
Abstract
Introduction:
Children in foster care are at higher risk of health problems. These risks present challenges to achieving permanency, safety, and well-being. Despite efforts to improve the systems serving children in foster care, gaps remain in achieving timely and quality health services. Based on stakeholder reports that health care provider knowledge about child welfare systems is a barrier to care, the Fostering Health Partnerships project conducted 2-session learning collaborative events across Michigan. The project team hypothesized that participants would increase knowledge of child welfare policy and that physician participants would identify and commit to practice change to improve health care services to children in foster care.
Methods:
Learning collaborative events included an in-person session followed by a live webinar session. Participants included child welfare professionals, physicians, and other health care representatives. Participants completed surveys assessing knowledge about child welfare health policy. Physician participants completed a post-event interview. The investigators used pre- and post-intervention survey design and qualitative evaluation of physician interview data to assess the impact of the learning collaborative events on knowledge and practice.
Results:
A total of 781 individuals attended the initial session and 383 attended the second session of 36 events for 80 counties in Michigan. 247 individuals completed pre- and post-event surveys and 7 physicians completed interviews after the events. Survey data showed that event participants demonstrated increased knowledge of child welfare policy related to health (P < .001). Interviewed physicians reported making practice changes to improve health care services and indicated that the events were valuable though time intensive.
Conclusion:
An abbreviated learning collaborative process is an effective tool to improve knowledge and drive practice change. Future efforts will build on this project to improve access, coordination, and quality health services for children in foster care.
Keywords
Introduction
Children in foster care experience high rates of health, dental, and behavioral health issues1-4 related to a number of factors including family/genetic risk and sociodemographic characteristics, 5 prenatal exposures,6,7 and trauma exposure. 8 Unmet health and mental health needs reduce well-being, safety and permanency, 9 the core goals of the child welfare system. As a result, child welfare systems at local, regional, state and national levels work with health providers, and systems to improve access to and quality of care.
Despite such efforts, evidence shows persisting gaps in achieving health care benchmarks for children in foster care.10-12 National trends are reflected in some of the challenges faced by states, including ensuring seamless insurance coverage during the transition into foster care, maximizing the access pathways to health care providers, supporting foster caregivers in making and keeping appointments and ensuring effective health information transfer.2,10 The Michigan Department of Health and Human Services (MDHHS) engages its internal departments and divisions and external community partners to address these barriers to timely, comprehensive, and quality health care for children.
Noting ongoing challenges in ensuring that children entering foster care participate in an initial comprehensive health examination after foster care placement, MDHHS convened partners and stakeholders across systems to identify and address barriers in achieving benchmark standards for initial health examinations. Among the barriers identified was engaging primary care providers in understanding child welfare policies that support meeting the health needs of children at foster care entry.
As a response to this and other stakeholder information related to the challenges of meeting the health care needs of children in foster care, the department developed the Fostering Health Partnerships project. The aims of Fostering Health Partnerships were to (1) improve the understanding of all stakeholders about child welfare policy related to health and well-being, (2) to identify the gaps faced at the local and regional level to meeting the health and well-being needs of children in foster care, and (3) to engage in strategic planning to close gaps in care including creating practice change across systems. These aims were supported by the following objectives: (1) to hold learning collaborative events (LCEs) throughout Michigan in single-county or regional county-clusters that included key stakeholders, (2) to facilitate a discussion among partners about systems gaps and potential solutions, (3) to gather data about participants’ knowledge and practice pre- and post-LCEs, and (4) to gather more detailed information from physicians about the impact of the LCE participation on their understanding and practice.
Stakeholders included child welfare teams and representatives from throughout the health care and social services community including primary care, dental and mental health care providers; health plan representatives; Early On (the system in Michigan that helps infants and toddlers who have or are at risk for developmental delays and their families find social, health and educational services to promote development), local health departments and school systems. The project adapted the principles of learning collaboratives, which have been used to accomplish goals within health care systems by engaging stakeholders in strategic planning to address clinical issues.13,14 The combination of flexibility and capacity to structure discussions allowed by the learning collaborative process seemed well-suited to the goals of this project. In examining child welfare health systems, Jee et al 10 used a learning collaborative process involving health care providers to examine best practices and the impact of different care models in adhering to clinical guidelines. They discovered variation within and between the care models and noted that the participants benefitted from describing their unique experiences.
The project built on the lessons of earlier work in three Michigan counties. That effort consisted of a series of three stakeholder meetings held in each county. These events were well-received by attendees but required a substantial time commitment by both planning team and participants, limiting the reach of the project both in terms of geography and in the number and types of participants able to commit to the three-part series. To reach child welfare and health care provider teams across the state within a shorter time frame, the project team adapted the typical learning collaborative process from multiple meetings over several weeks to a format consisting of two meetings. This format required less time commitment for attendees while still providing both education and a platform for local cross sector providers to meet and engage in planning and systems change.
