
Abstract
Background:
Perinatal factors including gestational age, birthweight, size for gestational age, delivery route, maternal parity, maternal age, maternal education, socioeconomic status, race, and sex, are associated with the future risk of obesity and co-morbid conditions. This study evaluated the relationship of birthweight for gestational age and perinatal factors with severe obesity and dyslipidemia in adulthood.
Methods:
We conducted a population-based, retrospective birth cohort study of infants born to residents of Olmsted County, MN between 1976 and 1982. Outcomes were assessed after age 18 years until October 2020, including severe obesity (BMI ≥ 40 kg/m2) and dyslipidemia (total cholesterol ≥200 mg/dL, non-high density lipoprotein [non-HDL] cholesterol ≥145 mg/dL or HDL cholesterol <40 mg/dL). We obtained mother’s age, education level, and parity as well as newborn sex, race, type of delivery, single/multiple birth, gestational age, and birthweight from birth certificate data. Individual-level socioeconomic status (SES) of the household at birth was determined with the HOUSES index.
Results:
Of 10 938 birth cohort subjects, 7394 had clinic visits after age 18 years and were included, with 2630 having severe obesity (n = 798) or dyslipidemia (n = 2357) as adults. In multivariable models, female sex, singleton birth, less maternal education, and lower SES defined by HOUSES were independently associated with an increased risk of severe obesity in adulthood. Non-white race, singleton birth, and lower birthweight were independently associated with adult dyslipidemia. Birthweight for gestational age was not associated with severe obesity or dyslipidemia.
Conclusion:
Perinatal factors were associated with both severe obesity and dyslipidemia in adulthood. Lower SES at birth was predictive of severe obesity in adulthood, highlighting the opportunity to investigate modifiable perinatal social determinants to reduce the risk of severe obesity.
Introduction
The rise in obesity and comorbidities such as dyslipidemia are a public health crisis that has steadily worsened over the last 20 years.1,2 Research has also consistently shown that obesity and its comorbidities predispose individuals to conditions from diabetes to cancer.3,4 As these diseases have grown in importance, researchers have sought targets for preventing them. A convincing body of evidence shows the impact of birthweight on the later development of obesity and dyslipidemia.5-7
Scientists postulate that high birthweight indicates excessive nutrition in utero resulting in metabolic changes and predisposing the infant to obesity throughout its life.8,9 Conversely, researchers propose that low birthweight indicates fetal under-nutrition that leads to in-utero changes in glucose: insulin metabolism. It is thought that a combination of insulin resistance and parent over-feeding of small for gestational age infants predispose patients to diabetes, metabolic syndrome, and central obesity later in life.9-11 Though most existing literature has focused on substantiating the link between birthweight and pediatric metabolic diseases, a growing number of studies suggest the persistence of these associations into adolescence. 5 Fewer published studies show an association between birthweight and obesity and dyslipidemia in adulthood.8,12-14
Studies in Sweden have found a correlation between high birthweight and later obesity and other chronic illnesses.8,13,15 In contrast, some studies have shown a correlation between low birthweight and metabolic syndrome, insulin resistance, and central obesity in adulthood.16-21 Additionally, a few studies have shown a U-shaped or J-shaped relationship between birthweight and obesity, demonstrating correlations between both, high and low birthweight and obesity.22,23 Similarly, with regards to dyslipidemia, studies in Australia, Norway, and Spain show an association between low birthweight and dyslipidemia.24-27 Despite their strengths, these studies have limited generalizability due to non-representative study samples and their locations abroad.
The aim of this study is to evaluate the relationship of birthweight for gestational age and perinatal factors with long-term incidence of severe adult obesity and dyslipidemia in a United States cohort accounting for several infant and mother related variables, including socioeconomic status. We hypothesized that large for gestational age or small for gestational age would be associated with increased long-term incidence of severe obesity compared to normal birthweight for gestational age. We also postulated that small for gestational age would be associated with dyslipidemia.
