
Abstract
Background:
Orthotic interventions for knee osteoarthritis (OA) aim to reduce mechanical loading on the medial compartment of the knee and may lessen the lateral trunk lean as the most important compensatory gait strategy. The lateral wedge insole is a known orthotic intervention for knee OA. However, the question whether the addition of a subtalar strap to the wedge improves its effect has not been addressed in the literature.
Objective:
To compare the effects of lateral wedge insoles, with and without a subtalar strap, on the lateral trunk lean in patients with knee OA.
Methods:
Twenty-three patients aged over 40 years, with grade I or II OA of the medial compartment of one knee, based on the American College of Rheumatology criteria, were included in this study. The patients were diagnosed with OA based on a clinical examination, and the diagnosis was confirmed with radiographs. A 3-dimensional motion measurement system was used to collect the gait data for 3 different conditions: (1) with no insole, (2) with a lateral wedge insole, and (3) with a lateral wedge insole and a subtalar strap. The immediate effect of the 3 test conditions on the lateral trunk lean was compared during a gait cycle a stance phase and at the point of midstance.
Results:
Based on the laboratory coordinate system, the 3 conditions had no significant effect on the lateral trunk lean during a gait cycle and a stance phase and at the point of midstance in patients with knee OA.
Conclusion:
The results of this study demonstrated that the lateral wedge insoles, with and without a subtalar strap, had no immediate effect on the lateral trunk lean in patients with knee OA. However, the long-term effect of lateral wedge insoles on the lateral trunk lean in these patients requires further investigation.
Introduction
Knee osteoarthritis (OA), as the most common type of arthritis, 1 is one of the main causes of chronic musculoskeletal pain and disability in the elderly western population. 2 The average annual economic burden of disabling hip and knee OA is reported to be $12 200 per individual, 3 and it mostly occurs in the elderly population. 4 Surgery is the only solution in advanced stages of OA; however, surgery is associated with risks in the elderly population. 5 Therefore, noninvasive methods to alleviate symptoms or slow down the progression of OA are of vital importance. 6 Noninvasive management of mild and moderate knee OA with a laterally wedged insole (LWI) is one of the most established approaches 7 ; previous studies that determined its efficacy in the reduction in the knee adduction moment 8–10 through alteration of lower leg mechanical alignment and calcaneal valgus correction 11 support this approach.
Theoretically, it is possible that the degree of freedom in the subtalar joint absorbs part of the effectiveness of a LWI and thus movement of the talus inhibits part of the femorotibial valgus correction. 12 Therefore, to enhance the effect of a LWI, Toda et al in 200112 added a subtalar strap to the LWI for the first time to limit movement in the subtalar joint and ultimately restrain calcaneal valgus correction. They found that adding a subtalar strap provided more efficacious outcomes in patients with knee OA. It has also been considered to have a therapeutic effect resembling that of a high tibial osteotomy. 12,13
Patients with knee OA adopt different compensatory gait strategies 14 to reduce the load on the medial compartment of the knee and as a result alleviate the feeling of joint instability and pain. 15 As reported by Hunt et al, 16 the lateral trunk lean is one of the well-reported strategies for altering knee joint loading; various other studies support that the lateral trunk lean reduces abnormal loading on the medial compartment of the knee joint. 17,18 Therefore, we can assume that any intervention that affects knee OA could produce some effects on the compensatory strategies adopted by the patients. The lateral trunk lean has been employed in previous studies as an indicator of intervention results in knee OA and has been shown to be decreased after high tibial osteotomy. 19
Considering the aforementioned aspects, the purpose of the current study was to compare the effects of LWIs, with and without a subtalar strap, on lateral trunk lean in patients with mild, early knee OA.
Methods
Study Design and Recruitment
This is a cross-sectional study on patients with medial compartment knee OA. The participants were recruited from an outpatient orthopedic clinic located in a rehabilitation hospital, based on physician referrals from November 2010 to January 2011. Ethics approval was obtained from the Human Research Ethics Committee of the affiliated university, and all the participants voluntarily signed a written and informed consent form.
