
Abstract
Introduction
The Björk procedure incorporates the right ventricle (RV) into the pulmonary circulation. 1 The idea behind this modification was to use the RV as a potential pumping chamber. This modification did not show an immediate haemodynamic superiority, or survival advantage over an atriopulmonary connection. However, RV growth was observed during follow-up in some patients, providing an RV-dependent pulmonary circulation.2,3 It has been demonstrated that a laminar flow, observed after atriopulmonary connection and total cavopulmonary connection (TCPC), causes structural vascular change and endothelial dysfunction in the long term, 4 whereas pulsatile flow reduces vascular resistance and increases lung perfusion. 5 Continuous flow may also lead to increased pulmonary vascular resistance. 6 Nowadays, survivors following the Björk procedure reach their fourth or fifth decade of life. They often present with late complications such as arrhythmia, ventricular dysfunction, thromboembolic events, or protein-losing enteropathy (PLE). 7 Our previous study demonstrated that patients with pulsatile pulmonary blood flow (PBF) showed a larger RV and better exercise capacity, compared with those with nonpulsatile pulmonary blood flow. 8
This study aims to compare further long-term outcomes in this cohort between Björk patients with a pulsatile pulmonary blood flow and those with a nonpulsatile PBF. We compared clinical presentations and hemodynamic findings between the groups. Finally, we analyzed the factors associated with pulsatile PBF.
Patients and Methods
Ethical Statement
This study was approved by the Institutional Review Board of the Technical University Munich (approved number of 2022-303-S-KH on June 27, 2022). Due to the retrospective nature of the study, the need for individual patient consent was waived.
Patients
We evaluated all patients who underwent the Björk procedure at the German Heart Center Munich between 1978 and 1995. All patients who survived longer than 15 years postoperatively and had their follow-up at our institution were included in this study. Medical records including the clinical status, physical examination, echocardiogram, cardiac magnetic resonance imaging (CMRI), and cardiopulmonary exercise testing were reviewed.
Surgery and Intervention
The Björk procedure was performed according to the original method 1 with some modifications (Figure 1). 8 Conventional TCPC conversion was done according to our previous study. 9 A valve implantation into the right atrium-RV (RA-RV) connection was performed at the time when patients needed a Fontan pathway revision and demonstrated a pulsatile PBF in order to recruit the RV and create a biventricular circulation. TCPC conversion was considered in patients without pulsatile pulmonary blood flow. Percutaneous valve implantation in the RA-RV connection was performed with either a Melody (Medtronic) or Sapien (Edwards Lifesciences) valve, if applicable.
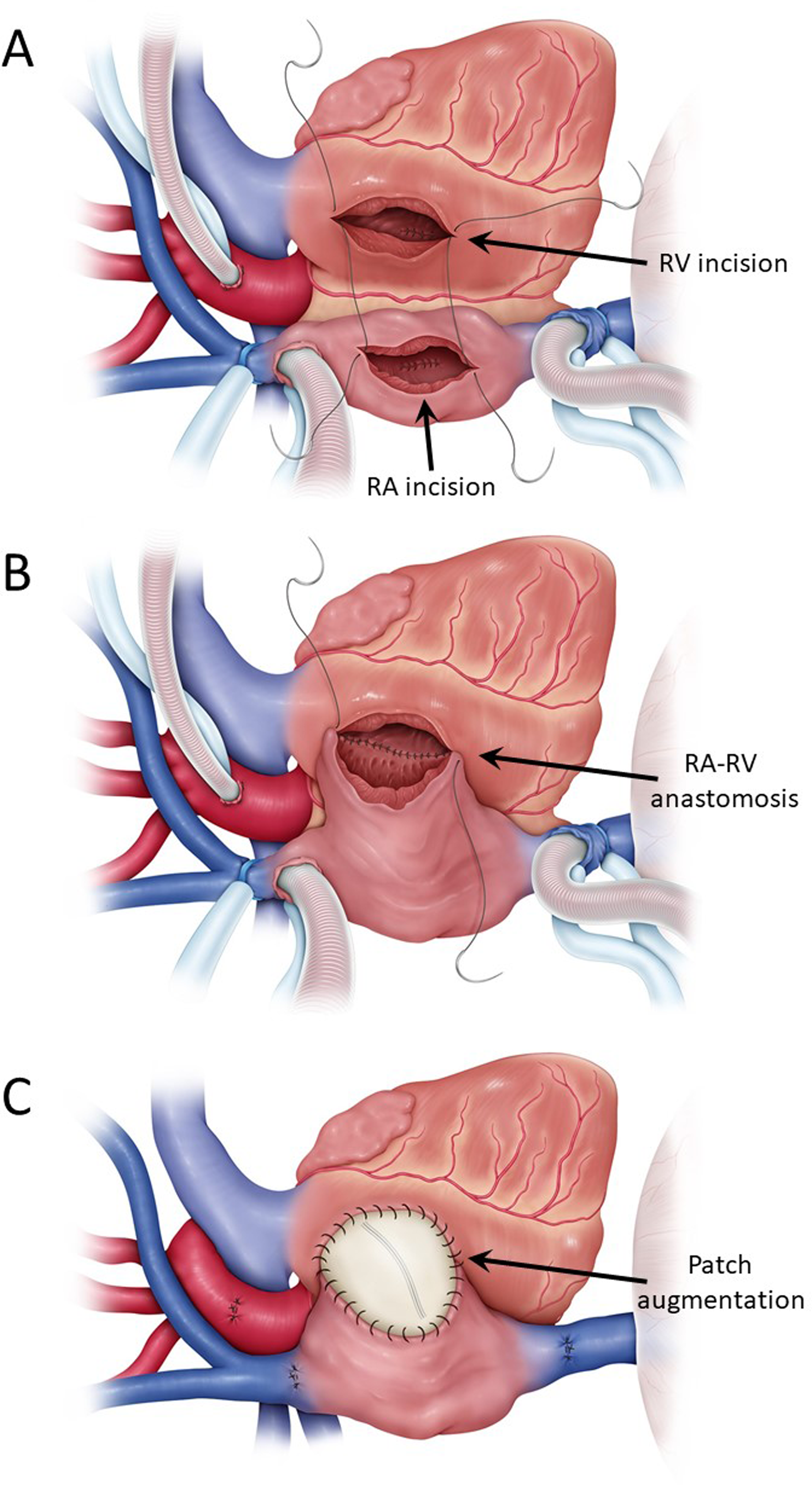
Depiction of the Bjork procedure. (A) After establishing cardiopulmonary bypass and cardioplegic cardiac arrest, RA, and RV are incised. ASD and VSD are closed through atriotomy and ventriculotomy, respectively. (B) RA and RV are directly anastomosed in the posterior side of the RA-RV connection. (C) Anterior side of the RA-RV connection was augmented with a Dacron patch. Abbreviations: ASD, atrial septal defect; RA, right atrium; RV, right ventricle; VSD, ventricular septal defect.