Methods
Study Setting and Population
We conducted a population-based retrospective cohort study using the 1976 to 1982 Olmsted County birth cohort, which consists of 10 938 individuals born between January 1, 1976 and December 31, 1982 to mothers residing in Olmsted County, Minnesota at the time of the child’s birth. 28 Olmsted County is located in southeast Minnesota and as of the 1980 census there were 92 006 residents, of which 98% were white. As of the 2000 census, 91.1% of individuals 25 years and older had a bachelor’s degree or higher and 3.8% of families were below the poverty level, compared to rates of 80.4% and 9.2%, respectively, for the general US population. 29 The cohort was assembled using birth certificate data obtained from the Minnesota Department of Health and using the resources of the Rochester Epidemiology Project (REP). The REP is a medical records-linkage system that includes outpatient and inpatient records from providers in the community and the Mayo Clinic Health System, including Mayo Clinic, Olmsted Medical Center, their affiliated hospitals, as well as smaller care providers. 30 The study protocol was approved by the Institutional Review Boards at both the Mayo Clinic and Olmsted Medical Center.
This study focuses on 7394 individuals who met the inclusion criteria for this study after excluding 17 individuals whose residency could not be confirmed at birth, 136 who had denied access to all of their medical records for research purposes, 3198 without a clinical visit in the REP after 18 years of age, and 193 who lacked 3 or more visits prior to age 5.5 years. Patients with less than 3 visits prior to age 5.5 years were not included in this study due to their exclusion from a partner study using the same study example.
Outcome Variables
Severe obesity and dyslipidemia in adulthood, age 18 years or older, served as the primary outcome variables. Patients in the cohort had their 18th birthday between January 1, 1994 and December 31, 2000. The date of the first documented occurrence of severe obesity prior to October 31, 2020, defined as BMI ≥ 40 kg/m2, was obtained electronically through the REP or identified through manual review of medical records. For instances without simultaneous height and weight measurements, the closest adult height measurement to the corresponding weight measurement was used to calculate BMI. We did not consider weights of pregnant women 6 months before to 3 months after pregnancy. Because height, weight, and BMI were only electronically retrievable starting in 1994 for clinical visits at the Mayo Clinic and starting in 2002 for clinical visits at Olmsted Medical Center, we also used International Classification of Diseases Ninth Revision diagnosis codes for morbid obesity and BMI of 40 or higher to further identify patients with a BMI ≥ 40 kg/m2. A patient was only considered to have severe obesity if there was a documented BMI ≥ 40 kg/m2 irrespective of the diagnosis code.
Dyslipidemia was determined by laboratory values that were obtained electronically up through October 31, 2020. For this study, the date of the first documented occurrence of dyslipidemia was identified based on either a total cholesterol ≥200 mg/dL, non-high density lipoprotein (non-HDL) ≥145 mg/dL or HDL cholesterol <40 mg/dL. 31 Both low density lipoprotein (LDL) cholesterol and triglyceride levels were not used to define dyslipidemia in this study as they are significantly impacted by fasting status which can’t be determined in this retrospective population-based study. 31
Primary Independent Variable
Birthweight and birthweight for gestational age served as the primary risk factors of interest. Both birthweight and gestational age were obtained from the patient’s birth certificate. Birthweight for gestational age during this era was defined as small (SGA), average (AGA), or large (LGA) for gestational age using the 10th and 90th percentiles determined for each gestational age of 30 772 deliveries during 1962 to 1969 in Cleveland, Ohio of single live births. 32
Covariates
The following maternal and birth characteristics were also obtained from the birth certificate data and evaluated: mother’s age and education level, parity, type of delivery, single/multiple gestation, and child’s race and sex at birth. Gestational age was divided into 7 categories based on guidelines by the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists: extremely preterm (<28 weeks), very preterm (28-31 weeks), moderate to very late preterm (32-36 weeks), early term (37-38 weeks), full term (39-40 weeks), late term (41 weeks), and postterm (42-43 weeks).33,34
Socioeconomic status (SES) at birth was quantified using the HOUSES index, a validated index that assesses individual SES from property data using a patient’s address. 35 The HOUSES Index is represented by a single factor made up of 4 items (number of bedrooms, number of bathrooms, square footage of the unit, and estimated value of the unit) ascertained from the county Assessor’s office. Since the original validation of HOUSES index, it has shown to predict a broad range of health outcomes for both adults and children which are known to be inversely associated with SES and compare favorably to other methods of estimating SES.35-47 The HOUSES Index was determined using data from 1985 property data of the Olmsted County (the earliest property data available) by matching with the address where the child lived at birth, but only for houses with a valid street address (eg, PO Box address, incomplete address not matched).
