
Abstract
Background
Most older adults with comorbidities in primary care clinics use multiple medications and are at risk of potentially inappropriate medications (PIMs) prescription.
Objective
This study examined the prevalence of polypharmacy and PIMs using Thai criteria for PIMs.
Methods
This study was a retrospective cross-sectional study. Data were collected from electronic medical records in a primary care clinic in 2018. Samples were patients aged ≥65 years old with at least 1 prescription. Variables included age, gender, comorbidities, and medications. The list of risk drugs for Thai elderly version 2 was the criteria for PIMs. The prevalence of polypharmacy and PIMs were calculated, and multiple logistic regression was conducted to examine associations between variables and PIMs.
Results
Of 2806 patients, 27.5% and 43.7% used ≥5 medications and PIMs, respectively. Of 10 290 prescriptions, 47% had at least 1 PIM. The top 3 PIMs were anticholinergics, proton-pump inhibitors, and nonsteroidal anti-inflammatory drugs (NSAIDs). Polypharmacy and dyspepsia were associated with PIM prescriptions (adjusted odds ratio 2.48 [95% confident interval or 95% CI 2.07-2.96] and 3.88 [95% CI 2.65-5.68], respectively).
Conclusion
Prescriptions with PIMs were high in the primary care clinic. Describing unnecessary medications is crucial to prevent negative health outcomes from PIMs. Computer-based clinical decision support, pharmacy-led interventions, and patient-specific drug recommendations are promising interventions to reduce PIMs in a primary care setting.
Keywords
Introduction
Most older adults have multiple morbidities and use primary care services for their health conditions. These older adults often require multiple medications and are at risk of polypharmacy. Recent research reports that 33.3% of elderly patients in a primary care setting use 5 or more concurrent medications. 1 Elderly patients with polypharmacy have a high chance of drug-related problems, such as potentially inappropriate medications (PIMs)2,3 and non-medication adherence.4,5
PIMs are medications that should be avoided or used with caution in older adults. There are 5 general categories for PIMs 2 : (1) Medications that are generally inappropriate because of physiological change in older adults; (2) Medications that are not appropriate because of renal impairment; (3) Medications that are not appropriate because of drug-drug interactions; (4) Medications that are not appropriate because of patients’ conditions; and (5) Medications that need lower dosages. Elderly patients with PIMs reported higher negative health outcomes than those without PIMs. For example, 1 study reports that elderly patients with PIMs were hospitalized 1.25 times higher than those without PIMs (Risk Ratio (RR) 1.25, 95% CI 1.09-1.44). 6
Almost one-third of older adults receive 1 PIM each year. 7 The most common PIMs vary depending on countries and criteria for PIMs. In the USA, digoxin in doses greater than 0.125 mg/day, glyburide, and estrogen are the top 3 PIMs using the 2012 Beers criteria. 8 According to the Dutch version of the STOPP/START criteria, salicylates, NSAIDs, and opiates are the top 3 PIMs in Netherland. 7 In Thailand, orphenadrine, dimenhydrinate, and benzodiazepine are the most common PIMs prescribed according to the 2015 Beers criteria, while benzodiazepine and first-generation antihistamine were common in STOPPv2. 9
Trends in potentially inappropriate prescriptions in primary care settings vary. The study in the USA reported a decrease in the PIM prevalence from 37% to 34% in 2007 and 2012, respectively. 8 In Ireland, the prevalence of PIMs increased over time from 39.7% in 2010 to 45.6% in 2015. 10 The prevalence of PIMs increases when a newer version of criteria for PIMs is applied. For example, a study in China finds that the prevalence of PIMs using Beer 2015 was 8.8% higher than the prevalence of PIMs using Beer 2012. 11 The 2019 Beers criteria also have more additions than deletions of PIMs from its 2015 version. 2 Similarly, STOPPv2 has more criteria of PIMs than those in STOPPv1. 3
The primary objective was to examine the prevalence of PIMs in the primary care clinic to monitor PIM prescribing for older adults following the study in 2016. 9 We also examined factors associated with PIMs.
Methods
Study Design and Setting
A retrospective cross-sectional study was conducted in 2019. Data were obtained from the Primary Care and Applied Thai Traditional Medicine center, Faculty of Medicine, Thammasat University. The center provides primary care services for approximately 24 000 patients with a universal health coverage scheme in a Kukot municipality in Pathum-Thani province. The study protocol was approved by The Human Research Ethics Committee of Thammasat University no.1 (Faculty of Medicine) (Grant No. MTU-EC-CF-1-041/62). A director of the center granted permission to conduct research.
Samples
Samples were patients aged 65 years old or more, who visited the center between January and December 2018. The patients were excluded from the study if (1) they visited the center for reasons other than doctor visits and (2) they did not have a prescription. We collected data of all patients, who met inclusion criteria but not exclusion criteria.