Echocardiography
Using the findings of echocardiography at 15 years postoperatively, the patients were divided into two groups based on the pulmonary flow patterns assessed by pulsed-wave Doppler. Group P (n = 13) consisted of patients who demonstrated pulsatile systolic flow, and group N (n = 30) which consisted of patients who did not. 8
Cardiac Catheterization
Cardiac catheterization examinations were performed when patients had clinical symptoms or echocardiographic findings. Pressure measurements were performed of the right atrium (RAP), pulmonary artery (PAP), right ventricle (RVP), and left ventricle (LVP). Additionally, Cardiac Index (CI) was calculated.
Cardiac Magnetic Resonance Imaging
Cardiac magnetic resonance imaging was performed on a 1.5 T whole-body scanner using a phase array cardiac coil. The right ventricular end-diastolic volume (RVEDV) and right ventricular end-systolic volume (RVESV) were measured. Then, the right ventricular ejection fraction (RVEF), RVEDV index (RVEDVI), RVESV index (RVESVI), and right ventricular stroke volume index (RVSVI) were calculated.
Cardiopulmonary Exercise Test
A symptom-limited cardiopulmonary exercise test on an electronically braked cycle ergometer (Ergoline) in the upright position was performed. Peak oxygen uptake (VO2) was defined as the highest mean uptake of any 30 s time interval during exercise. Age- and sex-related reference values (percent-predicted peak VO2) were calculated.
Statistical Analysis
Categorical variables are presented as absolute numbers and percentages. A χ2 test was used for categorical data. Continuous variables are expressed as medians with interquartile ranges (IQRs) or means with standard deviation (SD). The Student t test was used to compare normally distributed variables, and the Mann-Whitney test was used for variables that were not normally distributed. Overall survival was evaluated by the Kaplan-Meier method, and comparison between Group P and Group N was performed using log-rank test. Various factors were analyzed to find out whether there was an association with a pulsatile flow using logistic regression model. Data analysis was performed with SPSS 28.0 for Windows (IBM) and R statistical software 4.2.1 (R Foundation for Statistical Computing).
Results
We identified 66 patients who underwent the Björk modification at the German Heart Center Munich between 1978 and 1995. A flowchart of the selection criteria is shown in Figure 2. The causes of 14 deaths within 15 years are shown in Supplemental Table S1. Competing risk plots of death and reoperation in all 66 patients are shown in Supplemental Figure 1. Among 52 patients who survived more than 15 years postoperatively, 43 patients had follow-up examinations at our institution and were included in this study. Patients’ characteristics and operative variables are shown in Table 1. The median age at the Björk procedure was 5.7 (2.1-7.3) years. Diagnoses included tricuspid atresia (n = 39), tricuspid stenosis (n = 2), and double inlet left ventricles (n = 2). Ventricular septal defect (VSD) was closed directly without patch more frequently in Group P, compared with Group N (61% vs 27%, P = .03). No patient had a Glenn anastomosis prior to or at the Björk procedure.