Statistical Analysis
Data was analyzed using SAS version 9.4 statistical software (SAS Institute, NC; Cary, NC) and version 1.4.1103-4 of RStudio. Maternal and birth characteristics were summarized using standard descriptive statistics. Follow-up was calculated starting at each individual’s 18th birthday up until the date of the outcome of interest (ie, first date when BMI ≥ 40 kg/m2 or first date when laboratory values met criteria for dyslipidemia); the follow-up of individuals without the outcomes was censored at the date of their last clinical visit prior to October 31, 2020. Univariate Cox proportional hazards models were fit to evaluate the association of each characteristic with the risk of severe obesity and dyslipidemia, respectively, using age as the time scale. Continuously scaled characteristics were each evaluated in univariate Cox models using penalized smoothing splines to assess the functional form of the relationship with the risk of the outcome. Prior to fitting full multivariable models, missing values for the maternal and birth characteristics were handled using multiple imputation. Ten multiple imputation datasets were created using fully conditional specification methods and the Rubin rules were used to combine the results from the Cox proportional hazards models fit using the multiple imputed datasets. Birthweight and birthweight for gestational age were each evaluated in separate multivariable models given the relationship between birthweight, gestational age, and birthweight for gestational age. Both birthweight and gestational age were included in Model A, but not the categories for birthweight for gestational age. Whereas, the categories for birthweight for gestational age was included in Model B, but not birthweight or gestational age. Associations were summarized using the hazard ratio (HR) and corresponding 95% confidence interval (CI) estimated by the models. All calculated P-values were 2-sided and P-values <.05 were considered statistically significant.
Results
The maternal and birth characteristics of the 7394 individuals included in the analysis cohort are summarized in the first column of Table 1. Overall, 51.9% of patients were male and 98.4% of patients were white. The mean birthweight was 3478.8 (SD, 553.2) grams and 4.2% (308/7378) had a low birthweight (<2500 g). The distribution of birthweight for gestational age was 3.6%, 71.0%, and 22.6% for SGA, AGA, and LGA, respectively, with the remaining 2.8% having incomplete information on either birthweight or gestational age.
Results From the Univariate and Multivariable Analysis of Maternal and Birth Characteristics Associated With Severe Obesity.

Abbreviations: CI, confidence interval; HR, hazard ratio.
Hazard ratio is per a 500-g decrease for birthweight and per a 5-year decrease in maternal age.
Among the 7394 individuals, 798 were identified as having severe obesity and 2357 had dyslipidemia after 18 years of age. Among the remaining 4764 individuals who did not have either outcome, the median age at their last clinical visit was 32.8 (interquartile range, 23.4-38.8) years.
Severe Obesity
In the univariate analysis (Table 1), female sex, singleton birth, younger maternal age (Figure 1B), lower maternal education (Figure 1C), being the first child, and lower SES based on the HOUSES index (Figure 1D) were each significantly associated with an increased risk of severe obesity in adulthood. Neither birthweight (HR per 500 g decrease 1.01, 95% CI 0.95-1.08, Figure 1A) nor birthweight for gestational age (HR for SGA vs AGA 1.04, 95% CI 0.73-1.48) were significantly associated with an increased risk of severe obesity in adulthood. After imputing for missing covariate values, 2 separate full multivariable models were fit. In both multivariable models, female sex, singleton birth, lower maternal education, and lower SES based on the HOUSES index were all independently associated with an increased risk of severe obesity (Table 1, Models A and B). Neither birthweight (in model A) nor birthweight for gestational age (in Model B) were statistically significant in these adjusted analyses.
