
Abstract
An estimated 2 to 3 out of 1000 infants are born with hearing loss in the United States annually.1-4 Newborns with hearing loss who receive appropriate intervention at an early age exhibit better language outcomes than children identified later in childhood who do not receive such services.5-10 Pediatric primary care physicians (PCPs) can help to ensure that infants with hearing loss and their families get the services they need.
Early Hearing Detection and Intervention (EHDI) programs have been established in all US states and most US territories. National goals for EHDI programs are as follows: all newborns will be screened for hearing loss before 1 month of age; all infants who screen positive will have a diagnostic audiologic evaluation before 3 months of age; all infants identified with a hearing loss will receive appropriate early intervention services before 6 months of age. 11
For these overall efforts to succeed, state EHDI programs need accurate and timely information about newborn hearing screening and follow-up. These data form part of an integrated child health information system to monitor the quality of EHDI services and provide recommendations for improving systems of care. 12 In 2009, only 45% of US infants referred for diagnostic evaluation were documented by state EHDI programs as having received follow-up testing. 13 Because pediatric PCPs are often the first professionals who serve a child who is referred for a rescreen or diagnostic evaluation, they can play a pivotal role in decreasing loss to follow-up by referring infants who have risk factors for hearing loss or who have confirmed hearing loss to the appropriate services. Reporting this information to their state EHDI program forms an important part of this role.
The 2007 Joint Committee on Infant Hearing (JCIH) position statement provides comprehensive information about risk factors, associated conditions, and guidelines for medical home professionals for referring infants under their care with suspected or confirmed hearing loss. An algorithm to guide pediatric PCPs regarding the delivery of care to children with, or at risk for, hearing loss can be found at http://www.medicalhomeinfo.org/downloads/pdfs/Algorithm1_2010.pdf. 12 Information about state EHDI programs, including contact information, can be found at http://www.cdc.gov/ncbddd/hearingloss/ehdi-programs.html. In the present article, we examined patient, physician, and practice variables associated with pediatric PCP–reported adherence to 2007 JCIH recommendations. 12
Methods
We licensed data from the 2008 annual DocStyles survey to examine EHDI practices among pediatricians and family/general physicians. In 2008, Porter Novelli * conducted DocStyles, an annual web-based survey of health practitioners. Quotas included 1000 family/general physicians and 250 for each additional specialty sample (pediatricians, ob/gyns, dermatologists, and registered dietitians). Participants were paid $50–$75 for completing the survey.
The physician sample was drawn from Epocrates Honors Panel, 14 an opt-in panel of 135 000 physicians. Epocrates randomly invited a sample of eligible physicians listed in its main database to participate in the survey. The sample reflected American Medical Association proportions for age, sex, and region. Physicians were included if they practiced in the United States, actively saw patients, worked in a practice (individual, group, or hospital), and had been practicing medicine for at least 3 years. Invited physicians were not required to participate and could exit the survey at any time.
Response Rate
To reach quotas, 14 346 physicians from the Epocrates Honors Panel were invited to participate in DocStyles 2008 via e-mail. Of this sample, 1880 completed the survey; 33 did not complete the survey; 141 sessions were terminated on the basis of screening questions; 1088 physicians logged in, but the survey was not administered because of filled specialty quotas; and 11 204 did not respond to the invitation, or they tried to respond after the survey closed. The overall response rate was 22%. †
Inclusion/Exclusion Criteria
Pediatricians and family/general physicians were stratified in the analyses because their respective academic guilds have different histories of endorsing newborn hearing screening (American Academy of Pediatrics 15 in 1999, American Academy of Family Physicians 16 in 2008). The statement by the American Academy of Family Physicians followed a revised statement by the US Preventive Services Task Force. 17 This difference might influence whether each type of pediatric PCP follows the JCIH 2007 guidelines. 12
The DocStyles quotas for family/general physicians and pediatricians was 1000 and 250, respectively. In sum, 510 family/general physicians and 250 pediatricians were eligible for this study. Of the 510 potentially eligible family/ general physicians, 23 were excluded because they had no data indicating the number of pediatric patients they saw. One was excluded because she or he reported seeing no pediatric patients. This resulted in 486 completed surveys from family/general physicians and 250 from pediatricians.