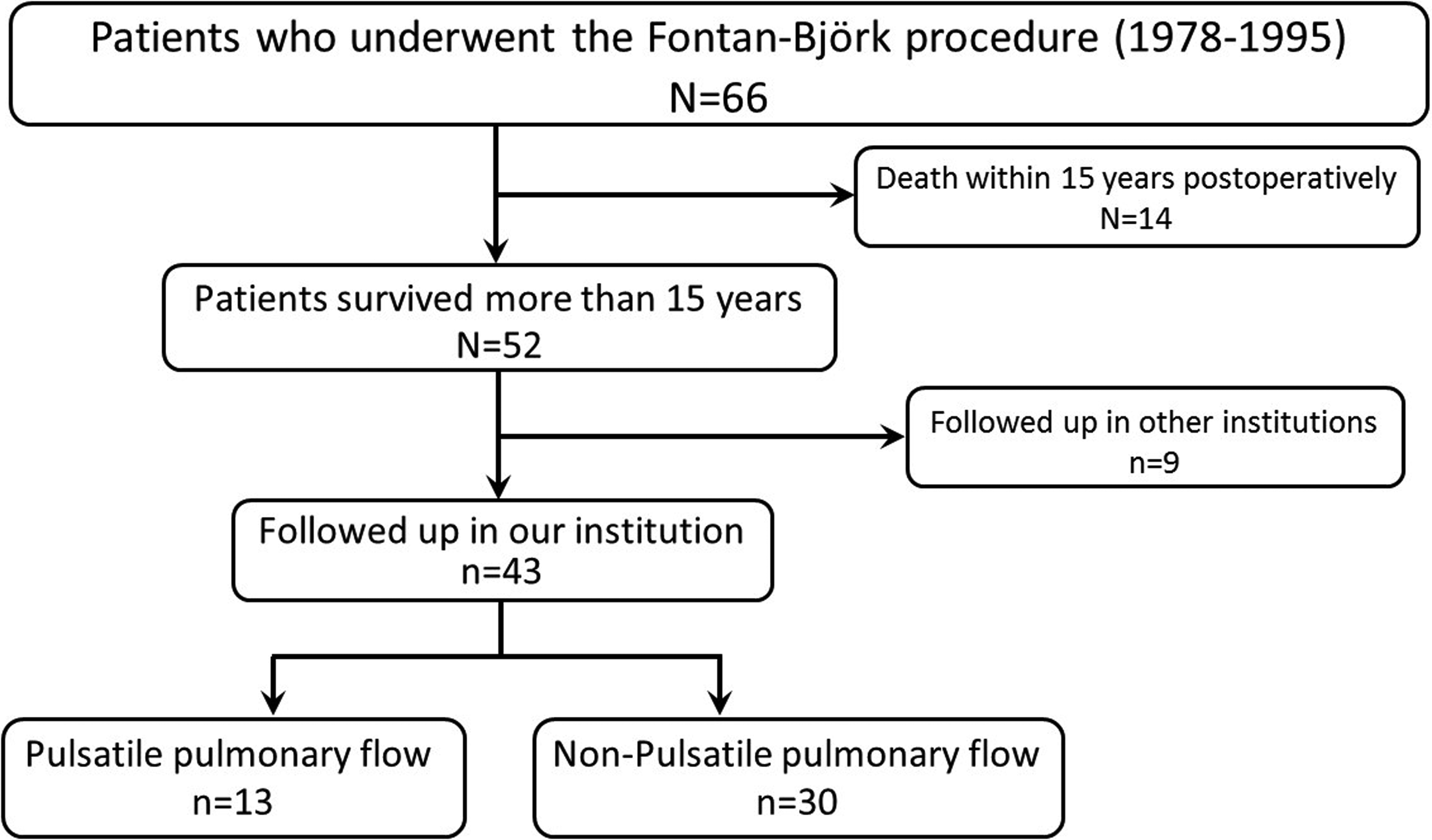
Flowchart showing patient enrolment.
Patient Characteristics and Data of Initial Björk Procedure.
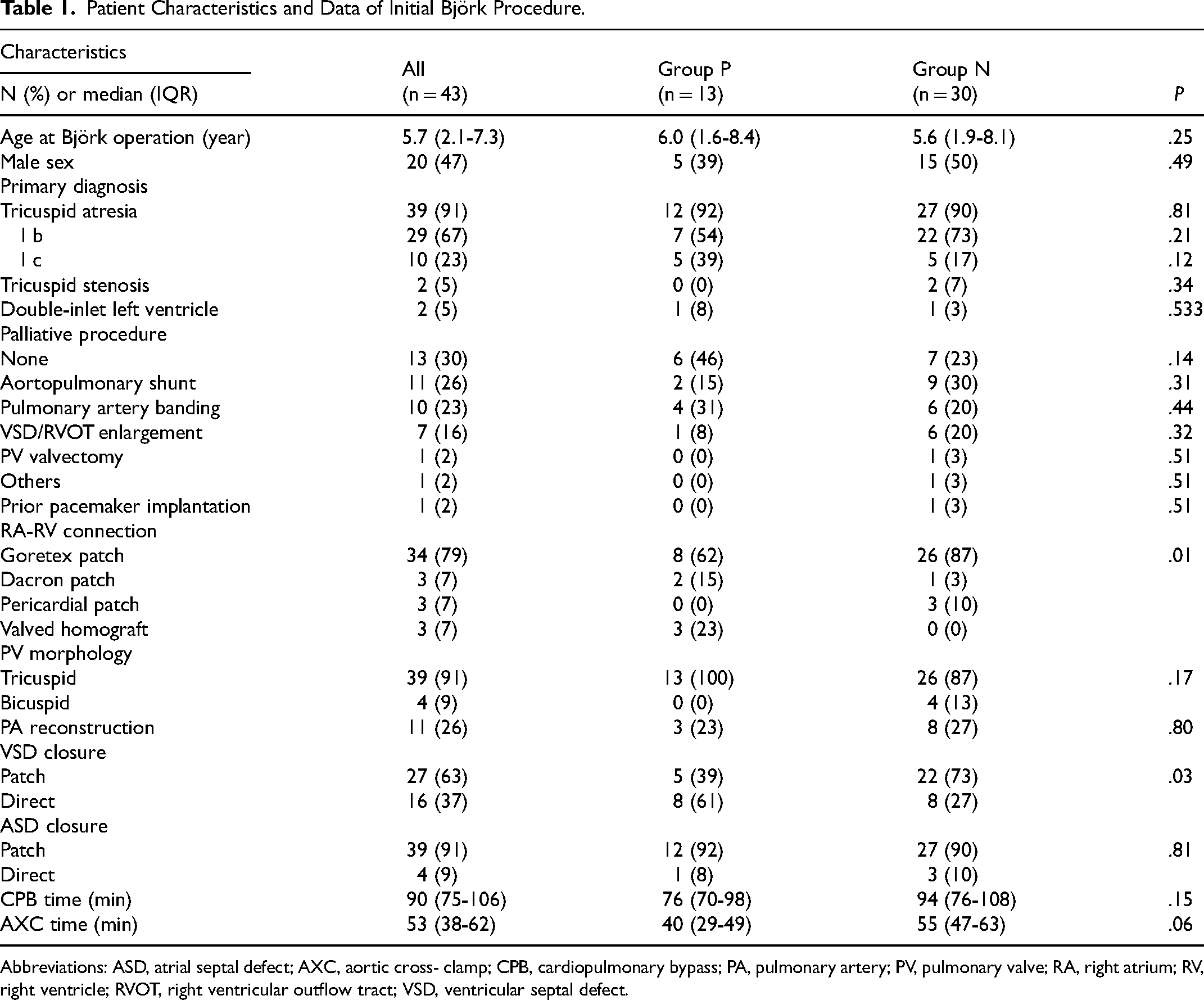
Abbreviations: ASD, atrial septal defect; AXC, aortic cross- clamp; CPB, cardiopulmonary bypass; PA, pulmonary artery; PV, pulmonary valve; RA, right atrium; RV, right ventricle; RVOT, right ventricular outflow tract; VSD, ventricular septal defect.