This manuscript reports data to test the following hypotheses: (1) participants would demonstrate an improved knowledge of child welfare policy, and (2) physician participants, as a primary stakeholder group, would identify and commit to making changes in their practice to improve their capacity to meet the health care needs of children in foster care.
Methods
Study Population and Design
The present report utilizes both pre- and post-intervention design and qualitative evaluation of physician interview data to assess the impact of LCEs on the practices of professionals from organizations providing services for children in foster care in the state of Michigan.
Health care professionals and child welfare personnel were the main target audience of the intervention. Health care professionals included primary, dental, and mental health providers as well as office staff. Child welfare personnel included foster care and protective services caseworkers, supervisors, managers, and health liaison officers, specialists who assist direct care workers in activities related to health services. Other invited professionals included employees of intermediate school districts, local health department staff, Medicaid Health Plan (MHP) case managers, and representatives from courts, including court administrators. Only data from participants who provided written informed consent are included in this report.
Intervention
The intervention examined was the LCE conducted as two meetings, the first in person, and the second as a live webinar. Each in-person meeting started with brief presentations on child welfare policy and practice related to meeting health needs of children, for example the requirement to complete a comprehensive health examination within 30 days of foster care entry, and Medicaid policy related to children in foster care, including provisions to reimburse for these examinations. Then the facilitators led a discussion based on a theoretical case about a child in foster care. The case highlighted common challenges faced by child welfare teams and health care providers when providing health services for children in foster care. From this discussion, the participants identified gaps in the systems of care that they had experienced, shared information about existing local and regional resources, prioritized needs, and developed action steps to meet the needs. The follow-up meeting focused on reporting progress achieved on the action steps from the in-person meeting and discussing ongoing actions to maintain system change.
Data Acquisition
Attendance and action plans were documented in a project database. Participants were invited to take pre- and post-LCE surveys, either in person or online. Both surveys included questions to assess mastery of topics relevant to providing health care services for children in foster care. The post-LCE survey included a closed-ended yes/no question about the participants’ intention to implement ideas as a result of participating in LCEs. In addition, the post-LCE survey included open-ended questions asking respondents to identify any practice changes or concrete actions they were planning to implement to improve health care services for children in foster care. Answers to these questions were processed and analyzed to derive the most common action commitments. The most reported commitments for practice changes among physicians provided the topics for subsequently conducted follow-up physician interviews to determine the extent to which commitments for practice changes were implemented. Survey and interview data were de-identified prior to analysis.
Data Analysis
To measure levels of knowledge in areas relevant to the health care of children in foster care, we examined survey responses to 15 questions on a scale from 1 to 5, ranging from “No Understanding” to “Very Good Understanding.” For the purpose of statistical analysis, we then constructed a composite score by averaging across all knowledge items. To evaluate the effectiveness of LCEs on knowledge gains, we conducted a paired samples t-test comparing the average self-reported pre- and post-intervention knowledge scores.
Answers to open-ended survey questions regarding practice changes or concrete actions were submitted to content analysis to derive common action commitments. Analysis of data collected via the follow-up physician interviews was focused on answers to a series of closed-ended yes/no questions about the physicians’ actual implementation of a specific set of practice changes derived from content analysis of answers to relevant survey questions.
This study protocol, including the pre- and post-event surveys and physician interviews and the written informed consent provided by participants, was reviewed and approved by the Michigan Department of Health and Human Services Institutional Review Board for the Protection of Human Research Subjects (201805-04-XA).
Results
Participant Characteristics
A total of 781 participants attended one of 36 in-person meetings and 383 attended follow-up webinar meetings for 36 total LCE events held between February 26, 2018, and January 6, 2020. Analysis of in-person attendance records reveal the number of participants ranged from 11 to 41, generally reflecting the range of the population density across the state, including urban, suburban and rural regions. All in person events included representation from child welfare, 32 of 36 in person events included primary care participants, with the following represented as well (in order of decreasing frequency): behavioral health, education, community-based organizations, health plans, dental providers, public health, courts, parents, and native American tribal members.