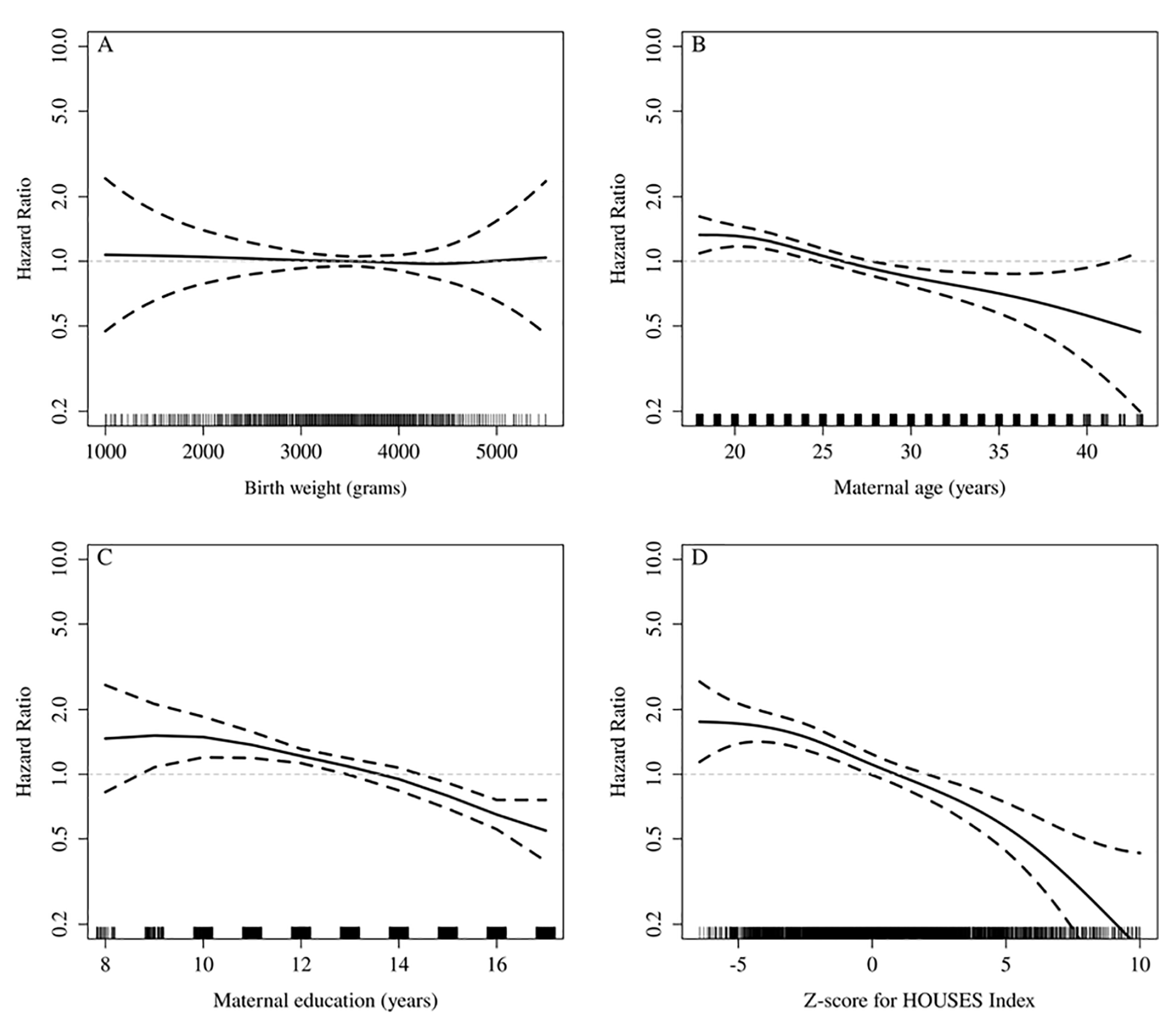
Hazard ratio (HR) for the risk of severe obesity across the range of (A) birthweight, (B) maternal age, (C) maternal education, and (D) z-score for the HOUSES index, respectively. The referent (HR of 1) was pre-defined at the mean of each variable. To address the wide 95% confidence bands (dashed lines) in the tails of each distribution the values in the tails were rounded to the lowest and highest values shown along each x-axis.