Late Mortality and Morbidities
Median follow-up since 15 years after the Björk procedure was 17 (IQR 13-21) years. There were seven late deaths occurring later than 15 years postoperatively, and all of them were observed in Group N. There was no heart transplantation. The estimated transplant-free survival in our study cohort of patients who survived more than 15 years postoperatively was higher in Group P, compared with Group N (P = .045, Figure 3).
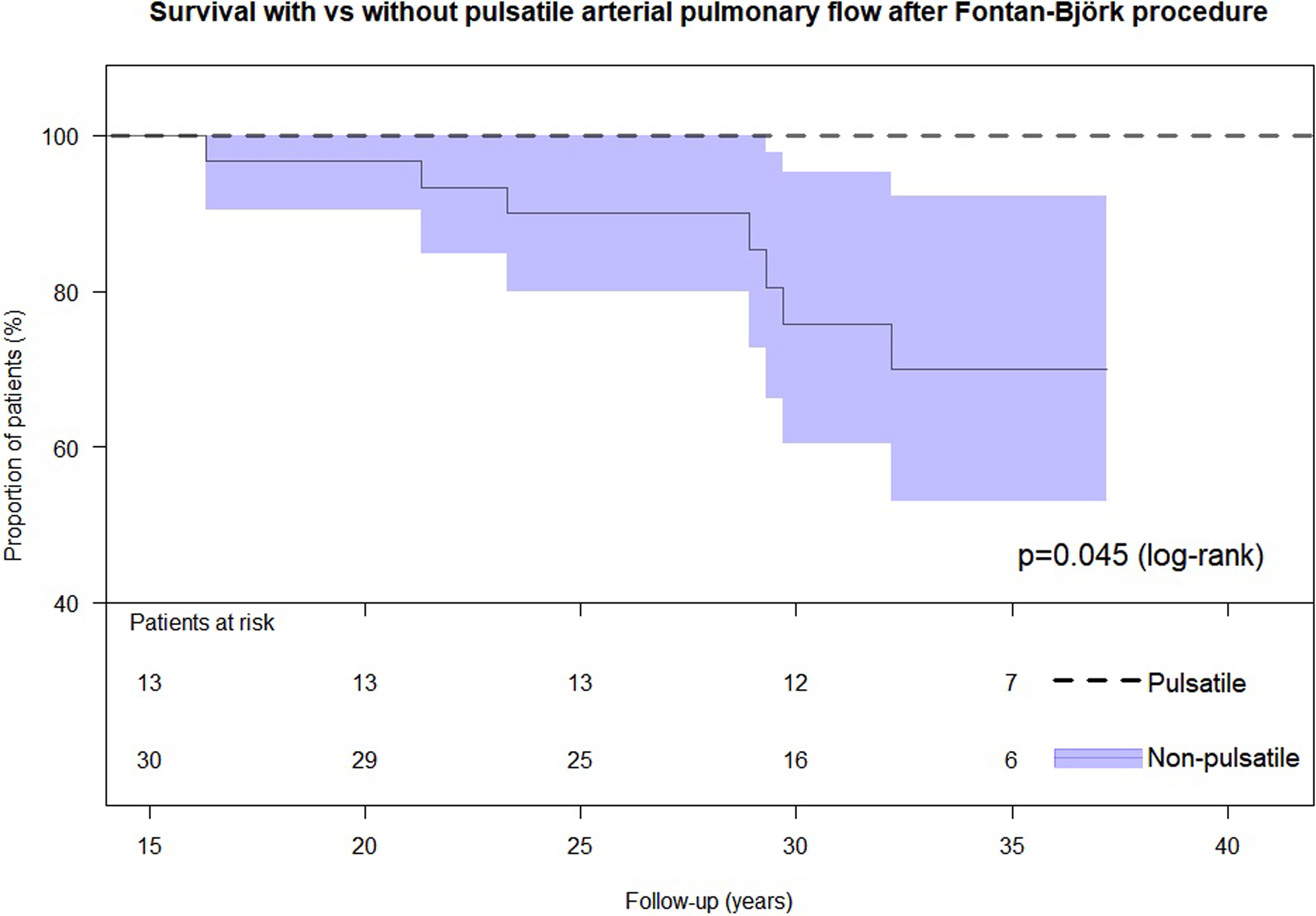
The estimated transplant-free survival in our study cohort of patients who survived more than 15 years postoperatively was higher in group P, compared with group N (P = .045).
