
Abstract
Introduction:
Understanding barriers in primary health care access faced by Canadian immigrants, especially among women, is important for developing mitigation strategies. The aim of this study was to gain an in-depth understanding of perceived challenges and unmet primary health care access needs of Bangladeshi immigrant women in Canada.
Methods:
In this qualitative study, we conducted 7 focus groups among a sample of 42 first-generation immigrant women on their experiences in primary health care access in their preferred language, Bangla. Descriptive analysis was used for their socio-demographic characteristics and inductive thematic analysis was applied to the qualitative data.
Results:
The hurdles reported included long wait time at emergency service points, frustration from slow treatment process, economic losses resulting from absence at work, communication gap between physicians and immigrant patients, and transportation problem to go to the health care centers. No access to medical records for walk-in doctors, lack of urgent care, and lack of knowledge about Canadian health care systems are a few of other barriers emerged from the focus group discussions.
Conclusions:
The community perception about lack of primary health care resources is quite prevalent and is considered as one of the most important barriers by the grassroots community members.
Introduction
In Canada, primary health care (PHC) serves as the first point of contact to access health services. 1 PHC services often include family physicians, prevention, and treatment of common diseases and injuries, basic emergency services, referrals to/coordination with other levels of care (such as hospitals and specialist care), primary mental health care, palliative and end-of-life care, health promotion, healthy child development, primary maternity care and rehabilitation services. 2 Difficulty accessing PHC may contribute to delay in seeking and obtaining treatment; under using preventive health care or services, which could lead to a delayed diagnosis; increased risk of complications; more complicated treatment for sicker patients; and longer hospital stays. These potential consequences, in turn, may increase the financial burden on the health care system and decrease compliance with treatment. 3 Thus, easy and timely access to PHC services is of immense importance for the overall health of Canadians. 4
A significant proportion of the Canadian population are immigrants (21.9%). 5 Increasingly so, the health of Canadian immigrants is an important determinant of population health and is directly related to issues of cost and adequacy of the Canadian health care system. 6 New immigrants were reported to be almost two and a half times more likely to perceive difficulties accessing immediate care compared to their Canadian-born counterparts. 3 Health conditions for immigrants worsen over time, with the decline becoming steeper when more than 10 years are spent in Canada.7,8 Remarkably, this is despite arriving with similar or better self-reported health than the general Canadian population. 6 Therefore, understanding any barriers to PHC access faced by Canadian immigrants and identifying ways of mitigating them is crucial for Canadian health care and the economy.
Immigrant women have less access to PHC and poorer health outcomes compared to men. Many factors play a role in this disparity, including socially constructed gender roles, sociodemographic variables and the role of women as major caregivers to family and friends in declining health. 9 Further, women face unique PHC needs, such as child and maternal health and certain cancers. 10 This, combined with their newcomer status, makes immigrant women an important target of PHC research, where revealing issues related to care access as a function of sex and gender can create opportunities to strengthen and support improved access to health care for immigrant women and a more sustainable health care system. 11
Few studies have explored the challenges reported by immigrant women while accessing PHC in Canada, most of which were conducted among a single large ethnic groups such as Indian and Chinese immigrants or among a broader ethnic community such as South Asian immigrants. 12 These studies do not capture the true diversity of people migrating to Canada. Previous studies have illustrated that people from varying ethnic and cultural origins perceive different barriers to health care. 12 With approximately 250 ethnic origins and ancestries in Canada, 13 it is important to explore the unique health care challenges faced by Canadians of different ethnic and cultural backgrounds. This granular level understandings will lead toward programs or interventions which can cover a wide spectrum of communities.
Bangladeshi-Canadians are one of the most rapidly growing immigrant community in Canada. Studies showed that the migration rate from Bangladesh had an increased rate of 110% from 2001 to 2011. 14 According to Bangladeshi High Commission in Ottawa, around 100 000 people of Bangladeshi origin live in Canada. 15 Previous studies investigating barriers to accessing health care among South Asian communities in Canada usually included Bangladesh-Canadian immigrants too, nevertheless, Bangladeshi immigrants’ unique socio-cultural, linguistic, and religious nuances may not be reflected adequately in those studies. 16 Islam et al. showed that there are notable differences in the health outcome and the determinants of health within various groups of South Asian population. 17 Ethnic origin within South Asians immigrants may shape their social networks, health behavior, access to health care, and other socio-economic resources that may influence their health outcomes. 18 The Bangladeshi-Canadian immigrants often get lost in the shadow of other bigger South Asian communities, only a handful research explored health-related issues and behaviors of Bangladeshi immigrant women; and that showed Bangladeshi women experienced a significant physical and mental health disparities, and poor health behavior compared to other racial/ethnic groups.19,20 However, to date, not much health-related research has been conducted among the Bangladeshi-Canadian immigrants. The aim of this qualitative research was to gain an in-depth understanding of perceived challenges and unmet PHC access needs of Bangladeshi immigrant women in Canada.