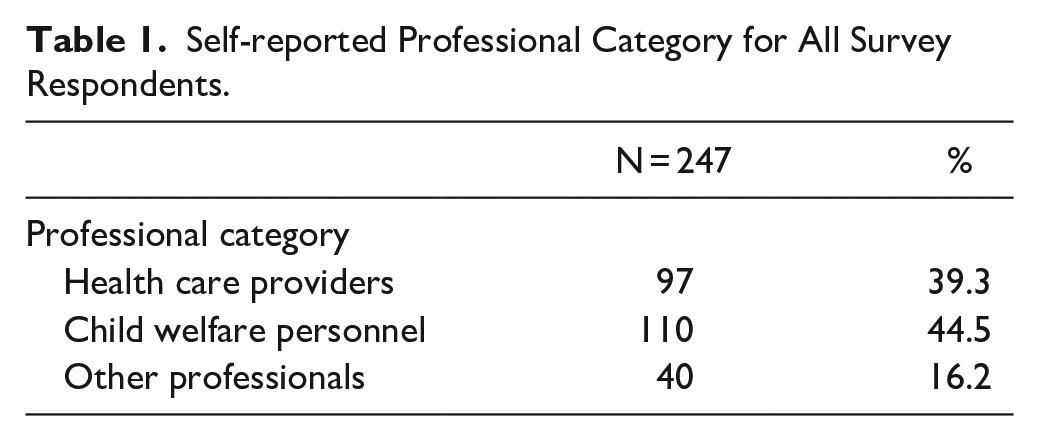
A total of 247 LCE participants completed both pre and post surveys (31% of the participants during day one, and 64% of participants who attended both days). Table 1 presents the professional category reported by survey respondents and the roles reported by health care participants. The two largest professional categories consisted of health care (39.3%) and child welfare (44.5%) personnel. Other professional categories had sizable representation (16.2%), and consisted primarily of employees of intermediate school districts, Medicaid Health Plan case managers and court representatives.
Self-reported Professional Category for All Survey Respondents.
The survey also asked health care providers to indicate whether they were providing care for children in foster care. Of the 97 health care professionals who attended the LCEs, 82 (85%) reported providing services to children in foster care. Over half of these (53.6%) had more than 10 years’ experience providing health care to children in foster care and nearly half (43.9%) were providing services to 6 or more children each month. However, less than half (45.8%) of these 82 respondents reported having a special process in place to identify children in foster care.
Participant feedback
Responses to questions in the post-LCE survey showed that 41% of all participants were familiar with less than half of the material that had been presented during the LCE. However, 60% of the participants from health care and other systems, compared with 15.5% of child welfare personnel, indicated that they were familiar with less than half of the presented material.
Over 90% of participants found the LCE beneficial. Specifically, participants reported understanding child welfare policy better (n = 204), integrating new information (n = 163) and stimulating interest to learn more about systems serving children in foster care (n = 174).
Primary outcomes
Knowledge gains
As expected, participants in the learning collaborative events increased their knowledge of child welfare policy related to health and well-being. The post-LCE (M = 4.15, SD = 0.64) scores were significantly higher than the pre-LCE (M = 3.22, SD = 1.07) scores (t(246) = 17.78, P < .001).
Supplemental Tables 1 to 4 show the pre- and post-intervention results for each of the 15 topics. Each table lists the items in decreasing order of post- to pre- survey change. Supplemental Table 1 shows the results for all participants and Supplemental Tables 2 to 4 show the results for each participant category. The items with greater knowledge are different according to the participant category.
Intention to change
The post-LCE survey also asked participants if they intended to implement any ideas or do anything else differently as a result of participating in LCEs. Table 2 presents the percentage of health care providers, child welfare personnel, and other professionals who reported an intention to act following their participation. Overall, 82.2% of participants expressed the intention to make changes because of their participation in LCEs. Results were similarly high across all groups, including health care providers (83.5%), child welfare personnel (80.9%), and other professionals (82.5%). In addition, respondents answered open-ended questions in the post-LCE survey asking them to identify what concrete actions they were planning to implement to improve health care services for children in foster care. Child welfare personnel most frequently reported intention to develop more detailed office protocols that would improve distributing child welfare documents to health care providers and to develop stronger communication with health offices that would improve information transfer to providers new to children (n = 32). The most frequently intended practice changes reported by physicians included plans to implement new, or improve existing, processes in their offices to facilitate the identification of foster care cases and increase parental engagement (n = 46). Concrete steps in this regard included: (1) identifying children who were in foster care, (2) engaging birth/legal parents, and (3) coordinating with foster care workers. Additional intended actions included: (4) meeting the initial exam requirements, (5) obtaining proper consent for psychotropic medication per child welfare policy, (6) complying with reporting requirements, (7) receiving medical history, and (8) sharing and receiving care plans.
Intention to Change.