Inclusion/Exclusion Criteria
Community-dwelling people diagnosed with medial compartment knee OA in 1 knee, based on the American College of Rheumatology criteria 20 and confirmation via radiographic images, were included in this study. The severity of OA was graded based on the Kellgren and Lawrence (K/L) grading system, 21 and the inclusion criteria were a K/L grade I or II as suggested by Shimada et al, 10 pain worse than level 3 on the visual analog scale (VAS), over 40 years of age, and presence of radiographic osteophytes in the joint space. The participants were excluded if they had undergone bilateral knee OA, had a K/L grade > II, secondary knee OA caused by trauma, history of knee joint surgery or other rare forms of arthritis, 18 significant knee joint ligament laxity, previous knee joint fracture, therapeutic knee joint injection in previous 6 months, disorders of the nervous system interfering with voluntary movements, perception disorder, chronic back pain, lower limb length discrepancy, orthotic treatment of the knee joint or foot, 9 body mass index (BMI) > 36 kg/m2, 8 hip joint or lumbar joints arthritis, hallux stiffness, midfoot valgus deformity, hind-foot arthropathy, foot ligament laxity, and flat foot or any other problems that restricted the use of an insole. Patients with valgus/severe varus malalignment or recurvatum of the knee, lateral compartment knee OA, and other problems that limited their independent walking ability were excluded.
The sample size for this study was 23 and was calculated using the G* Power package, with the power of 0.8 and the effect size of 0.25. 22 An extra 10% was added to cover possible dropout of participants; therefore, 25 patients with grade I or II of knee OA were recruited for this study. However, the data from 2 of the patients were incomplete due to missing markers. Hence, the data of 23 patients were used for statistical analysis.
Insoles
Bilateral noncustom, full-length, high-density ethyl-vinyl acetate insoles 8 that were covered by leather (Kish teb Aria, Tehran, Iran) were used in this study (Figure 1). The insole for the involved limb was equipped with a 5° full-length lateral wedge. 23 A no-wedge insole was used on the contralateral side to avoid leg length discrepancy. A medial arch support was embedded in both insoles. 24 Gymnastic shoes were employed to keep the insoles in the right place. The subtalar strap, which consisted of a 5-cm wide elastic strap (Teb & Sanat, Tehran, Iran), was twisted around the ankle joint of the involved limb in a figure of 8 shape and was fixed on the posterior aspect of ankle joint using velcro 12 (Figure 2). The insoles and straps were paid for by the research committee of the affiliated university.

A, Lateral wedge insole with leather covered. B, Neutral insole with leather covered.

Lateral wedge insole with subtalar strap.
Assessment of Knee Symptoms
A locally adopted version 25 of the Knee Injury and Osteoarthritis Outcome Score (KOOS) questionnaire was employed in this study. 26 This questionnaire is a 42-item disease-specific questionnaire with 5 subscales, including pain, symptoms, function in daily living (activities of daily living [ADL]), function in sport and recreation (sport/rec), and knee related quality of life (QOL), which are scored separately. For scoring each item, a Likert-type scale with 5 possible answer options ranging from 0 (no problem) to 4 (extreme problem) was used. The sum of the scores of the included items in each subscale is transformed to a 0 to 100 scale with 0 indicating extreme problems and 100 indicating no problems.
Gait Testing and Analysis
Each patient was examined on 3 occasions in random order (1) without insole; (2) with a LWI; and (3) with a LWI and a subtalar strap. Gymnastic shoes were employed on all 3 occasions. The measurements were taken after a short adaptation to each condition (approximately 5-10 minutes).