Instrument
The DocStyles survey was developed with guidance from federal public health agencies and other nonprofit and for-profit clients. The 2008 DocStyles survey contained 140 questions about physicians’ attitudes and counseling behaviors regarding a variety of health issues; 8 questions related to pediatric PCPs and EHDI were included.
Statistical Analyses
Descriptive statistics and multivariate logistic models were calculated with SPSS 17. 18 To ensure adequate power and to allow for logistic regression modeling, responses of “sometimes” and “yes” were combined to form yes/no dichotomous indicators. Independent variables were age, work setting, years of experience, number of pediatric patients seen during a week, financial status of patients, and race/ethnicity of patients, which were collectively included in each of 8 models predicting the dichotomous indicators of physician responses for the EHDI survey questions. Statistical significance was accepted at P < .05.
Due to expectedly large differences in pediatric patient load, the average number of pediatric patients seen per week was divided into quartiles, stratified by type of pediatric PCP (Table 1).
Pediatricians and Family/General Physicians: Patients per Week (in Quartiles)

Results
Demographic characteristics of the 2 types of pediatric PCPs and their patients are shown in Table 2. Tables 3, 4, and 5 show that pediatricians who worked in a hospital or clinic were more likely to receive hearing screening results than were pediatricians who worked in individual or group practices (adjusted odds ratio [OR] = 5.87; 95% confidence interval [CI]: 2.72, 12.65). Family/general physicians with heavier caseloads were more likely to receive hearing screening results for their pediatric patients (adjusted OR = 1.02; 95% CI: 1.01, 1.03). Pediatricians who worked in hospital and clinic settings were more likely to check for hearing screening results than were those who worked in individual or group practices (adjusted OR = 0.16; 95% CI: 0.05, 0.53). Family/general physicians with heavier case loads were less likely to check for hearing screening results for their pediatric patients than were those with lighter caseloads (adjusted OR = 0.97; 95% CI: 0.95, 0.99). Younger family/general physicians were more likely to counsel parents to have their infant’s hearing screened than were older family/general physicians (adjusted OR = 1.00; 95% CI: 0.95-1.00).
Pediatricians and Family/General Physicians: Demographic and Practice Characteristics a
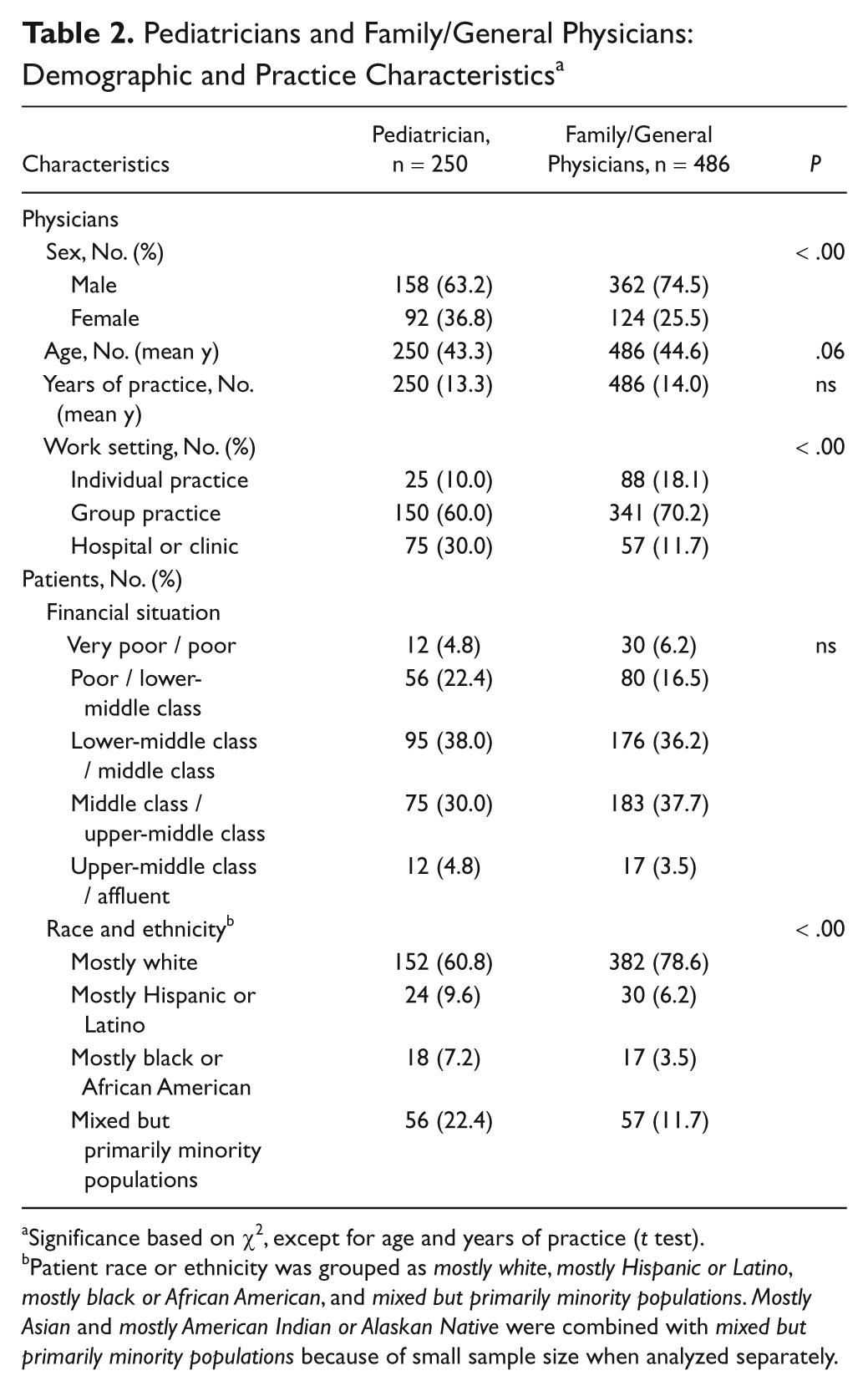
Significance based on χ2, except for age and years of practice (t test).