Methods
Using community-based participatory research 21 (CBPR) approach, which is a form of the integrated knowledge translation (iKT), 22 7 focus group discussions (FGDs) among Bangladeshi immigrant women were conducted in Calgary, Alberta. CBPR or iKT brings the community members, community organizations and various stakeholders, in the research process alongside the researchers to identify individual, societal and systemic inequities through a collaborative approach. We have engaged with the Bangladeshi-Canadian community members through several informal conversations that lead us to identify the research question. We also had citizen researchers from the Bangladesh-Canadian community who were engaged in every stage of this research. They helped and guided us in participant recruitment, transcription, translation, analysis, and interpretation of the data. The citizen researchers also contributed to identifying and verifying the themes derived from the FGDs and writing the manuscript. The FGD method was used to collect data as this method has been proven effective for collecting qualitative data especially in the field of health disparity research among minority populations. 23,24 It allows participants to provide detailed information about complex experiences and the rationale behind their beliefs, attitudes, perceptions, and actions. 25 In total, 42 Bangladeshi immigrant women participated in the 7 FGDs. Each FGD consisted of 4 to 8 participants from July to December 2018. The FGDs were conducted in settings of the Bangladeshi-Canadian community organizations for the convenience and accessibility of participants, where privacy and confidentiality were ensured. This study was reviewed and approved by the Conjoint Health Research Ethics Board of our academic institution prior to any research activity commenced. Informed consent was obtained from all the participants.
Recruitment and Participants
FGD participants were recruited according to the following selection criteria:
The participant must be an adult first-generation legal Bangladeshi immigrant woman; and
The participant must have exposure to Canadian PHC.
There are an estimated 3110 first-generation Bangladeshi immigrants living in Calgary, 1515 of whom are women. 26 The first language for the most is Bangla. Based on our selection criteria and considering the distribution of the immigrant population in Calgary, the following recruitment strategies were taken:
English and Bangla posters were distributed in community locations, including Bangladeshi grocery stores, restaurants, and community centers.
A snowball recruitment method was implemented in which key community leaders were identified and contacted for their support in recruiting potential participants. As people were enrolled, they were encouraged to provide additional contacts based on their personal social networks.