Dyslipidemia
As shown in Figure 2, neither maternal age, maternal education, nor the HOUSES index were significantly associated with increased risk of dyslipidemia in adulthood, whereas the hazard ratio for birthweight was 1.19 per 500 g decrease in weight (95% CI 0.99-1.44, Figure 2A). Birthweight for gestational age did not attain statistical significance in the adjusted analysis (Table 2, Model B). Univariately, non-white race and singleton birth were each significantly associated with increased risk of dyslipidemia, with hazard ratios of 1.44 (95% CI 1.05-1.98) and 1.50 (95% CI 1.07-2.12), respectively (Table 2). In multivariable model A, non-white race, singleton birth, and birthweight (HR per 500 g decrease 1.05, 95% CI 1.00-1.09) were all independently associated with an increased risk of dyslipidemia (Table 2, Model A). Given the significant association observed for birthweight, an additional full multivariable model was fit including low birthweight (<2500 g vs ≥2500 g), gestational age, and all of the covariates listed in the table except for birthweight and birthweight for gestational age; the adjusted hazard ratio for low birthweight was 1.34 (95% CI 1.07-1.67; P = .009). Lastly, in a series of 3 separate multivariable models restricted to the 7138 individuals who were white and singleton births, the adjusted hazard ratios in each of the models were 1.05 (95% CI 1.00-1.09, P = .040) for birthweight, 1.08 (95% CI 0.87-1.35, P = .48) for SGA versus AGA, and 1.41 (95% CI 1.13-1.77, P = .003) for low birthweight.
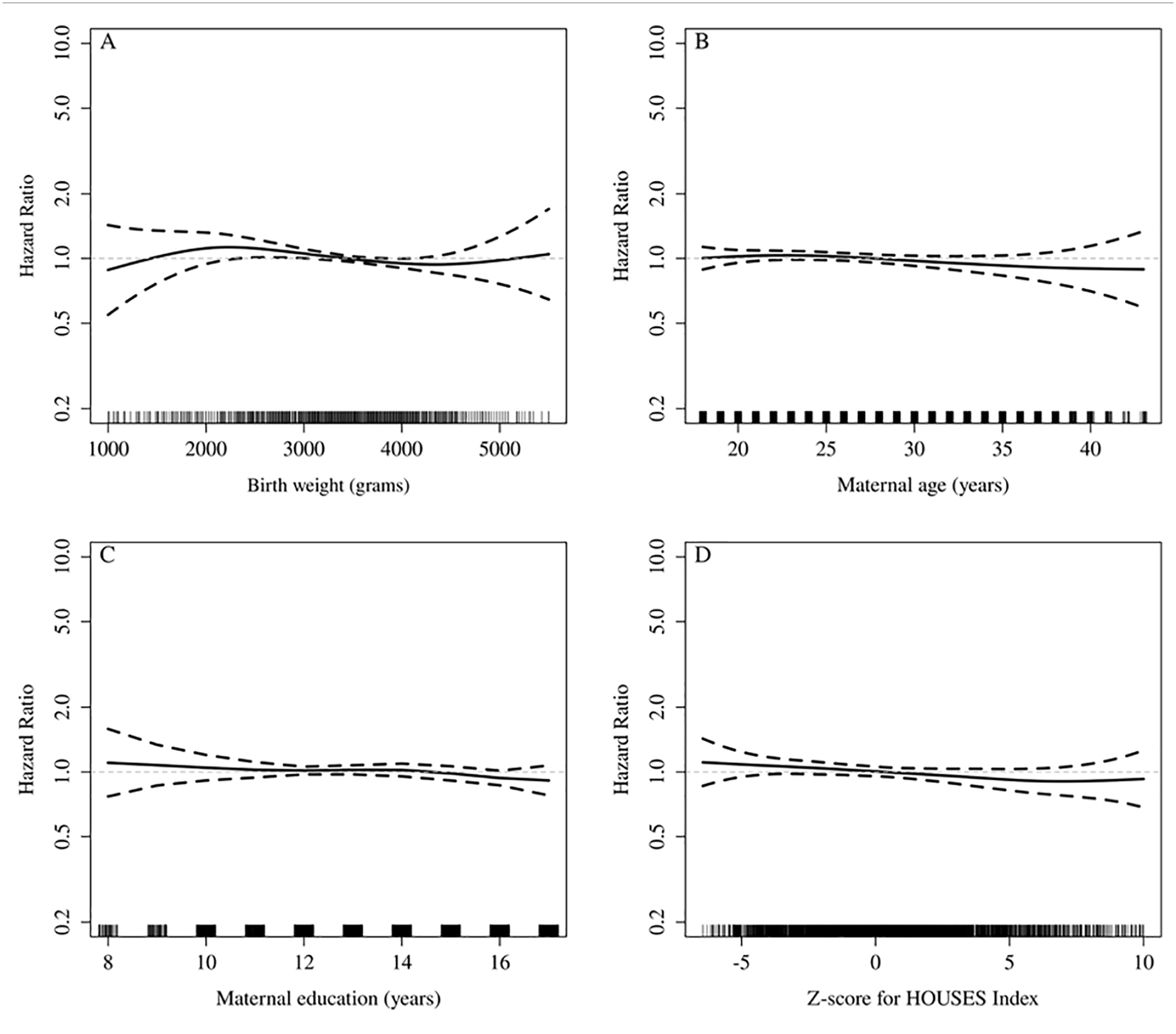
Hazard ratio (HR) for the risk of dyslipidemia across the range of (A) birthweight, (B) maternal age, (C) maternal education, and (D) the z-score for HOUSES index, respectively. The referent (HR of 1) was pre-defined at the mean of each variable. To address the wide 95% confidence bands (dashed lines) in the tails of each distribution the values in the tails were rounded to the lowest and highest values shown along each x-axis.
Results From the Univariate and Multivariable Analysis of Maternal and Birth Characteristics Associated With Dyslipidemia.

Abbreviations: CI, confidence interval; HR, hazard ratio.
Hazard ratio is per a 500-g decrease for birthweight and per a 5-year decrease in maternal age.
Discussion
In this study, female sex, singleton birth, less maternal education, and lower SES were independently associated with an increased risk of severe obesity in adulthood. There was no association between birthweight or birthweight for gestational age and severe obesity in adulthood. There was an association between low birthweight (<2500 g) and dyslipidemia.