Patient race or ethnicity was grouped as mostly white, mostly Hispanic or Latino, mostly black or African American, and mixed but primarily minority populations. Mostly Asian and mostly American Indian or Alaskan Native were combined with mixed but primarily minority populations because of small sample size when analyzed separately.
Multivariate Logistic Regression Models Predicting a Positive Response: “Does Your Office . . . ?” a

“Does your office receive hearing screening results for newborns and young children under your care?” CI, confidence interval.
Family/general physicians who see more pediatric patients per week were more likely to receive hearing screening results.
Pediatricians who work in a hospital setting or clinic more likely to receive screening results.
Pruned Multivariate Logistic Regression Models Predicting a Positive Response: “If Your Office . . . ?” a

“If your office does not always receive the newborn hearing screening results for an infant under your care, do you or someone else in your office check with the birth hospital or state [Early Hearing Detection and Intervention] program for the results?” CI, confidence interval.
Negative coefficient, indicating that family/general physicians who see more pediatric patients per week were less likely to check for hearing results.
Pediatricians who work in a hospital setting more likely to check for screening results.
Pruned Multivariate Logistic Regression Models Predicting a Positive Response: “If You Know . . . ?” a

“If you know an infant under your care has not had his/her hearing screened, do you counsel the parents to have the infant’s hearing screened?” CI, confidence interval.
Younger family/general physicians more likely to counsel.
Tables 6-9 summarize the percentages of physicians who selected each response, the χ2 values, and P values regarding reasons for checking or not checking for hearing screening results and for taking or not taking actions if an infant or young child under their care failed the newborn hearing screening, was identified with hearing loss, or had risk factors for hearing loss.
Responses to Questions About Knowledge and Practices of Early Hearing Detection and Intervention: “Why Does Your Practice . . . ?” a

“Why does your practice not check or only sometimes check for the hearing screening results? Please select all that apply.”
Responses to Questions About Knowledge and Practices of Early Hearing Detection and Intervention: “What do you do . . . ?” a

“What do you do if you know an infant fails the newborn hearing screening? Please select all that apply.”
