
Abstract
Background:
Due to the need for medical optimization and congested operating room schedules, surgical repair is often performed at night. Studies have shown that work done at night increases complications. The primary aim of our study is to compare the rates of complications and 30-day mortality between 2 surgical times of day, daytime group (DTG, 07:00-15:59) and nighttime group (NTG, 16:00-06:59).
Methods:
Retrospective chart review from 2005 through 2010.
Setting:
Level 1 Trauma Center.
Participants:
1443 patients with hip fracture, age ≥50 years with isolated injury and surgical treatment of the fracture.
Main Outcomes and Measures:
Thirty-day mortality and complications: myocardial infarction, cardiac event, stroke, central nervous system event, pneumonia, urinary tract infection, postoperative wound infection, and bleeding requiring transfusion of 3 or more red blood cell units.
Results:
A total of 859 patients met the inclusion criteria; 668 patients in the DTG and 191 patients in the NTG. The 30-day mortality was 7.8%. The complication rate was 28%. No difference was found in 30-day mortality or complication rate based on the time of day the surgery was performed (P = 1.0 and P = .92, respectively). This remained unchanged when controlling for health status and surgical complexity. Age (odds ratio = 1.03/year), Charlson Comorbidity Index (CCI; odds ratio = 1.21), and American Society of Anesthesiologists (ASA; odds ratio = 1.85) score were predictive of adverse outcomes.
Conclusion:
Surgical time of day did not affect 30-day mortality or total number of complications. Age, ASA score, and CCI were associated with adverse outcomes.
Introduction
Each year in the United States, fractures in the elderly people account for approximately 432 000 hospital admissions, 2.5 million office visits, and 180 000 nursing home admissions. 1,2 Total annual costs exceed US$17 billion. 3,4 The incidence of fractures in individuals more than 50 years old approaches 50% in women and 20% in men. As a subset of these fractures, hip fractures are a major contributor to resource expenditures, accounting for 14% of the total number but 72% of the costs of fractures in the elderly individuals. 1 -4 In addition, the number of hip fractures is projected to double or triple by the year 2040. 5
High complication and mortality rates associated with hip fractures have been well documented in the literature. 6 -15 Poor outcomes may be predicted by patient comorbidities, surgical timing, and surgical volume. 7,15 -27 The effect of surgical time of day on hip fracture outcome is less clear.
Prior to surgery, many patients with hip fracture require medical optimization that may delay their surgical start time. 28 In addition, delays due to surgeon and operating room (OR) availability may result in the treatment of many of these fractures at night. 28 -30 Several studies in the general medical literature have shown that after-hours surgery has led to a higher rate of complications. 31 -35
In the orthopedic literature, however, there is a paucity of data regarding the effect on outcome of surgical time of day. Even less information exists regarding time of day of surgical repair of hip fractures and outcomes. 36,37 Fatigue, reduced staff availability, and decreased familiarity with the surgery are theories proposed for increased operative risk at night. 38,39
The purpose of this study was to retrospectively compare the rates of complications and mortality between 2 surgical times of day, daytime group (DTG, 07:00-15:59) and nighttime group (NTG, 16:00-06:59). We hypothesized that there would be a significant increase in 30-day mortality and complications in patients with hip fractures treated surgically at night rather than during daytime hours.
Materials and Methods
Following institutional review board approval, a retrospective chart review was performed for patients surgically treated for a hip fracture from January 1, 2005, to December 31, 2010, at a Level I trauma center. Patients aged 50 years or older with an isolated hip fracture (intertrochanteric, subtrochanteric, or femoral neck fracture) who underwent surgical intervention were included in the study. Patients with periprosthetic fractures, osteotomies (Girdlestone procedures), multiple injuries, or incomplete records were excluded.
Medical records were reviewed for age, comorbidities, American Society of Anesthesiologists (ASA) score, time to surgery, procedure length, total time in the OR, intraoperative fracture, and complications (myocardial infarction [MI], cardiac event, stroke, central nervous system event, pneumonia, urinary tract infection [UTI], postoperative wound infection, bleeding requiring transfusion of 3 or more red blood cell units and 30-day mortality). Individual comorbidities were used to calculate the Charlson comorbidity index (CCI) for each patient. The CCI score was originally validated as a prognostic tool designed to predict mortality in medical patients 1 year after admission by categorizing and assigning weights and severities to 19 different patients with comorbidities. 40 The original study validation was done in 1987 on general medical patients. Patients with a score of 0 had a 1-year mortality of 12%; those with scores of 1 to 2 had a 1-year mortality of 26%; those with scores of 3 to 4 had a 1-year mortality of 52%; and those with scores ≥5 had a 1-year mortality of 85%. 40 The CCI has since been used to assess the association postoperative 30-day mortality in older patients undergoing hip fracture surgery. 41 Surgical start time, defined as the time of surgical incision, was recorded and used to assign the patients into a DTG (07:00-15:59) and an NTG (16:00-06:59). Our primary outcome was postoperative complications as defined previously. Our secondary outcome was 30-day mortality.