Email recruitment invitations were sent through the Bangladesh Canada Association of Calgary email lists to all community members.
Advertisements were posted in the local Bangla newspaper.
A social media campaign was undertaken through Facebook and Twitter.
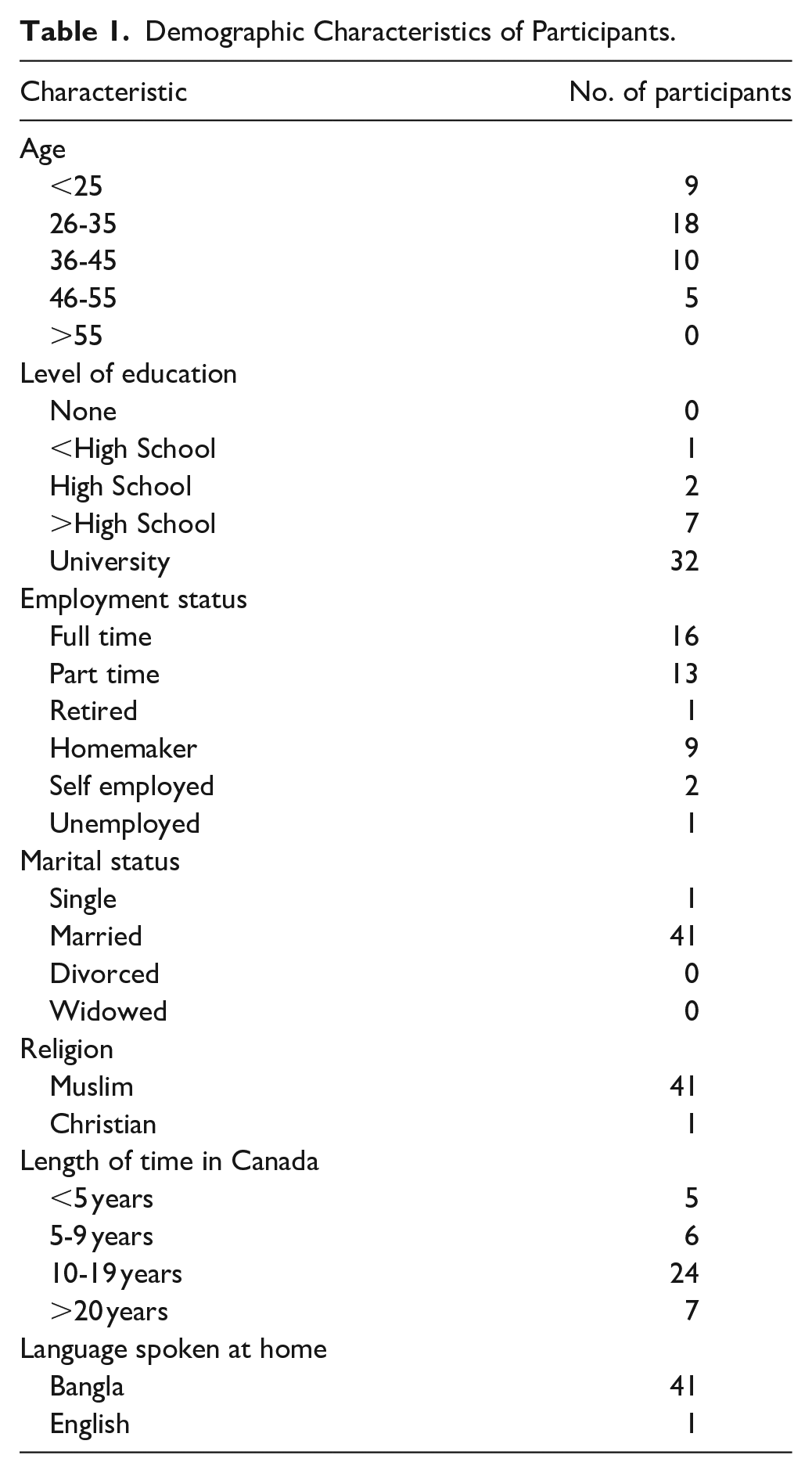
Potential participants were contacted by the study coordinator and were informed about the study objective, either by telephone, by mail (first contact) or in-person (on-site). The demographic details of the participants are illustrated in Table 1.
Demographic Characteristics of Participants.
Conducting the FGDs
FGDs were overseen by a moderator and an assistant moderator cum-note taker, both of whom were bilingual and fluent in both English and Bangla. The FGDs were conducted in Bangla, but the participants were given the option of using either Bangla or English. The moderator applied appropriate working group techniques and provided equal opportunities for communication to all participants. The moderator guided the discussions which addressed the following questions or topics:
General experience with accessing PHC services in Canada;
Perception of important PHC services or health professionals to maintain health;
Accessibility to PHC health services;
Factors affecting access to PHC health services;
Challenges they face for timely and optimal PHC health services
Ways they perceived the access to PHC can be improved; and
The possible role of PHC practitioners, government and community organizations in improving access to health care services.
The moderator occasionally posed open questions to clarify content or context, to deepen the perspectives voiced and to stimulate the flow of discussion if participants’ statements were unclear or if the discussion came to a halt. The assistant moderator acted as a note-taker and was responsible for capturing what was expressed, noting the tone of the discussion and the order in which people spoke (by participant number or name), phrases or statements made by each participant and non-verbal expressions. At the end of each discussion, the assistant moderator summarized the discussion and asked for feedback from the participants. FGDs were audio-recorded and lasted for about 1.5 to 2 h.
Data Analysis
Data analysis was undertaken using the 6 phases of thematic analysis proposed by Braun and Clarke, 27 which includes the following:
Familiarizing oneself with data: All of the recorded FGDs were transcribed verbatim and the complete transcript was compared with the recorded audio and the handwritten notes taken by the note-taker to fill in the gaps.