The late morbidities are shown in Table 2. TCPC conversion was performed in nine patients including two patients in Group P (21.7 and 29.2 years postoperatively) and seven patients in Group N with median of 22.2 (21.3-24.3) years postoperatively. Surgical valve implantation into the RA-RV connection was performed in four patients in Group P (28.0, 29.4, 35.2, and 35.4 years postoperatively). Transcatheter valve implantation into the RA-RV connection was performed in four patients including two in Group P patients (21.4 and 29.4 years postoperatively) and two in Group N patients (25.3 and 31.0 years postoperatively). All nine patients after TCPC conversion and eight patients after surgical/interventional valve implantation into the RA-RV connection were alive at their last follow-up.
Patient Postoperative Data.
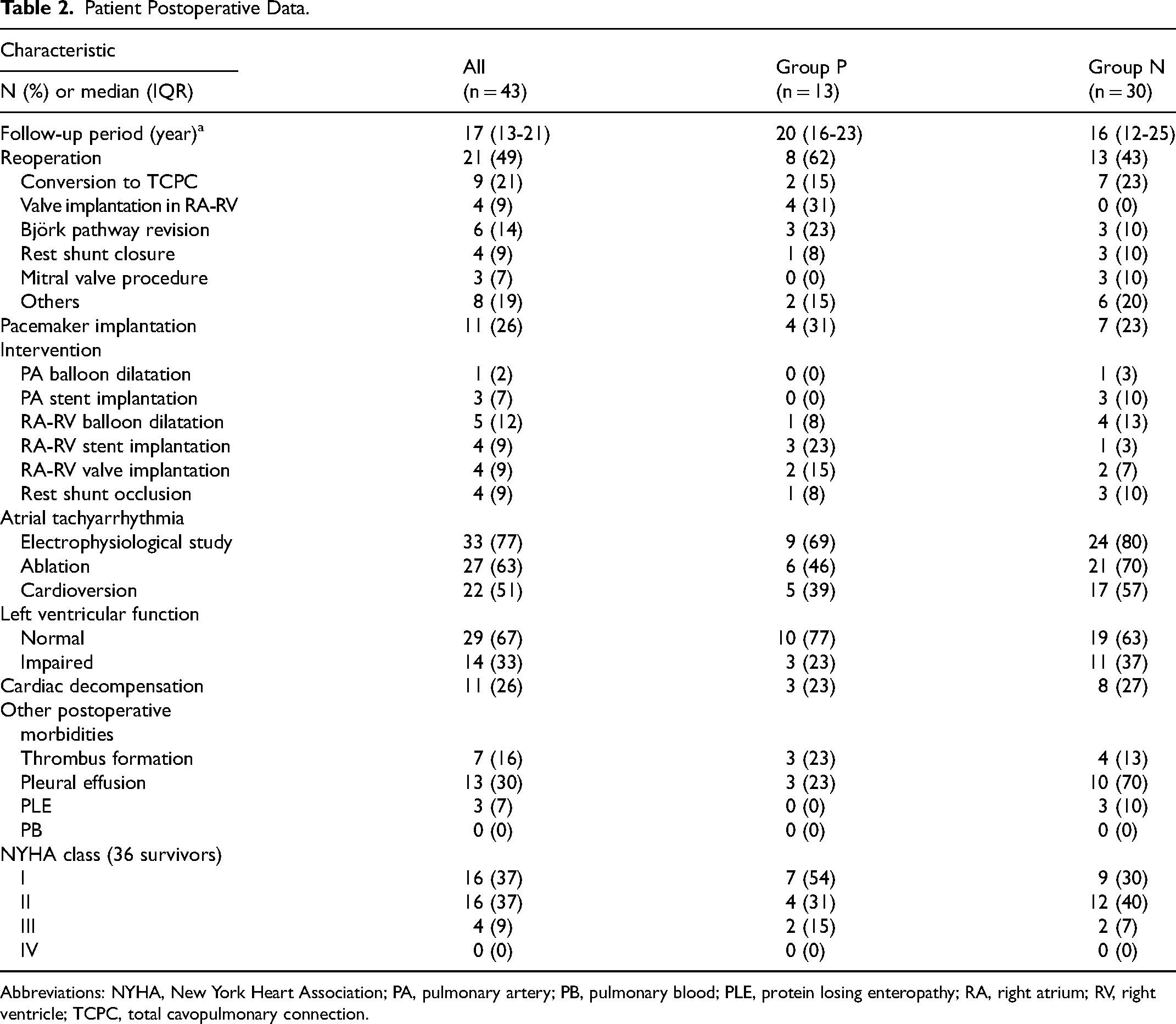
Abbreviations: NYHA, New York Heart Association; PA, pulmonary artery; PB, pulmonary blood; PLE, protein losing enteropathy; RA, right atrium; RV, right ventricle; TCPC, total cavopulmonary connection.
Hemodynamic Data
Cardiac catheterization was performed in 37 patients at a mean follow-up of nine years with the starting time being 15 years postoperatively (Table 3). Although there was no significant difference in systolic- (P = .181), diastolic- (P = .289), and mean PAP (P = .329), delta PAP (systolic PAP-diastolic PAP) was higher in group P than in group N (8.9 vs 5.4 mm Hg, P = .047). Cardiac Index was significantly higher in Group P, compared with Group N (3.5 vs 2.8 L/m2, P = .014).
Patient Hemodynamic Data.
