectomy.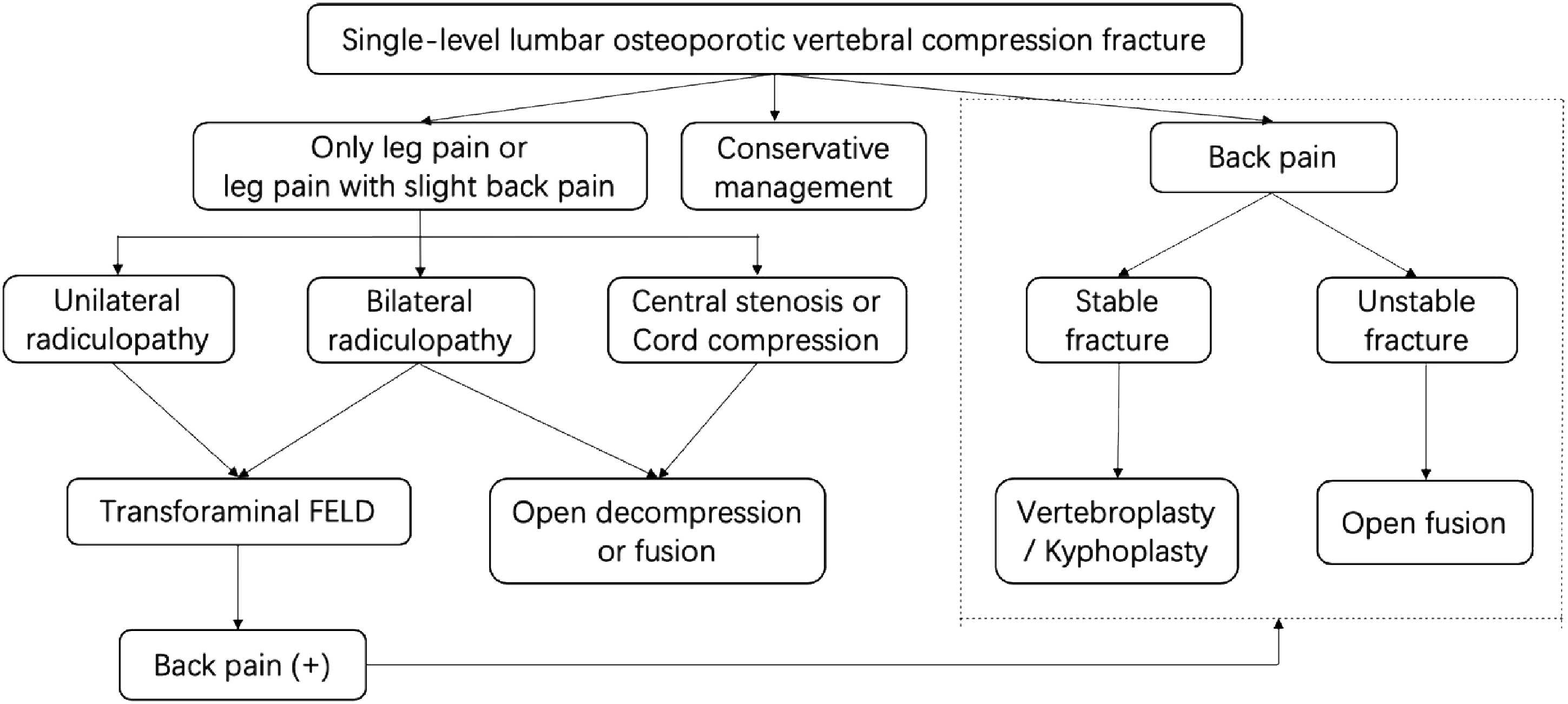
The theory of symptom occurrence proposed in this study is speculative. To solve this problem more scientifically, experimental data include accurate measurement of the foramen size based on the weight load in the fractured vertebra. Experimental research with finite element models may be a good way to test hypotheses. In addition, due to the limited number of cases, lack of a control group and short follow-up period, further prospective studies on transforaminal FELFD for the treatment of foraminal stenosis due to OVCF will be required, including larger sample sizes, multicenter, add control group, and longer follow-up periods.
At present, we think that transforaminal FELFD can help patients in the special situations described above. Therefore, after accurately diagnosing the cause of radiculopathy, surgical management should be selected after considering the general condition. However, mechanisms proposed to explain improved symptoms require further verification, and some important points can be highlighted when performing transforaminal FELFD based on the results in these patients.
Conclusion
The transforaminal FELFD is an effective treatment option for foraminal stenosis due to lumbar OVCF, including those patients are elderly with severe osteoporosis.
Footnotes
Author Contributions
Writing–original draft, Guang-Xun Lin; Investigation, Li-Wei Sun; Software, Shang-Wun Jhang; Validation, Su-Wei Ou; Formal analysis, Kai-Sheng Chang; Methodology, Ru-Yin Tsai; Project administration, Bao-Shan Hu; Supervision, Gang Rui; Writing–review and editing, Chien-Min Chen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This retrospective study was approved by the institutional Ethics Committee of the Changhua Christian Hospital. Informed consent was waivered due to the retrospective and non-interventional nature of this analysis.
Consent for Publication
Written informed consents for publication were obtained from all participants.
Availability of Data and Materials
The datasets are available on request due to privacy or other restrictions.