Data Collection
Data without identifiable information were obtained from electronic medical records. Variables include age, sex, principal diagnosis, and comorbidities using codes from the International Classification of Disease, the 10th revision (or ICD-10), and prescription details, including medications, dosage, and administration. A health information administrator of the center retrieved and submit data to the authors in an excel format. The authors asked the administrator to recheck the data if there were incomplete or possibly incorrect.
Criteria for PIMs
This study used the Lists of Risk Drugs for Thai Elderly or LRDTE. 12 An expert panel in geriatrics and clinical pharmacology developed the LRDTE based on Beers 2012 13 and Screening Tool of Older Persons’ Prescriptions version 1. 14 The LRDTE did not include drug-drug interactions, drug-syndrome interactions, and drug-disease interactions. The LRDTE divided older people into groups of 60 to 74 and 75 years old or older with different recommendations for some criteria. The LRDTE was revised with minor changes in recommendations (unpublished) after Beers 2015 15 and STOPP version 2 3 had been published. A total of the criteria in this second version did not change.
The LRDTE comprised 8 medication groups with a total of 77 PIMs: (1) anticholinergics, (2) antithrombotics, (3) anti-infective, (4) cardiovascular, (5) central nervous system, (6) endocrine medicine, (7) gastrointestinal medicine, and (8) pain management. Recommendations for each criterion include mild (use for a specific condition, short-term use, or use with close monitoring), moderate (avoided by using other safer medications), and severe (not recommended). Some criteria have specific advice. For example, trihexyphenidyl is for short-term use with a low dose and only for tremor and EPS from antipsychotic agents. The LRDTE also includes rationales for PIMs based on STOPP and Beers criteria.
The LRDTE detected 79% of elderly patients in general hospitals with amlodipine as the most common PIM (32%). 12 In a primary care setting, the prevalence of PIMs, according to the LRDTE version 1, varied from 20% to 45% (unpublished).
Analysis
Similar to other studies,16,17 only oral medications were included for the analysis to not overestimate the polypharmacy prevalence. Descriptive statistics were used to describe patients’ characteristics, the prevalence of polypharmacy (use of 5 or more medications) and PIMs. Percentages of each PIM were calculated to identify the most common PIMs. Analytical statistics were conducted to analyze associations between independent variables (age, gender, ICD-10, and polypharmacy) and PIMs. Multiple logistic regression was conducted to calculate adjusted odds ratios.
Results
Patients’ Characteristics
Data of 2806 patients were obtained. The mean age was 70.6 years (SD = 7) and two-thirds were women (Table 1). About 2.5% of the patients had chronic kidney disease stage 4 and 5. Hypertension and type-2 diabetes were the most common diagnoses.
Patients’ Characteristics from January to December 2018 (n = 2806).

Abbreviations: CKD, chronic kidney disease; PIM, potentially inappropriate medications.
Polypharmacy
Of all the patients, 27.4% used 5 or more concurrent medications. Polypharmacy is associated with older age (adjusted odds ratio or AOR = 1.017, 95% CI 1.006-1.028) and type 2 diabetes (AOR = 1.84, 95% CI 1.37-2.47) (Table 2). The patients with benign prostate hypertrophy (BPH) or dyslipidemia (DLP) had a lower chance of having polypharmacy than those without BPH (AOR = 0.29, 95% CI 0.12-0.70) or DLP (AOR = 0.39, 95% CI 0.26-0.59). Gender and other diseases, such as dyspepsia and hypertension, were not associated with polypharmacy.
Multivariate analysis of polypharmacy (January to December 2018).

Potentially Inappropriate Medications
Of the patients, 43.7% had a prescription with PIMs in the past year. The most prescribed PIMs were anticholinergics (22.2%), omeprazole (20.8%), and nonsteroidal anti-inflammatory drugs or NSAIDs (12.0%) (Table 3).
The most common PIMs from a total of 7436 PIMs (January to December 2018).