A 6 camera Vicon motion measurement system (460; Oxford Metrics, Oxford, UK) with a sampling rate of 100 frames/s (Hz) was used to collect the kinematic gait data. Participants were required to walk at a self-selected walking speed on an 8-meter walkway. Three successful trials were recorded for each participant in each condition. The participants were offered a rest break of 3 minutes between the trials and a rest break of 10 minutes between the conditions. Five passive reflective markers were placed on the patient’s skin over the right and the left acromioclavicular joints, the right and the left anterior superior iliac spines (ASIS), and the sacrum, midway between the posterior superior iliac spines by a wand. 16 Before testing the gait, a static trial was recorded to determine the orientation of the markers. Each trial was time normalized to 100% of the gait cycle. In this study, the intention was to assess the immediate effect of a LWI, with and without a subtalar strap to consider mechanical effects rather than neuromuscular adaptation. 27
Two-dimensional planar projection was used to calculate the lateral trunk lean angle. 16,28 The lateral trunk lean in each condition was calculated in 2 ways 28 : the lateral trunk lean according to the laboratory coordinate system (Figure 3A) and the lateral trunk lean according to the pelvic coordinate system (Figure 3B). The thoracic tilt, according to the laboratory coordinate system, was defined as the angle between the line connecting the midpoint of the acromion processes and the midpoint of the ASISs and the lab vertical axis. The thoracic tilt according to the pelvic coordinate system was defined as the angle between the lines used to measure the thoracic tilt according to the laboratory coordinate system and the frontal plane of the pelvis. All angles were calculated as the excursion of the thorax during a gait cycle and a stance phase of the affected limb, and at the point of midstance of the affected limb. The trunk lean angles according to the laboratory and pelvic coordinate systems were reported as being positive if the patient leaned over to the left limb during the stance phase. The walking speed was calculated as the projection of the ASIS marker of the affected limb through the walkway.
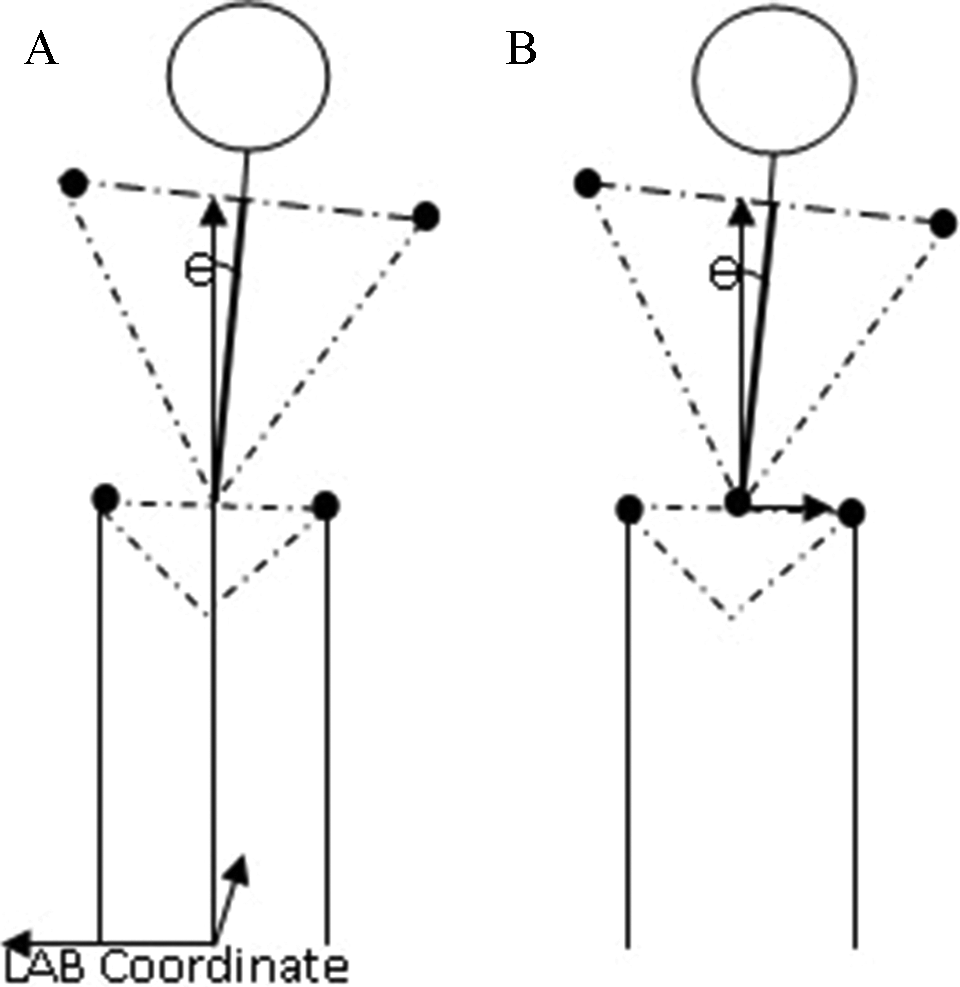
Two-dimensional planar projection of lateral trunk lean angle. A, According to laboratory coordinate system. B, According to pelvic coordinate system.