First, variables in our sample were described with summary statistics (eg, means, medians, standard deviations, and frequency counts) as appropriate for the type of data. We used Mann-Whitney-Wilcoxon tests to investigate the association between day and night surgery time and continuous or ordinal covariates. Bivariate associations between DTG/NTG surgery time and other variables (including the primary outcome variables of complications, adverse events, and 30-day mortality) were estimated using Fisher exact tests. Logistic regression was used to estimate the associations between measured covariates and complications. These associations were expressed in terms of odds ratios and 95% confidence intervals (CIs). Predictors that were associated with complications at P < .1 were selected for evaluation using multiple logistic regression, with the exception of total time of surgery, which was removed due to its colinearity with time in the OR. Receiver–operating characteristic curve analysis was used to compare 4 possible sets of prognostic indicators for complications: (1) all available predictor variables, (2) all available predictors except for DTG/NTG surgery time, (3) variables that were shown to be independent predictors (P < .05) in multiple logistic regression, and (4) DTG/NTG surgery time only (Figure 1). With the exception of the aforementioned multiple regression model selection processes, statistical tests were all 2 sided, with α = .05. The majority of analysis was done using SAS v9.2 (Cary, North Carolina). Figures were produced using the statistical software R 2.9.2 (Vienna, Austria).

Receiver–operating characteristic (ROC) curve analysis was used to compare 4 possible sets of prognostic indicators (listed in the legend) for complications. Of the 4 models analyzed, the greatest predictors of adverse outcomes (mortality and complications) were age, ASA score, and Charlson comorbidity index. Surgical time of day was not predictive of adverse outcomes.