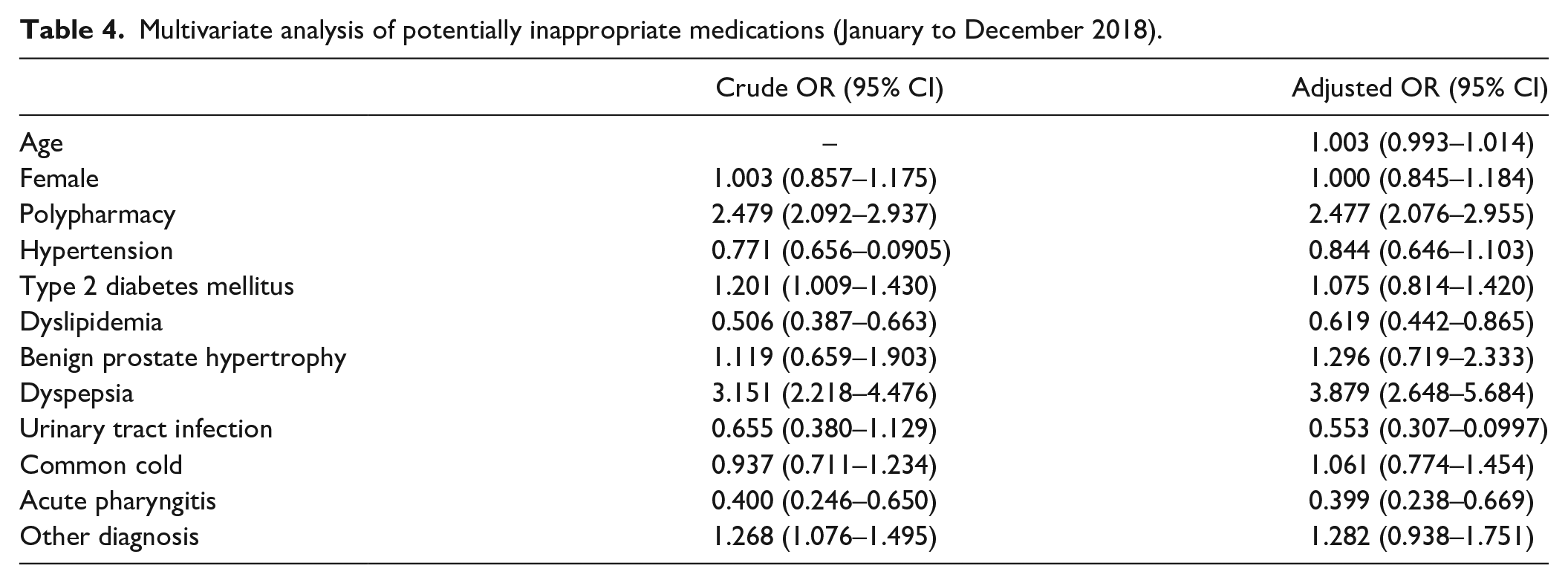
Factors associated with PIM use were polypharmacy (AOR = 2.48, 95% CI 2.07-2.96) and dyspepsia (AOR = 3.88, 95% CI 2.65-5.68) (Table 4). The patients with DLP had lower odds of using PIMs than their counterparts (AOR = 0.62, 95% CI 0.44-0.87). Age and gender were not associated with PIMs.
Multivariate analysis of potentially inappropriate medications (January to December 2018).
Discussion
This study examined potentially inappropriate medications prescribed for elderly patients in a primary care clinic using the LRDTEv2 to monitor the prevalence of PIM use. The previous study conducted in the same clinic 2 years ago reported 53.3% of polypharmacy and 59% of PIMs according to the Beers 2015 criteria. 9 Our current study found that the prevalence of polypharmacy and PIMs was still high, though it was lower than the previous study. The most PIMs prescribed for the patients were anticholinergics, omeprazole, and NSAIDs, which were different from the previous study. 9
The prevalence of polypharmacy in a primary care setting varies from country to country, ranging from 5% to 77%. In Portugal, 77% of 757 samples were prescribed polypharmacy (≥5 medications). 18 The median number of medications in the samples was 8. 18 In England, 27.6% and 7.4% of older adults received polypharmacy (5-9 medications) and hyperpolypharmacy (≥10 medications), respectively. 19 In total, 35% received 5 or more concurrent medications. In Brazil, about 20.5% of patients received polypharmacy. 20 In contrast, only 5% of Indonesian elderly patients received polypharmacy. 21 The prevalence of polypharmacy in our study was similar to Brazil and England. These studies do not mention the most common medication categories prescribed to the patients. Given that older age and multiple comorbidities were strongly associated with polypharmacy, 22 most medications prescribed for these patients are possible for their comorbidities. 23
A recent literature review found many determinants of polypharmacy, including poor health conditions, increasing age, low health educational attainment, and multiple OPD visits. 22 In our study, 2 factors associated with polypharmacy were older age and diabetes. The older the people, the more medications they require for their health conditions, such as hypertension and diabetes. 24 Data from a 37-month cohort study found that the risk of receiving polypharmacy in older adults, who were not exposed to polypharmacy, was 19.9 per 100 person-years and increased with age. 25
Polypharmacy results in poor health outcomes, though direct effects were from older age, poor health conditions (requiring multiple medications), and potentially inappropriate medications 22 rather than the number of medications itself. These negative health outcomes include frailty, hospitalization, and mortality. In an 8-year longitudinal study, every additional medication since the baseline increased the risk of frailty by 11%. 26 In the same study, the risk of frailty increased by 55% and 147% for patients with 4 to 6 medications and ≥7 medications, respectively. Similarly, those with polypharmacy had a higher chance of hospitalization compared to their counterparts. 27 Using 5 or more medications was also related to deaths. 28 The authors mention that using dose categories, the risk of death increased with the number of prescribed medications (5, 6-9, and ≥10 with adjusted OR of 1.31, 1.59, and 1.96, respectively).