The key informant interviews with 7 physicians representing 5 distinct regions of the state occurred approximately 8 months (range 3-11 months) after LCE participation. Physicians were specifically asked to indicate the extent to which attending the LCE had an impact in their practice related to the implementation of changes in each of the 8 areas identified through the qualitative analysis of Post-LCE responses. Results presented in Table 3 indicate successful implementation in most areas, including the identification of foster case cases, meeting the initial exam requirement, complying with reporting requirements, obtaining proper consent, and the engagement of birth/legal parents. However, results also suggest that improvement is needed in receiving medical history and sharing and receiving care plans. Six of the 7 physicians interviewed also reported that they had shared, or planned to share, the materials from the learning collaborative events with colleagues in their offices.
Progress Made in Implanting Practice Changes.

Interviewed physicians were also asked to assess the cumulative impact of practice changes in the 8 areas identified above. Physicians reported that the primary cumulative benefits were improved communication, greater participation in decision making, and more comprehensive and timely care of children in foster care.
Discussion
The participant survey and physician interview data from Fostering Health Partnerships support both of the project’s hypotheses that bringing together partners across the systems supporting children in foster care would improve the knowledge and understanding of each partner about the health needs of these children and begin the process of changing practice to address identified system gaps with the goal of improving care. It is notable that the increase in understanding was substantial in those coming from health and mental health systems, but not surprising, as physicians and other members of health care teams’ understanding of child welfare systems pre-event was lower than that of child welfare professionals who engage in child welfare practice daily. Survey responses from all participants post-LC events indicated that each stakeholder group used the event to develop practice changes that would improve access to care and increase coordination and collaboration. The physician interview data indicated that physicians passed the knowledge they gained from the events to colleagues, thus expanding the reach of practice change beyond those who attended the events. These results are consistent with the findings by Terrell et al 12 which showed that a learning collaborative involving child welfare personnel and a single pediatric practice helped to identify communication gaps and improve the time to initial examination for children new to foster care.
The results from this project highlight the capacity for even a brief (2 session) learning collaborative process to improve knowledge about the health care needs of children in foster care, understanding of the challenges developing a coordinated system to serve these children and to begin the process of practice change. The events also offered the opportunity to build upon existing local and regional relationships, thus expanding their impact. The project was not designed to measure how this learning collaborative event process translates into long term system change. However, increasing the participant prioritization of a change, and motivation for change generally, has been found to be an important initial component of building readiness for community change. 15 The survey and interview data from this project show that the learning collaborative events achieved these change prerequisites.
This project and therefore the data collected have some limitations. First, the attendees at each event included a subset of those in each community. The project framework provided no mechanism to predict the impact of the LCE on the broader health care provider community in any region. The physician interview data also indicated that although the attendees found the events valuable, the learning collaborative event process required a time commitment that most health care providers cannot make. As most physician attendees shared the information from the LCE with office colleagues, developing less time-intensive ways to inform and engage health care should be effective in expanding awareness and creating practice change. Finally, learning collaborative processes typically occur over a longer period; for example, 12 to 18 months (reviewed by Wells 14 ) and their intended outcome is often sustained change in a specific clinical practice. 13 The model followed in this project was intentionally that of short-term interactions over 2 sessions because of the intent to reach system partners across the state.
The project team took some steps to address these project limitations. First, the in-person meeting agenda focused on establishing relationships between parties, providing information that would set the stage for ongoing collaboration and asking attendees to identify a few key priorities in their region to work on and report back at the second meeting of the LCE. Second, the project team used the group discussion from the events to develop enduring materials to support ongoing collaboration and partnership. These materials include both information generally applicable across the state and unique to each county and region. These materials are available on Michigan’s Department of Health and Human Services public website https://www.michigan.gov/mdhhs/0,5885,7-339-73971_7117_77104_91971—,00.html to support ongoing collaboration. Third, the project leadership offered meeting times at the end of the project for partners to hear about the project outcomes and to discuss ongoing challenges and efforts to improving collaboration and coordination. A few counties took advantage of this opportunity.
In conclusion, the abbreviated learning collaborative process used during this project was an effective tool to expand knowledge about the health needs of children in foster care across the systems serving them and engage health care providers in initiating practice changes to meet these needs. Future efforts will include developing effective ways to bring information about the health needs of children served by child welfare systems to health care providers in each region to continue the work of improving access, coordination, and quality of care.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211048359 – Supplemental material for Learning Collaborative Events With Child Welfare and Health Care Providers Improve Systems Knowledge and Intent to Change
Supplemental material, sj-docx-1-jpc-10.1177_21501327211048359 for Learning Collaborative Events With Child Welfare and Health Care Providers Improve Systems Knowledge and Intent to Change by Jeanette M. Scheid, Issidoros Sarinopoulos, Sierra Cameron and Clare Tanner in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michigan Health Endowment Fund
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.