Responses to Questions About Knowledge and Practices of Early Hearing Detection and Intervention: “If an Infant or Young Child Under Your Care Is Identified . . . ?” a
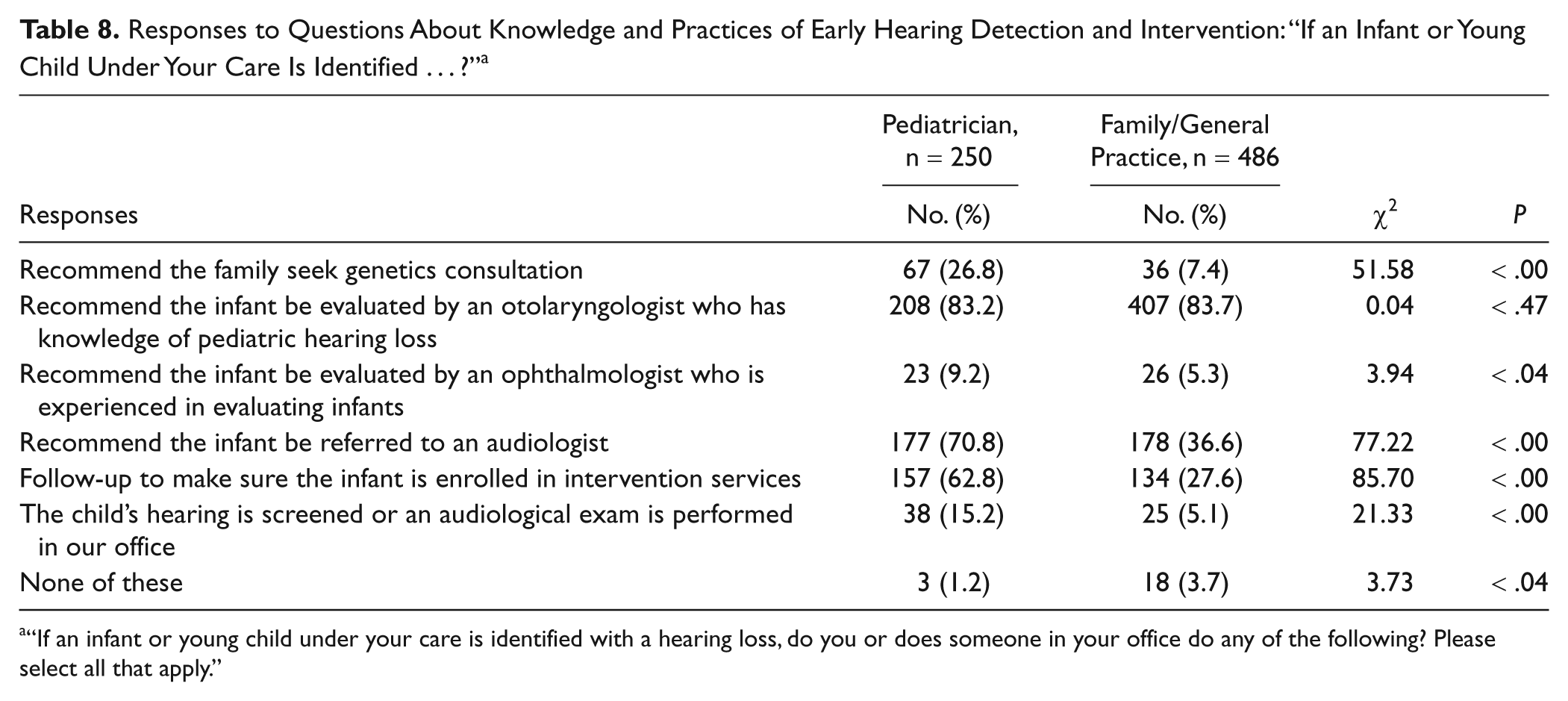
“If an infant or young child under your care is identified with a hearing loss, do you or does someone in your office do any of the following? Please select all that apply.”