A power analysis for testing the association between complication rate and surgical time of day was conducted. Our assumptions were that 24.7% of the patients would have surgical complications (based on previous research data); that 70% to 80% of surgeries would be DTG surgeries; and that 10% of the variability in surgery time would be explained by other predictors. Finally, we anticipated that 750 patients would meet our inclusion criteria and have complete data that were accessible through our electronic medical records. Under these conditions, a logistic regression model using a 2-sided α = .05 would have 80% power to detect a true increase in odds of complications between early and late surgeries of 1.67 to 1.78.
Results
We identified 1443 patients who were surgically treated for a hip fracture in 2005 to 2010. Of these patients, there were 584 exclusions (Figure 2).
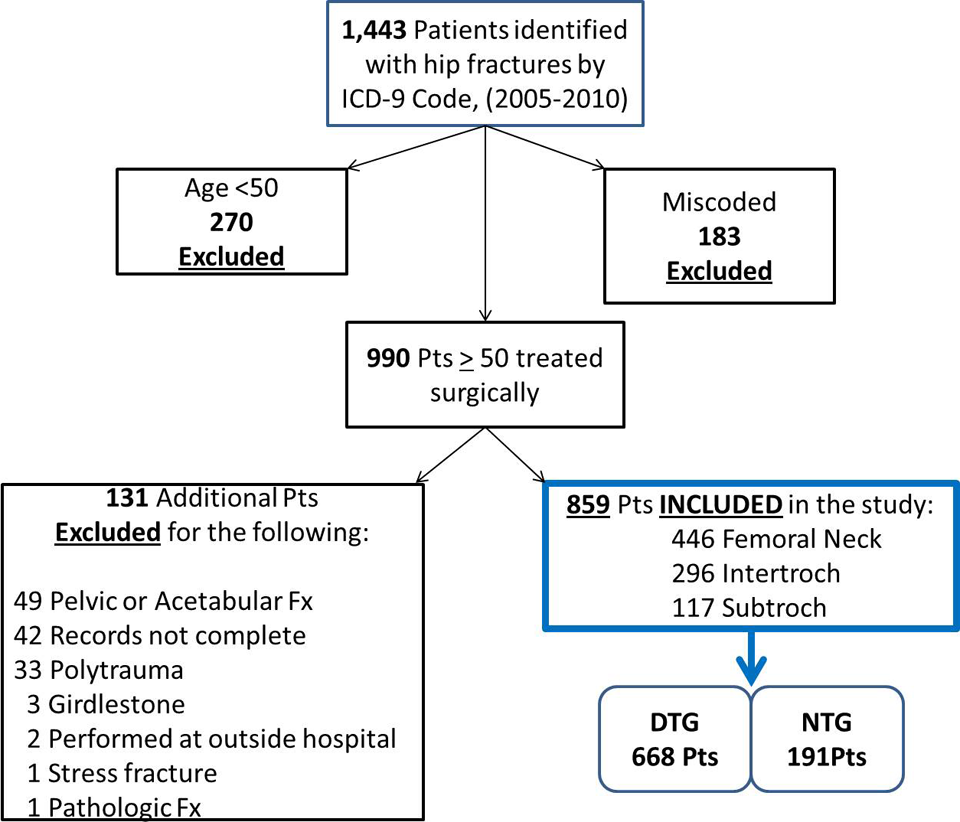
Patient cohort—retrospective chart review was performed for patients (
A histogram of surgical start time is depicted in Figure 3. Table 1 illustrates the characteristics of patients in the DTG and the NTG groups. A statistical difference existed in time to operation between DTG and NTG (DTG mean 26.8 hours vs NTG mean 21.2 hours, P = .0002), which was driven almost entirely by the tail of the distribution in the DTG, as the median time to surgery in both groups was similar (18.6 hours in the NTG vs 18.2 hours in the DTG).

A histogram of surgical start time shows that 668 patients underwent surgery in the daytime group (DTG) 07:00-15:59, while 191 underwent surgery in the nighttime group (NTG) from 16:00-06:59.
Patient Characteristics in the DTG and NTG.
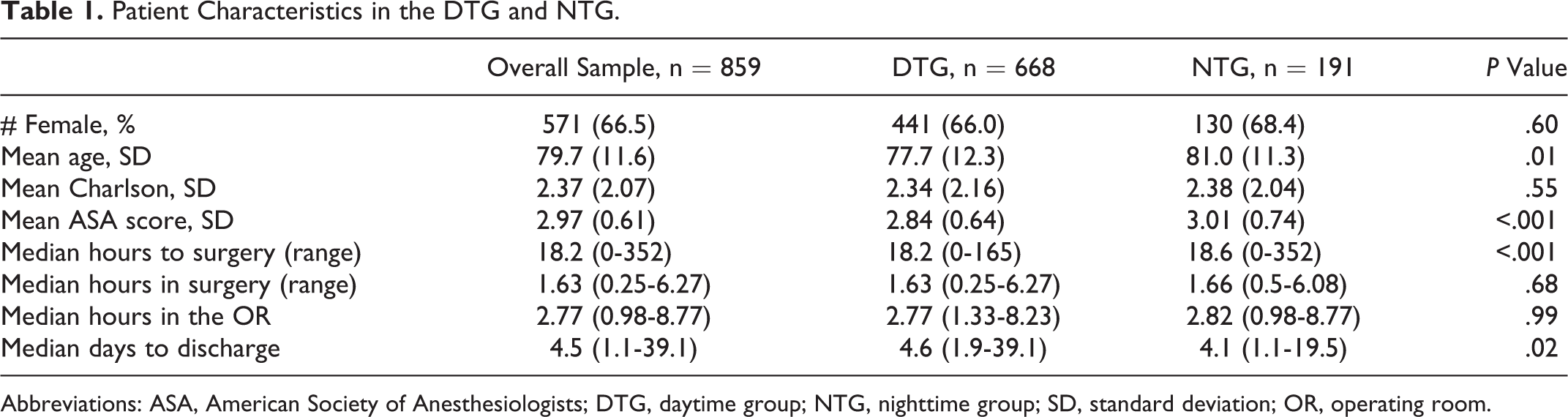
Abbreviations: ASA, American Society of Anesthesiologists; DTG, daytime group; NTG, nighttime group; SD, standard deviation; OR, operating room.
Four-hundred and ninety-seven (57.9%) patients required a transfusion either intraoperatively or postoperatively. Of those patients requiring a blood transfusion, the most common number of transfused units was 2, but ranged from 1 to 12, with a mean of 2.71 units. The patient who received 12 units of packed red blood cells underwent open reduction and internal fixation of a highly comminuted peritrochanteric fracture using a proximal femoral locking plate. A total of 51 (5.9%) patients required a transfusion of 3 or more units of packed red blood cells, 43 (6.4%) patients in the DTG, and 8 (4.2%) patients in the NTG (P = .299; Table 2).