The lack of association between birthweight and severe obesity in our study is a departure from findings of previous studies.8,15 The study by Derraik et al 8 found Swedish women born large for gestational age were 50% more likely to develop obesity and severe obesity in adulthood when analyzing 195 936 qualifying women in the national registry. Despite its strengths, this study only involved women and the median age of the adult women was 26, limiting application of these findings to the general adult population. The Rasmussen study involving 18 year old Swedish subjects found that newborns with higher birth weight and length had a higher risk of overweight than those in the control group but this study only included males and evaluated adult patients at age 18. 15 Another study in Sweden by Johnsson et al 13 similarly showed that adults with larger birthweights had increased risk of obesity and type 2 diabetes in adulthood. Additionally, the Nurses Health Study showed a correlation between high birthweight and adulthood overweight among women aged 30 to 55 years old in 1976 and another cohort aged 25 to 42 in 1989. 48 Regarding low birthweight and obesity, multiple international studies display evidence of low birthweight infants being predisposed to obesity in adulthood.16-21 Despite the evidence provided by these studies, most of them took place abroad in a nations with different political, social and environmental factors than the United States, limiting their generalizability to U.S. adult populations.
Several factors could have contributed to the departure of our findings from the literature. Firstly, we hypothesized that investigating severe obesity would provide stronger evidence of the effect of birth weight on metabolic changes. However, it is possible that different factors drive the risk of the development of severe obesity (BMI > 40 kg/m2) as compared to obesity in general. Additionally, it may be that the effects of birthweight are attenuated with advancing age due to a stronger effect of extrinsic factors, as this is an older cohort than other studies. Furthermore, the smaller number of patients with severe obesity in our cohort as compared to previous cohort populations of patients with obesity limited our statistical power in finding associations. Future investigation should focus on the association of both low and high birthweight with obesity in adulthood and analyze severely obese patients as a subset.