Responses to Questions About Knowledge and Practices of Early Hearing Detection and Intervention: “If an Infant or Young Child Under Your Care Has Risk Factors . . . ?” a
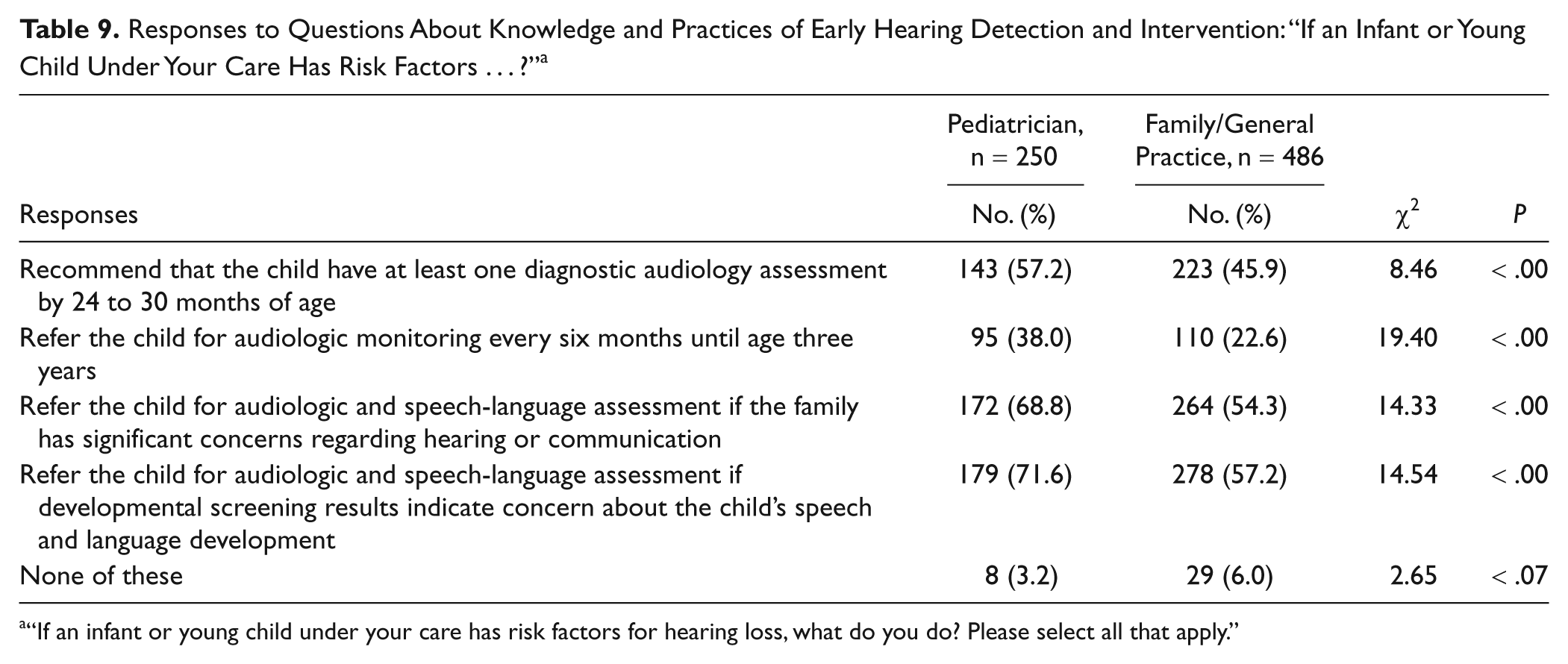
“If an infant or young child under your care has risk factors for hearing loss, what do you do? Please select all that apply.”
Table 6 indicates that similar proportions of pediatric PCP practices have no mechanism to obtain results or find it difficult to get the screening results and have charting procedures that do not include hearing screening results. Few physicians reported insufficient time or the belief that it was the parents’ responsibility. Pediatricians were more likely than family/general physicians to respond that the hospital keeps track of screening results and that the parents report the results to their office.
Table 7 shows low proportions of physicians reporting they contact the state EHDI program if they know that an infant under their care failed the newborn hearing screening. Pediatricians were more likely than family/general physicians to respond that they refer the infant for a rescreening or audiology appointment (and let the parents make the appointment). Family/general physicians were more likely than pediatricians to respond that they would have someone in their office make the rescreening or audiology appointment for the parents. Pediatricians were more likely than family/general physicians to respond that they follow up with parents to be sure that the rescreening or audiology exam is done and that they follow up with the rescreening facility or audiologist for results, although the proportion who follow up was low for both types of pediatric PCPs.
Table 8 shows high proportions of physicians responding that they recommend an infant with hearing loss under their care be evaluated by an otolaryngologist. Pediatricians were more likely than family/general physicians to respond that they recommend the infant be referred to an audiologist and that they follow up to ensure that the infant is enrolled in intervention services. Few pediatricians and family/general physicians reported recommending that an infant with hearing loss be evaluated by an ophthalmologist.
Table 9 shows that, overall, pediatricians were more likely than family/general physicians to follow JCIH 2007 recommendations if an infant or young child under their care had risk factors for hearing loss. However, only about half of both types of physicians responded that they recommended a child with risk factors have at least 1 diagnostic audiology assessment by 24–30 months of age. Sixty to seventy percent of family/general physicians and pediatricians responded that they referred an infant or child with risk factors for audiologic and speech-language assessment if the family had significant concerns regarding hearing or communication or if the infant’s or child’s developmental screening results indicated concern about his or her speech and language development.