Generating initial codes: The data from the first 3 focus groups were coded independently in English by 2 bilingual researchers (the research assistant and principle investigator) and discrepancies were resolved by discussion. The remaining FGDs were coded by the research associate and randomly checked by the principal investigator. The coders took the necessary steps to ensure the accuracy of the translation. 28
Searching for themes: In this stage, codes were extracted in Excel files. After analyzing the codes, we collected the relevant codes into potential themes and gathered all data relevant to each potential theme. The guiding framework introduced above was applied at this stage to create themes focusing on the structural and PHC delivery domains of PHC.
Reviewing themes: In this stage, we tested the themes in relation to the coded extracts and the entire data set and generated a thematic map of the analysis.
Defining and naming themes: In this stage of the ongoing analysis, the specifics of each theme were refined to reveal the overall story reflected and clear definitions and names for each theme were generated.
Producing the report: After selecting vivid and compelling extract examples, a final analysis of selected extracts was undertaken to tie the analysis to the research question and literature to produce a scholarly report of the analysis.
Results
As shown in the Table 1, the participants were predominantly educated and in the age range of 26 - 45 years. All but one (41 out of 42) participants were married, Muslim, and Bangla speaking women. Most of the participants were employed either full-time or part-time. Over half of the participants (24 out of 42) migrated to Canada 10 to 19 years ago, where only 5 participants migrated within last 5 years.
Data analysis of the focus group discussions revealed 5 dominant themes. The first theme, “Wait time,” described a prominent challenge commonly encountered by participants in accessing PHC. The second major theme was “Communication gap,” which greatly impacted access to and quality of PHC. The third theme, “Travel and Transportation,” described distance to health care centers and availability of transportation as common barriers that limit access to and utilization of health care services by the participants in this study. The fourth theme, “Health-related cost,” explained how costs related to health care services influenced study participants’ utilization of health care. The fifth theme, “Gaps in walk-in-clinics,” discussed the issues related to walk-in-clinics (i.e., a PHC facility that accepts patients without prior appointment), which discouraged participants from accessing care. All major themes were supported by multiple subthemes as data analysis progressed. Representative quotes from each of the main themes and sub-themes arising from the FGDs are set out in Table 2.
Themes Arising from Focus Group Discussions with Bangladeshi Canadian Immigrant Women Regarding Primary Health Care Access.

Theme I: Wait Time
Wait time were experienced by participants in emergency rooms or a doctor’s clinic, where they expressed frustration for the slow treatment process and the economic losses resulting from absence at work. Participants from all FGDs recognized that long wait time discouraged them from going to the doctor to obtain PHC services.
Long Wait Time at the Emergency Room (ER)
Long wait time at ER was complained by many participants. Waiting hours at ER room not only delayed treatment and kept the patient and attendance worried for long, but also affected their work, school, and other daily activities. Many participants avoided help-seeking due to this long wait time in ER.
Wait Time To Go Through the Treatment Process
Many participants expressed that overall treatment process in Canada is slow, which can be attributed to long wait time in various stages of treatment including finding appointments with specialists, delayed diagnostic services (MRI, CT scan, etc.), and unavailability of family doctors when they got sick. Also, family doctor’s hesitancy for referring to a specialist was expressed.
Appointment Time Not Maintained
Some participants mentioned they had to wait hours at doctor’s office past the given time of the appointment. This caused them missing their other appointments scheduled next, or other important chores such as picking their children from daycare center.
Theme II: Communication Gap
Communication gap, including language barrier and lack of effective communication between patients and physicians, was also discussed by participants.
Language Barrier
Many participants were unable to explain their health issues to the PHC providers due to language barrier. Having limited English and medical vocabulary, and difficulty with understanding accent of the care providers hindered some participants to explain their health issues as well as to follow the doctor’s advice properly.
Lack of Effective Doctor-Patient Communication
Participants expressed their dissatisfaction with physicians that they did not explain the health problems, treatment plans, side-effects from medication or complications of the disease clearly and did not listen to patient’s complaints attentively. Doctors rushed the patients to tell their problem and did not want to listen more than 1 complaint.
Theme III: Travel and Transportation
Many participants highlighted distance from home or workplace to the clinic/hospital as an important barrier to accessing care. Parking fees and inaccessible parking were also mentioned as important barriers to utilizing PHC.