Our study reported a higher prevalence of PIMs than other studies, ranging from 29.7% to 37% 1 ; however, the prevalence of PIMs is not different from studies published after 2015 (43.6% from other studies vs 47% from our study). Studies using the 2015 Beers criteria reported 40.4% of PIM users. The 2015 Beers criteria are better than their previous versions in detecting PIMs 11 ; therefore, studies using the 2015 Beers criteria usually report the high prevalence of PIMs. Zhang et al. 11 found that proton-pump inhibitors in the 2015 Beers criteria significantly increased the PIM prevalence.
The top 3 PIMs in our study were anticholinergics, omeprazole, and NSAIDs. Anticholinergics increase the risk of functional and cognitive decline, falls, vascular events, and hospitalization. 29 Assessing anticholinergic burdens and deprescribing anticholinergics is vital to prevent anticholinergic use in older adults. Despite the anticholinergic risk and deprescribing interventions, the prevalence of anticholinergic use is on the rise. 30 Recently, little is known about barriers to reduce anticholinergic use in older adults. 31 Future research should identify such barriers to guide doctors and pharmacists to avoid prescribing anticholinergics to older patients.
As shown in our study and other studies, prescribing proton-pump inhibitors (PPIs) in older adults is common.18,32 Indications for prescribing PPIs include gastroprotection in a high-risk group, treatment for gastric diseases, and maintenance use for chronic gastric conditions. 33 As PPI use increases, concerns about adverse effects, particularly in long-term use, have been raised. The potential side effects include Clostridium difficile infection, bone fracture, vitamin B12 deficiency, and hypergastrinemia34,35; yet, the strength of evidence indicating an association between PPIs and side effects is weak. The best practice is to prescribe PPIs when indicated and deprescribe for those without indication. Deprescribing strategies include stopping, stepping down, and reducing. 36 Other methods include, for example, pharmacist-led 37 or computerized decision support tools. 38
Inappropriate use of NSAIDs was high in our study. Older adults often have musculoskeletal problems, such as muscle strain, low back pain, and knee osteoarthritis. NSAIDs effectively alleviate pain from such problems. A major concern of NSAIDs use in older adults is gastrointestinal bleeding and acute kidney injury. The 2019 Beers criteria suggest avoiding chronic use of COX non-selective NSAIDs in older adults unless no alternatives and patients can take gastroprotective agents. 2 Patients with heart failure, history of gastric or duodenal ulcer, chronic kidney disease stage 4 or 5, or concomitant use of steroid or warfarin should avoid NSAIDs. Recommendation from professional societies is to prescribe NSAIDs with the shortest duration and lowest effective dose. 39
There are some limitations to our study. Samples came from 1 primary care center. Other primary care clinics with different contexts must cautiously interpret and use our findings. The criteria list for PIMs in our study is not as extensive as the 2019 Beers criteria and STOPP version 2; therefore, the prevalence of PIMs could be underestimated. For example, we did not identify drug-drug interactions and drug-disease interactions as defined in the Beers criteria.
Conclusion
The prevalence of PIM use is still high in primary care clinics. Future research needs to find supporting factors and barriers to avoid and deprescribe unnecessary medication. These may include computer-based clinical decision support, pharmacy-led interventions, and patient-specific drug recommendations.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211035088 – Supplemental material for Elderly Patients in Primary Care are Still at Risks of Receiving Potentially Inappropriate Medications
Supplemental material, sj-docx-1-jpc-10.1177_21501327211035088 for Elderly Patients in Primary Care are Still at Risks of Receiving Potentially Inappropriate Medications by Pasitpon Vatcharavongvan and Viwat Puttawanchai in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors are grateful to Miss Nattaya Puangsin for kindly facilitating data collection. We also thank the Head of the Primary Care and Applied Thai Traditional Medicine center for allowing us to conduct research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Clinical Research Funding, Faculty of Medicine, Thammasat University (Grant No. 01/2019)
Ethical Approval
This study received ethical approval from the Human Research Ethics Committee of Thammasat University No.1, Faculty of Medicine (MTU-EC-CF-1-041/62).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.