The gait data were averaged over 3 trials and processed via an in-house-written MATLAB program (7.0.4.365, R14, version 2.0). The differences between the 3 walking conditions (without insole, with a LWI, and with a LWI and a subtalar strap) were analyzed.
Statistical Analysis
Statistical calculations were performed using SPSS (Release 18 for Windows, 2009; SPSS Inc, Chicago), and all P values <.05 were considered statistically significant. Descriptive statistics were reported as mean and standard deviation (SD) if normally distributed or as median and range, if otherwise. The distribution of data was compared to normal by application of the one-sample Kolmogorov-Smirnov test for analysis. As normal distribution was assumed, the repeated measures analysis was employed to compare the mean of the dependent variables in the test conditions.
Results
Participants
The mean ± SD age and BMI of the participants (n = 23) were 46.65 ± 4.96 years and 31.63 ± 4.08 kg/m2 respectively. The average VAS pain score was 5.65 ± 1.69. No complaints of any adverse effects of LWIs were recorded during the tests. The patients’ pain, symptoms, function in daily living (ADL), function in sport and recreation (sport/rec), and the knee related QOL were assessed by the locally adopted version of KOOS. The results of the knee symptoms are shown in Table 1.
Presenting Score of Knee injury and Osteoarthritis Outcome Score (KOOS) Questionnaire Subscales.

Abbreviation: SD, standard deviation.
Gait Analysis
According to the laboratory and pelvic coordinate systems, the 3 conditions without insole, with a LWI, and with a LWI and an added subtalar strap had no significant effect on the lateral trunk lean during a gait cycle, a stance phase and at the point of 50% of the stance phase (Figure 4). Table 2 shows a summary of the statistics of the lateral trunk lean during the 3 conditions according to the 2 coordinate systems.
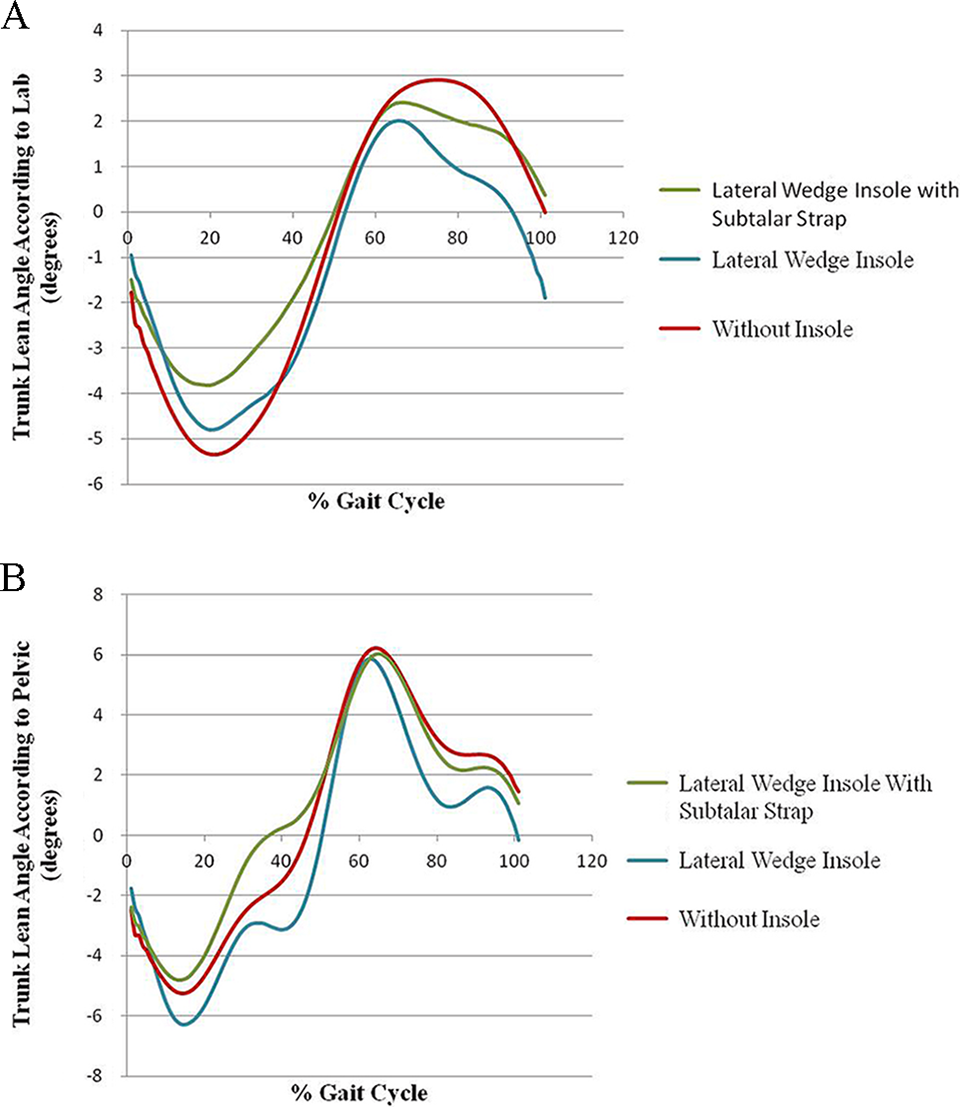
Lateral trunk lean angle. A, According to laboratory coordinate system. B, According to pelvic coordinate system. In 3 conditions: without insole, lateral wedge insole, and lateral wedge insole with subtalar strap, for one gait cycle of a patient.
Trunk Lean Angle (Degree) in Different Conditions and Coordinate Origins.

Additionally, the gait speed without insole, with a LWI and with a LWI and an added subtalar strap were 0.98 ± 0.12, 0.99 ± 0.12, and 0.97 ± 0.11 (m/s) respectively; the difference among these values was insignificant (P = .27).
Discussion
This study was conducted to examine the effect of a LWI, with and without a subtalar strap, on the lateral trunk lean in patients with knee OA. According to the results, use of a LWI, with and without a subtalar strap, had no significant effect on the lateral trunk lean in patients with knee OA.