Discussion
The results from this study indicate an association between adherence to the EHDI process and factors of care setting, physician type, and caseload. Offices in hospital settings and clinics might be more likely to have mechanisms for requesting newborn hearing screening results, such as access to electronic data tracking and surveillance systems and established standardized reporting protocols. 19 Family/general physicians with large caseloads of pediatric patients could be more likely to have standardized protocols for receiving infant hearing screening results, access to electronic EHDI data-tracking systems, and a standing order for hospitals to communicate any newborn screening results of their patients to their office. 19 This kind of support for family/general physicians with lighter pediatric caseloads could help improve follow-up.
It is important for physicians to inform their state EHDIprogram that an infant under their care failed a newborn hearing screening, because many children are lost to follow-up. 20 In addition, the results of newborn hearing screening are not always sent to the correct pediatric PCP. Pediatric PCPs can help bridge this gap by letting their state EHDI program know that an infant who failed a newborn hearing screen is under their care; however, few survey respondents reported doing so. Better infrastructure, such as efficient and accurate communication among those engaged in the EHDI process (eg, hospital staff, pediatric PCP offices, and EHDI programs), use of electronic surveillance and tracking systems, and standardized protocols for communicating results between pediatric PCPs and EHDI programs could help improve child outcomes. 19
That few respondents reported recommending referral to an ophthalmologist is an important gap in care. Many children with hearing loss are at higher risk for vision problems,21,22 which plays an important role in communication for children with hearing loss, regardless of mode of communication. Emphasizing this recommendation to physicians could benefit the communication outcomes of children with hearing loss. A recent survey showed that high proportions of otolaryngologists refer infants and children under their care to ophthalmologists (31%-66%). 23 Communication between PCPs on one hand and otolaryngologists and state EHDI programs on the other could help bridge this information gap and improve loss-to-follow-up rates and adherence to JCIH 2007 recommendations.
Only about half of physicians reported recommending at least one diagnostic audiology assessment by 24-30 months of age for children with risk factors for hearing loss (JCIH 2007 recommendation).
An important limitation of this study was the low response rate, which increases the possibility of nonresponse bias. The advent of web-based survey technologies has made contacting physicians less resource intensive. However, the yield of web-based surveys has been low: a meta-analysis of 68 web-based surveys revealed an average response rate of 39.6%, with a large range (±19.6%). 24 Therefore, the survey response rate in this study is comparable to previous web-based surveys of physicians.23,25,26 Future research should explore the effects of reimbursement on adherence to the 2007 JCIH recommendations.
Conclusions
Follow-up testing and early intervention are important for infants identified with, or who have risk factors for, hearing loss. This study highlights the need to increase the rate at which pediatric PCPs receive and request infant hearing screening results, and it suggests that improved infrastructure could facilitate pediatric PCPs’ ability to report and coordinate follow-up services for infants identified with hearing loss. 19 An algorithm to guide pediatric PCPs regarding the delivery of care to children with or at risk for hearing loss can be found at http://www.medicalhomeinfo.org/downloads/pdfs/Algorithm1_2010.pdf. 12 Information about state EHDI programs, including contact information, can be found at http://www.cdc.gov/ncbddd/hearingloss/ehdi-programs.html. Furthermore, communication among specialists to whom infants are referred and pediatric PCPs could help improve loss-to-follow-up rates and documented adherence to JCIH 2007 recommendations.
Footnotes
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
*
†
The following formula was used to calculate response rates based on the percentage of qualified or eligible respondents completing the survey: response rate = completed surveys / {completed surveys + [completed surveys / (completed surveys + terminated–did not meet screening criteria + terminated due to filled quota for specialty)] × (no response or responded after survey closed + incomplete surveys)}; or, 1880 / {1880 + [1880 / (1880 + 141 + 1088)] × (11 204 + 33)} = 22%. This formula is useful for accurately reflecting Internet research response rates; it weights respondents who are terminated because of filled quotas as a factor of the overall sample pool, as opposed to merely classifying them as standard incompletes. This equation can be found at the following websites: http://www.answersresearch.com/response.php and ![]() .
.