The association between low birthweight and dyslipidemia confirms findings of international studies within a Midwestern United States population.24-26 The study by Al Salmi and Hannawi 24 surveyed 4502 individuals in Australia through a nationally representative survey and showed low birthweight individuals to have an increased risk of high total cholesterol overall, increased LDL-cholesterol in low birthweight females, and decreased HDL in low birthweight males. Despite its strengths, the optional nature of this survey study made this study population less representative with regards to age distribution. 27 The Balasuriya study in Norway investigated the association between birthweight and dyslipidemia using a retrospective cohort study in 25 to 28 year old females. 25 Their work showed an association of low birthweight with decreased high-density lipids, increased low density lipids and increased triglycerides. These associations were stronger for the very low birthweight subgroup. Despite the strengths of this study, it primarily involved women ages 25 to 28, limiting its application to the general population. Another study by Gonzalez-Leal in Spain showed similar outcomes in which low birthweight correlated with higher triglyceride levels in obese patients. 26 Although this study evaluated a broader age range of patients, it focused on patients with obesity at a specific hospital, potentially limiting its generalizability. The association between low birthweight and dyslipidemia in adulthood illuminates an opportunity to target adult dyslipidemia by monitoring appropriate in utero growth and encouraging healthy weight gain during pregnancy.
Analysis of our data uncovered secondary associations between severe obesity and lower maternal socioeconomic status as measured by less maternal education and lower HOUSES index. These findings reinforce literature that connects low maternal socioeconomic status with childhood and adult obesity.49-52 Researchers have postulated that this occurs because a patient’s SES in childhood determines their access to quality and nutritious food and health-related activities in addition to influencing their SES in adulthood. Investigation should continue regarding effective ways to mitigate the effects of low maternal SES on later obesity. 50
We also found an association between single gestation births and severe obesity. This is a unique finding and merits further study. Though multi-gestation pregnancies are often compared with IUGR pregnancies, it has been difficult to delineate outcomes due to multiple gestation from confounding factors such as preterm birth that often accompany these pregnancies. 53 Our data which includes only term pregnancies suggests that individuals born as singletons may have greater risk for obesity than individuals born from multi-gestation pregnancies. This is in opposition to the common literature hypotheses that multi-gestation pregnancies have outcomes similar to IUGR pregnancies including increased risk for obesity, dyslipidemia, and comorbid conditions.54-57 Further study is needed to assess the risk of adult metabolic conditions for singleton versus multi-gestation pregnancies.
A major strength of this study is the inclusion of HOUSES index data that allows for the evaluation of the impact of individual-level SES at birth on outcomes in adulthood in a United States population. Another strength of this study is the age of patients from 39 to 45 which is older than the 25 to 28 age range of multiple prior studies and allows for greater generalization to adult populations. Lastly, heights and weights being measured at office visits instead of self-reported, provides better assurance of data objectivity. A limitation of this study was the inability to account for the impact of maternal gestational diabetes and family history of obesity due to limits of the REP. Additional limitations of the study findings are largely due to the timing, location and composition of our study population. Firstly, the study population was born between 1976 and 1982 which was accompanied by a different socio-cultural-political context than the present day. Lastly, the study population is much less ethnically diverse and is on average at a higher SES than the general United States population. Despite these factors, these study findings are important and should be further explored in other U.S. populations.
In conclusion, the results of this study reinforce the impact of maternal SES on adulthood severe obesity and the need for investigation of social supports that may compensate for low maternal SES. This contrasts the influence of low birthweight on dyslipidemia which may suggest a stronger role for epigenetic programming in dyslipidemia than obesity. Lastly, the confirmatory finding that low birthweight is associated with dyslipidemia reinforces that the risk for adult dyslipidemia may be mitigated by factors that promote a normal birthweight.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study used the resources of the Rochester Epidemiology Project (REP) medical records-linkage system, which is supported by the National Institute on Aging (NIA; AG 058738), by the Mayo Clinic Research Committee, and by fees paid annually by REP users. The content of this article is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health (NIH) or the Mayo Clinic. Our project was funded by The Mayo Clinic Children’s Research Center.