Complications by DTG and NTG.a
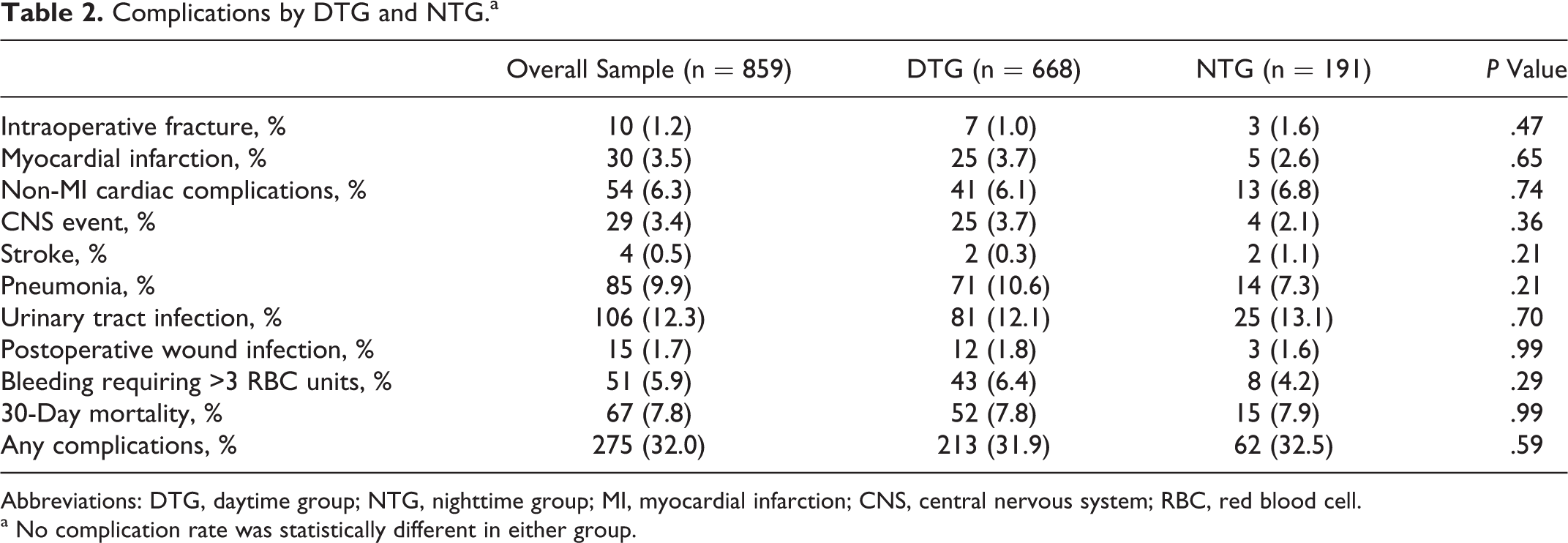
Abbreviations: DTG, daytime group; NTG, nighttime group; MI, myocardial infarction; CNS, central nervous system; RBC, red blood cell.
a No complication rate was statistically different in either group.
There was no statistical difference in 30-day mortality based on surgical start time (P = .503). There were 67 deaths documented within 30 days of surgery, which resulted in an overall 30-day mortality rate of 7.8%. The 30-day mortality rate in the DTG was 7.8% versus 7.9% in the NTG, which was not statistically significant, and, in fact, was distributed exactly as would be expected if sampling error was the only source of differences between the 2 groups (P = 1.00; Table 2). The finding of no difference remained when adjusting for ASA score, CCI, and age in multivariate logistic regression (odds ratio 0.899, CI 0.475-1.699). There was a trend toward increasing mortality with prolongation of time from admission to surgery, but this was not statistically significant (P = .091). However, in our cohort, 96% of the patients were treated within 72 hours of admission.
Complications are shown by DTG and NTG in Table 2. Total complication rate was 32.0% (275 complications recorded). Complication rate in the DTG was 31.9% (213 of 668) compared with 32.5% (62 of 191) in the NTG, which was not statistically significant (P = .920; Table 2). The odds of complications between groups were also not significantly different between DTG and NTG when adjusted for ASA score, CCI, and age (odds of complications were 0.877 in the DTG compared to the NTG, CI 0.608-1.266, P = .484). The most common complications were UTI (12.3%), pneumonia (9.9%), cardiac event other than MI (6.3%), and transfusion requirement of >3 units (5.9%). There was no increased risk of any complication type based on surgical time of day.