The results of this study give the first insight into the immediate biomechanical effects of LWIs, with and without a subtalar strap, on the lateral trunk lean as a kinematic factor. This parameter is a strategy used by patients with knee OA to alleviate pain and modify abnormal medial compartment loading. 17 The findings of the current study are similar to the results reported by Kean et al in 2013, 29 who examined the effect of a modified walking shoe with a mild full-length lateral wedge in patients with knee OA.
In the literature, LWIs with and without subtalar strap have already been proven to be effective in decreasing pain and external knee adduction moment in OA. 9,13 Additionally, the frontal plane lateral trunk lean is shown to be effective in decreasing the adduction moment in the knee joint. 17 Therefore, it was expected that a LWI, with and without a subtalar strap, would decrease the lateral trunk lean. However, this was not found in our study, and a possible explanation for this could be that the lateral trunk lean may have become habitual for the patient and could not be changed in a short duration. At best, these are assumptions with no first level supporting evidence. 18 In the current study, participants had a short duration to get used to LWIs, with and without a subtalar strap, before the measurements were taken. Nevertheless, according to the previous studies, the effect of LWIs on the medial loading of the knee is an immediate one and did not change within 1 to 3 months. 8,30 Based on the current data, no conclusion about the long-term effect of LWIs can be made; however, Chang et al in 201119 reported significant reduction in trunk movement in the coronal plane in the fourth week after total knee arthroplasty. Despite this finding, total knee arthroplasty, which is one of the most common knee surgeries for reduction in knee pain, for correction of alignment and for improvement in some of the functions of the affected limb, is difficult to undertake owing to its invasive nature. 31 We should take into consideration the fact that conservative interventions, such as use of a LWI, that alter the load slightly are absorbable by other factors, and therefore, their effects may not be seen in the lateral trunk lean in the short term. In this study, no gait analysis was performed on lateralization of the center of pressure, external knee adduction moment, or other kinetic or kinematic parameters. Thus, a detailed analysis is needed to determine the parameters that might be required for the mechanical accommodation of gait. Additionally, gait adaptations may have a neuromuscular effect rather than a mechanical effect; as the immediate effects of LWI, with and without a subtalar strap, were evaluated in this study, only the mechanical effect was taken into consideration.