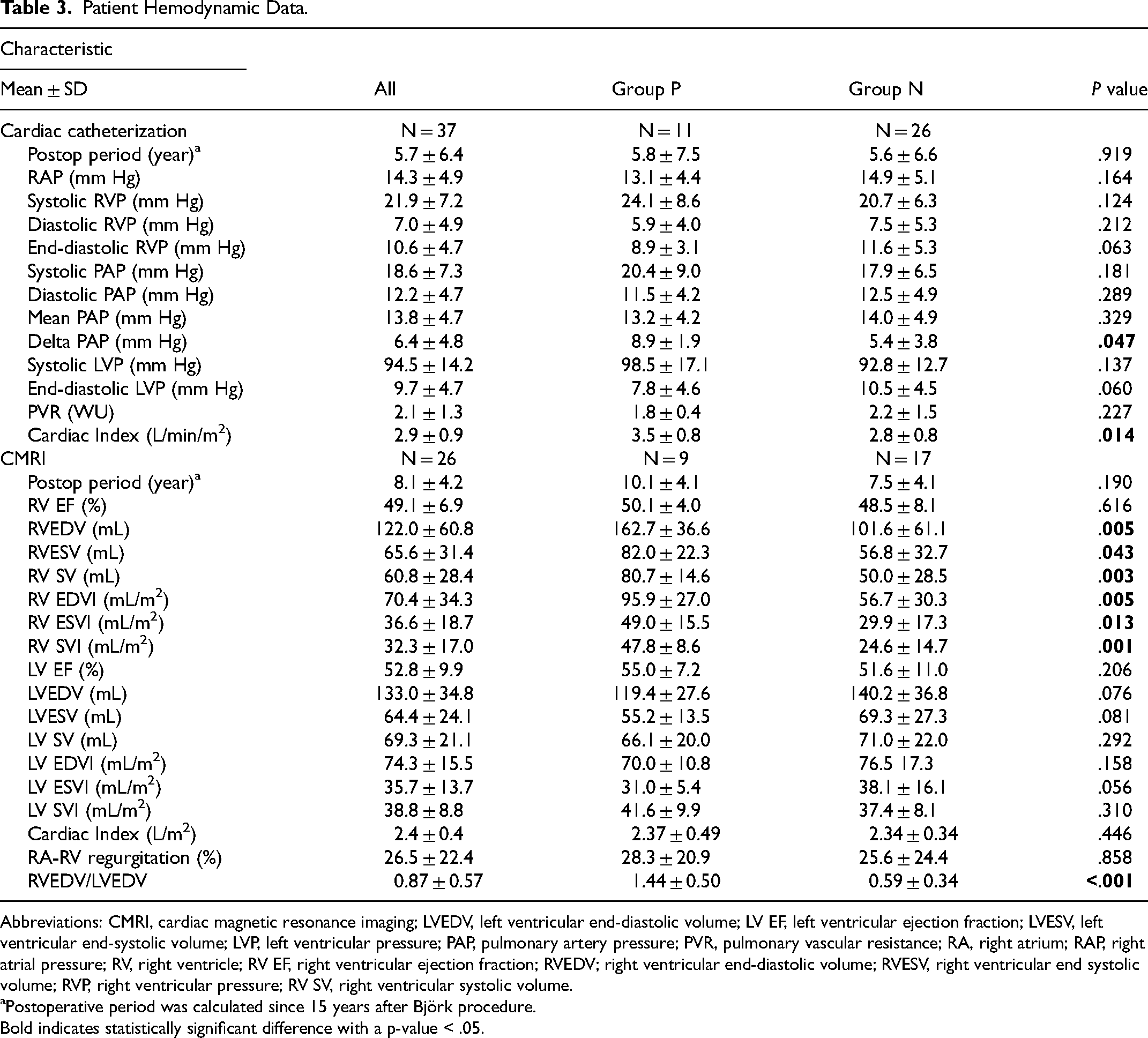
Abbreviations: CMRI, cardiac magnetic resonance imaging; LVEDV, left ventricular end-diastolic volume; LV EF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume; LVP, left ventricular pressure; PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance; RA, right atrium; RAP, right atrial pressure; RV, right ventricle; RV EF, right ventricular ejection fraction; RVEDV; right ventricular end-diastolic volume; RVESV, right ventricular end systolic volume; RVP, right ventricular pressure; RV SV, right ventricular systolic volume.
Postoperative period was calculated since 15 years after Björk procedure.
Bold indicates statistically significant difference with a p-value < .05.
Ventricular Volume Study by Cardiac Magnetic Resonance Imaging
Cardiac magnetic resonance imaging was performed in 29 patients at a mean follow-up of 12 years with a starting time of 15 years after the Björk procedure. Right ventricular end-diastolic volume (162 vs 101 mL, P = .005), RVESV (82 vs 56 mL, P = .043), RVSV (80 vs 50 mL, P = .003), RVEDVI (95 vs 56 mL/m2, P = .005), RVESVI (49 vs 29 mL/m2, P = .013), RVSVI (47 vs 24 mL/m2, P = .001), and the RVEDV/LVEDV ratio (1.44 vs 0.59, P < .001), were higher in Group P compared with Group N.
Exercise Capacity
Cardiopulmonary exercise tests were performed in 38 patients (68 examinations in 11 patients in Group P and 157 examinations in 27 patients in Group N) at a median follow-up of 24 (IQR 21-29) years postoperatively. Peak oxygen uptake (VO2) was higher in Group P (23.8 [18.8-28.1] mL/kg/min) compared with Group N (19.5 [15.5-24.5] mL/kg/min, P < .001). Percent predicted peak VO2 was higher in patients of Group P (76.1 [64.0-83.9] %) compared with Group N (59.0 [46.1-69.5] %, P < .001). Yearly distributions in percent predicted peak VO2 in individual Björk patients are shown in Figure 4.