We used multivariate logistic regression to determine which predictor variables captured by our records best predicted complications and death. Of 4 models analyzed, the greatest predictors of adverse outcomes (mortality and complications) were age, ASA score, and CCI. Surgical time of day was not predictive of adverse outcomes (Figure 1).
Discussion
Patients who sustain hip fractures have high complication and mortality rates. In 1997, Aharonoff et al reported an in-hospital mortality rate of 4% and a 1-year mortality rate of 12.7% in patients with hip fractures more than 64 years old. 10 Factors predictive of mortality were patient age greater than 85 years old, preinjury dependency in ADL’s, a history of malignancy, ASA rating of 3 or 4, and the development of one or more in-hospital postoperative complications (relative risk [RR] = 4.1). In a cohort of 43 165 patients with hip fracture treated in the Veteran’s Administration Hospital system, sex (male), heart failure, liver disease, and increasing frailty were factors that contributed to an increased 1-year mortality—as high as 30% in men. 24 Sex, race, and impaired renal or cardiac disease have also been shown to predispose to poorer outcomes and increased mortality. 25 -27
Many authors have therefore focused on factors that may decrease complications and improve mortality following hip fracture surgery. 15 -19 Time to surgery, in particular, has attracted considerable attention. Zuckerman et al found that an operative delay of more than 2 calendar days doubled the 1-year mortality risk. 20 Simunovic et al showed a decreased 30-day, 6-month, and 1-year mortality rate in patients treated within 72 hours of admission, (RR 0.90, 0.87, 0.55 respectively). 21 Decreased postoperative complications, improved return to independent living, and reduced hospital length of stay have also been reported. 22,23 This information is now widely disseminated, and early surgical stabilization and mobilization of patients with hip fractures has become the standard of care.
Prior to surgery, however, many patients with hip fracture require medical optimization that may delay their surgical start time.
28
In addition, delays due to surgeon and OR availability may result in the treatment of many of these fractures at night.
28
-30
Several studies in the general medical literature have shown that after-hours surgery has led to a higher rate of complications.
31
Eastridge et al demonstrated that sleep deprivation significantly increased the time to complete a task and the number of errors performed using a laparoscopic simulator.
32
Kelz et al showed that vascular and general surgeries performed at a Veteran’s Administration Hospital starting between 4
In the orthopedic literature, Ricci et al found that nighttime fixation of femoral shaft fractures with an intramedullary nail was associated with an increased frequency of unplanned future surgeries (27% vs 3%). 36 More recently, Chacko et al found an increase in total surgical time when hip fractures were treated at night. 37
In addition to fatigue, reduced staff availability and familiarity with the surgery are other theories proposed for increased operative risk at night. This is supported by Foss and Kehlet who showed that 5-day mortality and 30-day mortality in patients with hip fracture were significantly higher in patients admitted during holiday periods, with reduced staffing, than during weekdays and weekends. 38
We therefore hypothesized that there was a significant increase in 30-day mortality and complications in patients with hip fractures treated surgically at night rather than during daytime hours. In our present study, however, we found no difference in 30-day mortality or complications based on the time of day the surgery was performed. (P = 1.0, .92 respectively) Our 30-day mortality was 7.8%, and our overall complication rate was 32%. In our study population, there is high variation between both patients’ health status and the technical demands of the surgical procedures (a total hip arthroplasty can be more technically demanding than percutaneous fixation of a hip fracture). To control for health status, we collected ASA score, CCI, age, and sex. 15,41 The 2 groups were homogenous in these regards, although ASA score and age were slightly lower in the NTG (2.84 vs 3.01, and 77.7 vs 81.0 respectively). To control for variation in surgical complexity, we collected information on both fracture type and type of surgery performed. After controlling for these variables, no significant differences were noted.
We chose our groups (DTG: 7:00-15:59 and NTG: 16:00-06:59) because they corresponded with our OR staff work hours and
We investigated several different ways of looking at time of surgery, including treating it as a continuous rather than a dichotomous variable. In no case was there an association between surgery time and complication rate. In other words, at no time period (for example whether 4

A Kaplan-Meier plot of hospital length of stay (LOS) by surgical daytime group (DTG) and nighttime group (NTG) illustrates that patients in the DTG had a longer length of hospital stay compared to those in the NTG.