Location of Clinics and Hospitals
The location of the clinics and hospitals being distant from the residence was echoed by some participants. Especially, those who did not drive were discouraged from utilizing care for the long distance. While being sick had already inconvenienced them to use public transport, bad weather may throw additional challenge against using public transport and in turn accessing PHC.
Parking
Participants also pointed that parking a car and paying at the pay station of the hospital while accompanying a sick patient or a wheelchair patient was difficult. Some clinics did not have their own parking; therefore, getting an appropriate parking spot was a challenge. Cost for parking was also expensive and long wait time at the ER or doctors’ clinic burdened even more.
Theme IV: Health-Related Costs
Despite free universal health care services in Canada, some hidden cost namely emergency medical service (EMS) cost and out-of-pocket treatment-related cost was matter of financial burden.
Emergency Medical Service (EMS) Costs
Some participants voiced that the EMS ambulance cost is very high and they opposed this cost for ambulance showing the reason that they already are paying their taxes.
Out-Of-Pocket Health Care Costs
Certain treatments often advised by doctors are not fully covered by the universal health care of Canada such as dental care, physiotherapy, and eye care. Treatment needed in those modalities may be expensive and unaffordable by many participants.
Theme V: Gaps in Walk-In Clinic Services
Most participants in this study regularly or occasionally visited walk-in clinics, especially when they did not have a family physician or could not see their family physician when they were sick. Walk-in clinics in Canada comprise of integrated PHC centers that accept patients on a walk-in basis, with no appointments required, providing the advantage of easy accessibility and faster care. However, participants pointed out certain gaps in walk-in clinic services that discouraged them from utilizing care. This included having no access to patient’s medical records at walk-in clinics, no facility for a follow-up visit and lack of coordination with the patient’s family physician (for example, the walk-in-clinic doctor is not required to provide information to a patient’s regular family doctor after providing care to the patient) were major concerns among the participants.
Discussion
The study found a range of barriers that were categorized under 5 themes and subsequent sub-themes focusing on the structure and health care delivery domains of PHC: (1) Wait time (long wait time at the ER, wait time to go through the treatment process, appointment time not maintained); (2) Communication gap (language barrier, lack of effective doctor-patient relationship); (3) Travel and transportation (location of clinics and hospitals, parking); (4) health-related costs (EMS cost, out-of-pocket costs); and (5) gaps in walk-in clinic services. These themes provide evidence for both universal and specific factor faced by the general population within Canada and immigrant, respectively.
Long wait time, particularly in the ER, was reverberated as a barrier by many FGD participants. Similar to our findings in this study, Canadian-born individuals also reported waiting too long for an appointments or difficulty getting an appointment, as the most common barrier for their PHC access, 4 making it a common occurrence within the Canadian system. This may be due to the below average ratio of population to physician in Canada relative to some other developed countries. 29 Physicians shortages, further, seems to be well-cited issue within immigrant health literature, where physicians clinic representation within predominantly immigrant communities is different from other communities. 30 Accessibility to PHC by immigrant is further influenced by the lack of dedicated clinics for immigrant populations for easier access (i.e., less time travelled to clinic, physician availability) and culturally sensitive integrated care. 31 Lack of continuity across providers in the updating and sharing of patients’ medical records was also highlighted as a challenge for participants in this study.
Communication barriers appear to be a unique and universal encounter for immigrants worldwide that affects their understanding of disease, hampers the doctor-patient relationship and causes an overall dissatisfaction with care,32-34 which has yet to be overcome. Consistent with previous research, our FGD participants reported facing difficulties explaining their issues as well as understanding the doctor’s instructions, which leads to non-compliance. 33 An ineffective doctor-patient relationship due to the hurried attitude of physicians, lack of time spent by physicians explaining, talking and listening to patients, and perceived lack of compassion from physicians also discouraged participants from seeking access to health care. 35 These difficulties can be result of not only ethno-cultural differences between immigrant and health care providers, but also unique conceptualizations of health and illness by immigrants. 36
There is significant amount of literature that cites the socioeconomic difficulties that immigrants face, especially recent migrants. Socioeconomic disparities can be drivers to difficulties faced in affording certain health care services (e.g., medication), also experienced by participants of this FGD. This includes having the social support or security needed to be a sustained health care user. For example, many immigrants do not have the time or funds to afford childcare in order to attend health care appointments, or long travel times using public transportation. Notably, a study using data from the Canadian National Population Health Survey (NPHS) also showed that higher education and income to be associated with accessing PHC services, suggesting this trend to be ubiquitous within the Canadian population. 37 Studies suggested that those with higher educations are able to better realize and communicate their health care needs, and realize the benefits of continuous PHC. 38 This results in a more effective use of the health care system.