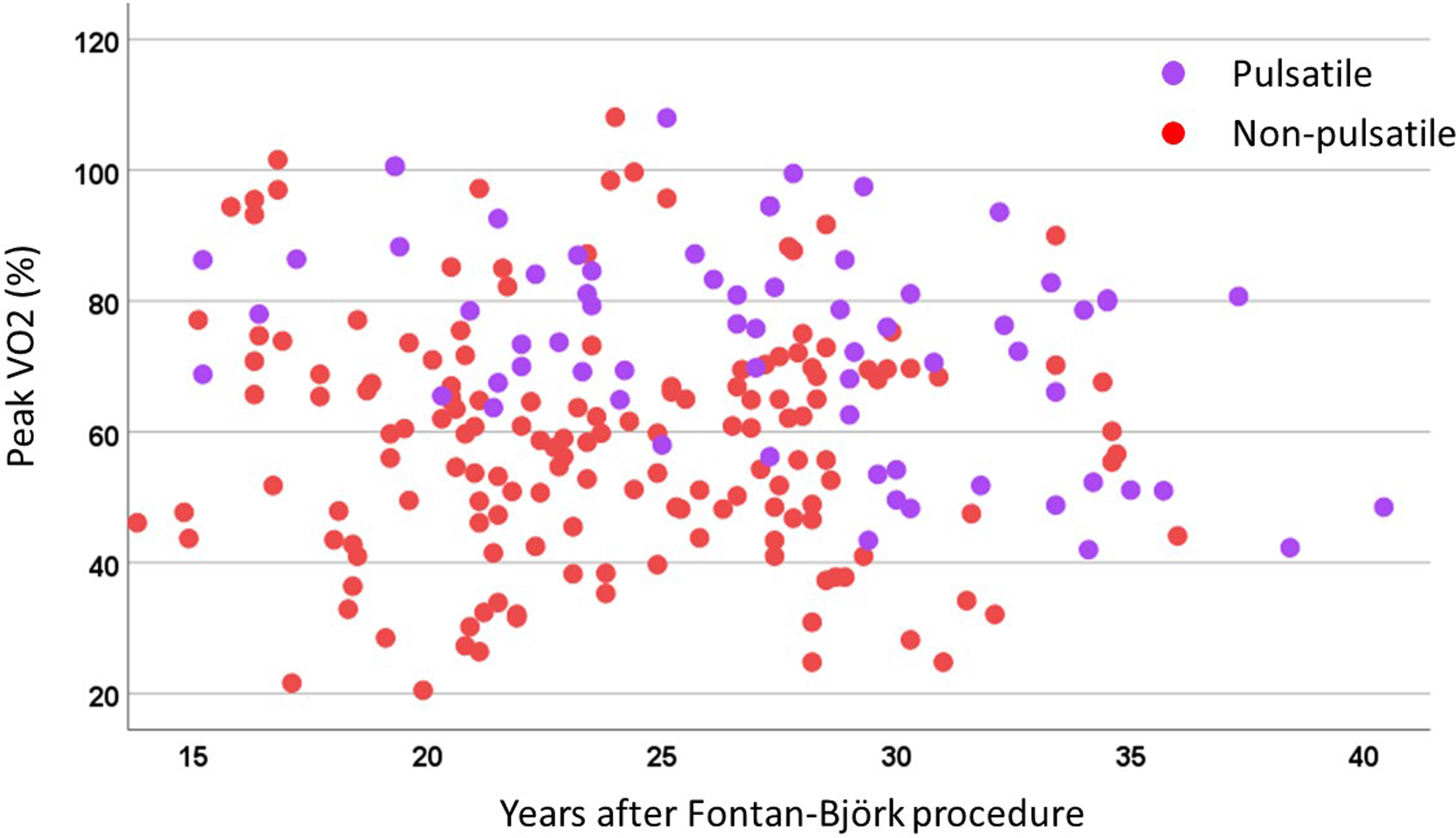
Changes in peak VO2 over time in Björk patients according to the presence (light grey) or absence (dark grey) of pulsatile pulmonary blood flow.
Factors Associated With Pulsatile Pulmonary Blood Flow
Direct closure of VSD (P = .035, OR: 1.400), higher RVEDVI (P = .056, OR: 1.062), higher RVESVI (P = .054, OR: 1.083), higher RVSVI (P = .091, OR: 1.327), higher delta PAP (P = .069, 1.176), higher CI (P = .041, OR: 3.047), larger RV size at last follow-up (P = .006, OR: 21.001), and no incidence of late arrhythmia (P = .039, OR: 0.208), were identified as associated factors with pulsatile PBF (Supplemental Table S2).
Comment
Patients with pulsatile pulmonary flow late after the Björk procedure had better survival compared with patients with nonpulsatile pulmonary flow. Furthermore, they showed better cardiac output, a larger RV size, and a better exercise capacity, compared with those with nonpulsatile flow.
Late Interventions for Right Atrium to Right Ventricle Connection
Right atrium-right ventricle graft/conduit dysfunction is a very common reason for symptoms after the Björk procedure. TCPC conversion is an option for these patients. However, valve implantation into the RA-RV pathway is an alternative to a TCPC conversion. Shah, et al demonstrated 16 patients who underwent transcatheter valve implantation into the RA-RV connection after the Björk procedure. 10 There were case reports describing a successful catheter-based valve implantation into the RA-RV connection.11–16 Surgically, Rybicka et al reported an exchange of the homograft located between the RA and the RV. 17 Several succeeding case reports showed reoperations of the Björk pathway using a bioprosthetic valve.18–20 In group P patients of our series, four interventional and four surgical valve implantations into the RA-RV connection were performed. Two patients underwent TCPC conversion; one patient received the TCPC conversion in the early era. At that time the concept of valve implantation into the RA-RV connection was not yet established. The other patient underwent a TCPC conversion in another clinic. In group N patients of our series, two interventional valve implantations into the RA-RV connection were performed in the early era. Specific criteria, when a valve implantation into the RA-RV connection was indicated, had not been established back then. In general, valve implantation into the RA-RV connection seems reasonable in patients with a sufficiently developed and well-functioning RV. Whereas in patients with a the small RV and nonpulsatile pulmonary blood flow, TCPC conversion should be an option if it is indicated.