Another reason for the results of this study might be the addition of a medial arch support to the insoles. A previously conducted study reported that exhaustive and increased tension on the medial aspect of the foot are consequences of using LWIs without medial arch support for a long period of time. 32 Additionally, it was reported that local pressure on the foot soles is increased by use of flat insoles. 19 Considering these reports and the recommendation made in the study by Nakajima et al in 200924 that addition of an arch support to LWI decreased knee adduction moment more efficiently, LWIs with medial arch supports were used in the current study. However, in the studies that were published after the method of the current study was formulated, a nonsignificant reduction in external knee adduction moment by addition of a medial arch support to LWIs was reported. 32 One of the possible reasons for the controversy between the results of the studies by Nakajima et al 24 could be that Nakajima had recruited asymptomatic participants, who may have more adaptability to changes in their footwear compared with patients with knee OA. However, based on the findings of this study and a small number of other studies, it is doubtful whether addition of a medial arch support to the insoles is beneficial for patients with knee OA.
Furthermore, in previously conducted biomechanical studies, 5% to 10% reduction in knee adduction moment was found to be an immediate effect of LWIs, 8,23 whereas an increase of almost 10° in lateral trunk lean in healthy participants caused a 65% reduction in the knee adduction moment. 17 It seems that walking with increased lateral trunk lean has more potential for reduction in knee adduction moment than high tibial osteotomy (2-fold), 33 bracing, 34 and shoe modifications (6-fold). Therefore, it appears that noninvasive therapeutic interventions with a trivial effect (about 5° of wedging) could not affect the trunk owing to its relatively large mass, which contributes to about two-thirds of the body weight. The use of a LWI, with and without a subtalar strap, had no significant effect on gait speed, which is understandable, as a wedge alters the alignment of the tibia (while weight bearing in a close packed chain) mostly in the frontal plane and thus does not affect the speed of walking. This finding is similar to the results of a previous study. 9 Additionally, the population of this study is comparable to that of another study with regard to age and BMI. 16 Therefore, the results of the current study may be generalized, at least with regard to age and BMI.
This study has several limitations that should be considered when interpreting its findings. Based on a previous study that reported that LWI is efficient in patients with early and mild knee OA, 10 the study sample selected for this study included patients with grade I or II knee OA. Therefore, the results of this study cannot be generalized to more severe knee OA grades. The possible long-term effects of LWIs, with and without a subtalar strap, on lateral trunk lean and knee adduction moment were not considered in this study and will be addressed in the future.
In conclusion, the results of this study demonstrated that LWIs, with and without a subtalar strap, had no immediate effect on the lateral trunk lean angle. However, interindividual differences with regard to other kinetic and kinematic parameters, the most decisive factors for the mechanical accommodation of gait, have to be considered further. Additionally, long-term measurements and a larger sample size will allow a more general conclusion to be drawn.
Clinical Implications
When prescribing a LWI, with or without a subtalar strap, for knee OA, we should not expect any significant short-term effects on the kinematic symptoms.
Footnotes
Acknowledgments
The authors would like to thank Saeedeh Seyed-Mohseni of the Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, and Fatemeh Navab Motlagh, PhD candidate of Biomechanical Engineering, Biomedical Engineering Faculty, Amir Kabir University of Technology for their valuable technical help in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was fully funded by Tehran University of Medical Sciences research committee [grant number 14094-125-02-90]. This study was registered in IRCT (Iranian Registry of Clinical Trials) as required by the funding body and the registration number is: IRCT201104185520N4.