Previous studies on immigrant women found certain immigrant women specific barriers to accessing PHC such as preference of female doctors over male doctors, privacy, and modesty concerns with exposing themselves to the health care providers, and sharing room with other patients. 39 In our study, Bangladeshi-Canadian immigrant women also expressed their preference for a female doctor, though they went ahead interacting with the available doctor when they visited the health system. Rest of the reported barriers by our participants aligned with the common barriers reported by both men and women immigrants such as long wait times, communication, transportation barriers, etc. 12 Unlike many other studies on immigrant women, our respondents did not highlight shyness, or modesty concerns in the discussion especially around sexual and reproductive health. 40 This finding may be explained by the characteristics of our study participants. Majority of our participants were educated, married, and were living in Canada for 10 to 19 years. Prior studies indicated that immigrants who are generally educated, 41 married, 42 and those who have been in the host country for a longer time 43 has shown better health awareness as well as overall better access to health care. 7
A fundamental limitation of FGDs is their susceptibility to bias, as group and individual opinions can be swayed by more dominant participants. 44 However, our facilitators were skillful to guide the FGDs in a way to invite every participant to express their opinion. Our study population was limited to Bangladeshi immigrant women whose views may not be representative of other immigrant populations in Canada. Moreover, using snowball sampling may have resulted selection bias to some extent, however, to recruit from a hard-to-reach visible minority group this strategy is often preferred. 45 Our study sample predominantly represented married, educated, Muslim, Bangla speaking, employed, 26 to 45 years old women living in an urban center. Although this sample characteristics may have been influenced by the selection method, it is not a misrepresentation of the Bangladeshi-Canadian immigrant diaspora because of the immigration process through which most Bangladeshi immigrants migrated to Canada. The point-based immigration criterion are favorable for the migration of immigrants who are married, educated, and have certain years of work experience. 46 Nonetheless, the aim of this study was not to generalize, but rather to understand the views of a relatively small immigrant population.
Despite the limitations, our study has generated understanding about the health care challenges of a population that have been reportedly understudied. The strength of our program of research is that we used a community-based participatory research approach 42 that helped us build a trust-based relationship with the Bangladeshi immigrant community and encouraged participants to speak out spontaneously. Furthermore, by using FGD methodology, we were able to build upon everyone’s comments and stimulate thinking and discussion, thus generating new concepts of barriers they face while accessing Canadian PHC. Moreover, due to the community engagement during the research process, the participants showed interest in further implications. Thus, the foundation for future research collaboration with the community was established, which is crucial for identifying the solutions toward improving their access to PHC.
We believe that this study will broaden the understanding of health care providers, policymakers, and researchers of how immigrants perceive their access issues in Canadian PHC system and what unique issues they face. Each ethnic group have their own expectations and preference of health care services, which might be different from current Canadian health care system. Some of those differences can be mitigated by updating the PHC system such as improving interpreter services, training health care providers to improve their cultural competency and others can be addressed by educating the immigrants about Canadian PHC system and how to navigate that, improving their individual and community health and wellness literacy, and providing social support to mitigate socio-economic determinants of health that affect their PHC access. To meet this goal, more community-engaged research in ethnically diverse immigrant groups is needed to understand their unique issues, needs, expectations, and preferences for PHC services. Moreover, in terms of over-reaching policy, health care planning and delivery can benefit from integrating an intersectionality perspective to understand the influence of race and gender in driving health care access disparities. Involvement of the immigrant community in the research process to plan and implement solution measures toward improving PHC utilization and improved accessibility is crucial to effectively improve health behavior and outcomes of the immigrant population in Canada.
Footnotes
Acknowledgements
We would like to acknowledge the engagement and support we have received from the Bangladesh-Canadian grassroots community members in Calgary. Also, we appreciate the encouragement we have received from all the socio-cultural organizations belonging to this community including the leadership of Bangladesh Canada Association of Calgary.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been supported from grant from Canadian Institute of Health Research (201612PEG- 384033).
Ethics approval
The study was reviewed and approved by the Conjoint Health Research Ethics Board of University of Calgary before commencing any research activity (Ethics ID: REB15-2325).