Benefit of Pulsatile Pulmonary Blood Flow in the Long Term After the Björk Procedure
Our results demonstrated that patients with pulsatile pulmonary flow had no mortality and no incidence of PLE, whereas patients with nonpulsatile pulmonary blood flow had seven deaths and three cases of PLE. Cardiac catheterization data showed that delta PAP was significantly different between the groups. We assume that the energy generated by the RV in patients with pulsatile pulmonary blood flow to augment the forward flow to the pulmonary artery is low. However, even a small systolic pulsatile flow in the pulmonary circulation synchronized with the systolic motion of the left ventricle might be clinically relevant. The assistance of the RV to the pulmonary perfusion in patients with pulsatile PBF might be beneficial, especially during cardiopulmonary exercise. Therefore, recruiting the small RV in patients with tricuspid atresia and normal position of the great arteries should be reconsidered.
Reconsideration of Right Atrium to Right Ventricle Connection
The Björk procedure was abandoned in favor of the TCPC, mostly due to stenosis/regurgitation occurring in the RA-RV connection and unfavorable hemodynamics. While it is intuitive that a pulsatile flow could be beneficial for maintaining Fontan circulation in patients following the Björk procedure, one has to weigh in the disadvantages that it brings in practice: reoperations due to the progressive stenosis and/or regurgitation of the RA-RV connection, atrial tachyarrhythmia due to the dilation of the RA, thrombus formation, pleural effusion, and PLE. In this cohort, 33 (77%) of patients showed late atrial tachyarrhythmia.
However, nonpulsatile pulmonary flow might be the cause of late complications after the TCPC. Our results demonstrated that patients with pulsatile pulmonary flow had better survival and maintained better hemodynamics, compared with those with nonpulsatile flow. Therefore, in order to promote RV growth, the idea to integrate the RV into the pulmonary circulation could be reconsidered. Some of these patients could benefit from a Björk-type RA-RV connection and even show better long-term results than patients after a staged TCPC procedure. However, these results depend on the patients’ right ventricular growth and the development of a pulsatile pulmonary flow. It turns out to be problematic, that it is not possible to accurately predict whether the RV will grow after the RA-RV connection. Our analysis showed that direct closure of the VSD was positively associated with pulsatile pulmonary flow. We assume a direct closure of the VSD was predominantly performed on small VSDs. A small restrictive VSD might protect the pulmonary vasculature and provide a low pulmonary vascular resistance. These data suggest that a well-developed pulmonary artery might be the key element for RV growth. On the contrary, our analysis showed that the size of the RV at the time of the Björk procedure was not related to late pulsatile pulmonary flow. Ausari et al reported a patient with tricuspid atresia, hypoplastic RV, and normal pulmonary valves and arteries, in whom the Björk procedure was performed at eight months old, and a 27-mm bioprosthesis was placed in the RA-RV connection at 13 years old. 21 The RV grew to normal range and the patient had a biventricular circulation. These data suggest that even a hypoplastic RV might grow when other conditions are optimal.
Another concern is the substitute for the RA-RV connection. Historically, a homograft was used, but calcification/stenosis occurred relatively soon after the procedure. A valveless connection was performed in the late era. Although this modification prevented the early development of stenosis, late regurgitations/stenosis in the RA-RV connection were observed in the long term. Therefore, an ideal valved conduit is desired which has growth potential and durable valve function. A decellularized homograft might be a potential candidate.
Study Limitations
There are limitations due to the retrospective and observational nature of this single center study, due to the small group of patients and the high proportion of patients lost to follow-up. Much of the data or protocol for decision-making is lacking or unavailable, and therefore, a causal relationship-to-effect cannot be inferred, and only end observations can be made.
The length of follow-up is different, and differences observed between the two groups are not adjusted by possible confounders. The data of cardiac catheterization, CMRI, and cardiopulmonary exercise test were not available in all patients. Not being able to predict when a pulsatile flow is likely to be obtained is quite an important limitation of the technique.
Conclusions
Long term after the Björk procedure, patients with pulsatile pulmonary blood flow had a larger right ventricular volume and a better exercise performance, compared with those without pulsatile pulmonary blood flow.
Supplemental Material
sj-docx-1-pch-10.1177_21501351231205568 - Supplemental material for Long-Term Survival Is Superior in Patients With Pulsatile Pulmonary Flow After the Björk Procedure
Supplemental material, sj-docx-1-pch-10.1177_21501351231205568 for Long-Term Survival Is Superior in Patients With Pulsatile Pulmonary Flow After the Björk Procedure by Lukas Klemm, Thibault Schaeffer, Paul Philipp Heinisch, Helena Staehler, Christoph Röhlig, Christian Meierhofer, Nicole Piber, Alfred Hager, Peter Ewert, Jürgen Hörer and Masamichi Ono in World Journal for Pediatric and Congenital Heart Surgery
Supplemental Material
sj-jpg-2-pch-10.1177_21501351231205568 - Supplemental material for Long-Term Survival Is Superior in Patients With Pulsatile Pulmonary Flow After the Björk Procedure
Supplemental material, sj-jpg-2-pch-10.1177_21501351231205568 for Long-Term Survival Is Superior in Patients With Pulsatile Pulmonary Flow After the Björk Procedure by Lukas Klemm, Thibault Schaeffer, Paul Philipp Heinisch, Helena Staehler, Christoph Röhlig, Christian Meierhofer, Nicole Piber, Alfred Hager, Peter Ewert, Jürgen Hörer and Masamichi Ono in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Authors’ Note
The data underlying this article will be shared by corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.