Interestingly, patients treated in the NTG had a shorter time to surgery and shorter length of stay than patients treated in the DTG. This can be explained by the admission time of patients. In our cohort, the majority of patients were admitted during daytime hours. These patients had been treated at night of their admission, they would have had a shorter time to surgery and overall shorter length of stay than patients who waited until the next morning for their surgery (Figure 4). This is consistent with the existing literature on dedicated trauma rooms. 42 Wixted et al showed that the median delay between admission and surgery increased from 5.7 hours to 10.9 hours after implementation of a trauma room. 44
Delayed time to surgical fixation for hip fractures increases morbidity and mortality and decreases future function. 15,12 -27,46 Our study confirmed this. Increasing time to surgery led to an increasing number of complications (P = .0492) and a trend toward higher mortality (P = .091). This did not reach statistical significance most likely because there were few patients in our cohort treated after 36 hours from time of admission. Orosz et al demonstrated that while surgery <24 hours from admission does not lead to improved mortality or locomotion postoperatively, it does lead to decreased time in severe pain and decreased overall length of stay. 46 Siegmeth et al also showed that operating within 48 hours led to a significantly decreased length of stay. 18 In our study, the difference in the time to surgery between groups was relatively small. However, as there was no demonstrable increased risk of surgery in the NT group, we see no compelling evidence to wait for surgery as long as the patient is medically optimized.
Recently, increased scrutiny on hospital resource utilization has uncovered a systemic problem with “patient flow”; hospitals operate most efficiently when patient volumes are stable. Times of high hospital volume can lead to medical errors, while less busy times can lead to a waste of resources. 47,48 This variation results primarily from variability in the elective OR schedule rather than from emergent cases. 47 -49 To avoid this, several large institutions have made successful structural changes to their elective OR schedules based on the principle of “smoothing,” scheduling cases in the OR such that case volumes are consistent on a day-to-day basis, with good results. 50 This scheduling strategy may become increasingly common as strain on resources continues, and hospitals employ more surgeons. Our study demonstrates that hip fracture cases can be safely performed by surgeons when the OR becomes available, including after hours.
In our cohort, age, CCI, ASA score, and total OR time were all predictive of adverse events. We were able to quantify this risk as demonstrated in Table 3. Our results are consistent with a recent review of the Danish national registry by Daugaard et al who found that ASA score, sex, and age significantly affected the in-house and 30-day mortality of patients with hip fracture. 51
Logistic regression was used to assess the degree of association between complications and other measured covariates.

Abbreviations: ASA, American Society of Anesthesiologists; AM, After Midnight; IT, intertrochanteric; ST, subtrochanteric; ORIF, open reduction and internal fixation; OR, odds ratio. Note: Increasing age, Charlson comorbidity score, ASA score and times to operation were associated with higher complication rates, while total hip arthroplasty was associated with lower complication rates. Female sex showed a trend toward lower complication rates (P = .09) but was not significant at α = .05. Other covariates were not associated with the complication rate in this sample. Odds ratios for combined adverse events after surgery.a
Unfortunately, over the last 20 years, mortality and complication rates following hip fractures have not significantly improved. 7,10,24 The results of our study may facilitate communication with patients with hip fracture and their families.
There are several limitations in this study. First, this is a retrospective study. Therefore, there are many confounding variables. We addressed this by analyzing ASA score, CCI, age, fracture type, surgery performed, and sex. Second, we include only adverse events that were recorded in the chart, so if complications were not correctly entered, they would have been missed in our review. Third, our study was performed at a high volume, teaching, Level I trauma center that has focused on the optimization of geriatric hip fracture care and has a hospital wide multidisciplinary geriatric hip fracture team and dedicated orthopedic trauma OR. The surgeons and surgical teams may be more accustomed to operatively managing hip fractures at night than at a community hospital that does not have a similar focus on trauma and perioperative patient optimization. Forte et al showed increased inpatient and 30-day mortality in patients with hip fracture treat at lower volume institutions. 7 Therefore, our results may not remain consistent at hospitals where hip fracture volume is low. Fourth, our follow-up was limited to 30-day mortality and complications.
Conclusion
Our study demonstrates that operating after hours at a Level 1 trauma center, optimized for hip fracture care did not increase the risk of adverse events surrounding hip fracture surgery. We found no difference in 30-day mortality or complications based on the time of day the surgery was performed. To provide optimal surgical care of patients with hip fracture, early operative intervention should be undertaken, and operating after normal OR hours is a safe and reasonable option to facilitate this goal. Age, ASA score, CCI, and total OR time are all predictive of adverse events and can be used to facilitate the discussion of the risks and expectations of hip fracture surgery with patients and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.