
Abstract
Keywords
Introduction
Patients who do not have a regular family physician (ie, unattached patients) often cannot use health care services appropriately, relying on emergency departments or walk-in clinics to access primary care services.1,2 Studies have found that patients with a regular family physician benefit from more preventive care,3,4 better care coordination,5-7 greater continuity of care,8,9 better chronic disease management,10,11 and improved health outcomes.12,13
However, more than 15% of Canadians are unattached, 14 placing Canada among the weakest OECD countries with regard to having a regular family physician. 15 To address this critical concern, 7 Canadian provinces have implemented centralized waiting lists for unattached patients to coordinate the supply and demand for attachment to a primary care provider. 16 Few studies have been conducted on these centralized waiting lists. 16 Only 1 previous study examined the amount and type of patients attached through centralized waiting lists. 17 This study suggested that physicians seemed to prefer attaching nonvulnerable patients, regardless of a larger financial incentive for attaching vulnerable patients. 17 However, because the study used provincially aggregated data, it was impossible to describe the characteristics of physicians who had attached new patients through centralized waiting lists and to examine the association between those characteristics and physician participation in centralized waiting lists. Gaining a better understanding of the association between family physicians’ characteristics and their participation in centralized waiting lists may provide useful information for policy makers seeking to increase attachment in primary care.
Aim of The Study
The objective of this study is to analyze the association between family physicians’ characteristics and the amount and type of patients they attached through centralized waiting lists.
Intervention: Centralized Waiting Lists for Unattached Patients
In Canada, the province of Quebec has the highest proportion (28%) of patients reporting that they do not have a regular family physician. 18 To address this issue, the government of Quebec implemented 93 centralized waiting lists for unattached patients across the province, the Guichets d’accès aux clientèles orphelines (GACO). Having attached more than 800 000 patients since their implementation in 2008, 17 Quebec’s GACOs are the largest centralized waiting lists for unattached patients in Canada. GACOs aim to facilitate patient attachment to a family physician in their local health network, based on both medical vulnerability and family physician availability. Patients are defined as medically vulnerable if they self-report at least 1 of 19 vulnerability codes as defined provincially by Quebec’s health insurance (eg, cancer, depressive disorders) or are older than 70 years. 19 The GACOs’ nurses may also contact patients by phone to complete the self-reported information.
Family physicians’ participation in GACOs is voluntary. They can contact their local GACO intermittently to attach the desired number and type of new patients. To encourage family physicians to attach new patients, particularly those considered medically vulnerable, financial incentives were put in place. 20 At the time of the study, physicians received a one-time financial incentive of $23 for nonvulnerable patients and $150 for vulnerable patients for up to 150 new patients per year, except for physicians who had been practicing four years or less who were not limited. These incentives were paid on the patient’s first visit to the family physician. Physicians could receive the incentive regardless of the primary care model in which they practiced and type of remuneration.
Setting
With a population of 8.3 million people, Quebec is the second most populous province in Canada. Quebec has a tax-based health care system with universal health insurance coverage for medical services. 21 In this system, primary care is delivered in several different models (see Table 1). All models are publicly funded, even those that are privately owned and managed by self-employed family physicians. The large majority of family physicians are paid fee-for-services (approximately 70%). 22 Family physicians in all models of primary care are encouraged to attach patients. In addition, physicians must dedicate part of their time to particular medical activities (activités médicales particulières) such as practicing in the emergency department or in long-term care facilities. 23 The nature of the activities is determined according to regional priorities, while the number of hours is determined provincially according to the years of practice (eg, 12 h/wk for physicians who have been practicing less than 20 years). 23
Comparison of Primary Care Models in Quebec, 2013-2015.

Methods
Study Design and Participants
We conducted a cross-sectional observational study using administrative data from the information system related to GACOs. Data were extracted from the databases of 5 local health networks, representing approximately 12% of the province’s population, which were selected to contrast GACOs with varying performances. 21 All variables available in this database were included in the study. All family physicians (n = 580) who had attached at least 1 GACO patient between April 1, 2013 and March 31, 2015 were included. We used the Consommation et Offre Normalisée des Services Offerts par les Médecins (CONSOM) database to compare the number of family physicians in our study and the total number of full-time equivalent physicians by local health network. 24 This study was approved by the Research Ethics Committee of Centre Hospitalier de l’Université de Sherbrooke (reference number MP-31-2015-819: 14-091). Informed consent was not necessary because data were anonymized.
Dependent Variables
The 2 main outcomes were the number of GACO patients attached and the percentage of vulnerable patients among GACO patients attached per physician. In the database, family physicians were identified by a medical license number. Using these identifiers, we extracted the number of GACO patients attached per physician during the study period and the percentage of vulnerable patients (ie, at least 1 of 19 health conditions or older than 70 years) among the total number of GACO patients per physician.
Independent Variables and Covariates
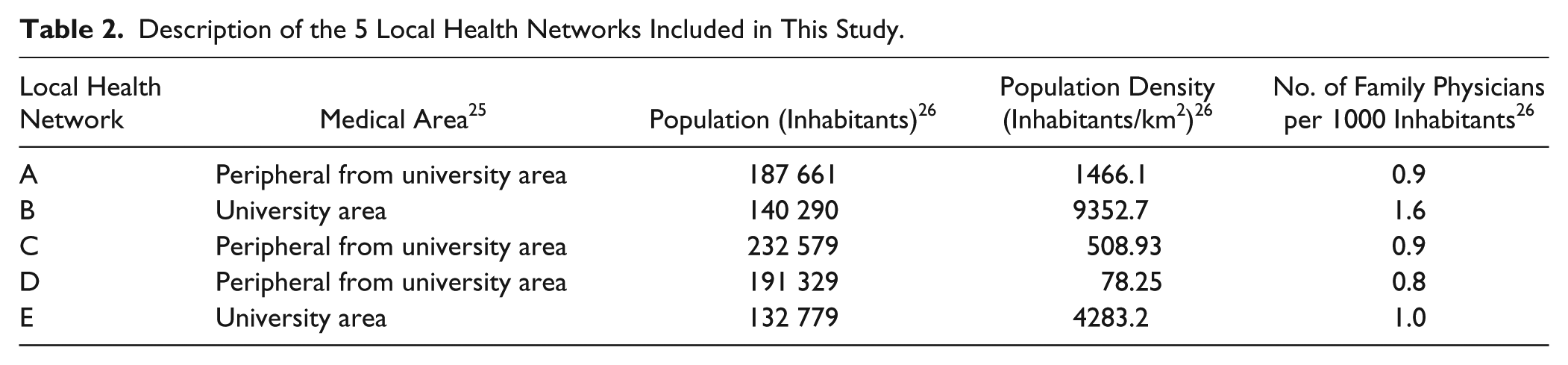
Two main independent variables were included in our analysis: the number of years of experience as a family physician and the model of primary care practice. We calculated the number of years of practice between the year the medical license was issued and 2015 and grouped physicians into categories based on relevant policy (eg, physicians with 0 to 4 years of experience can receive unlimited financial incentives for attaching GACO patients 20 ; physicians with more than 20 years of experience are exempted from having to practice in an emergency departments or other regional priority settings 23 ). Clinics were identified as being family medicine groups (FMGs), family medicine units (FMUs), centres locaux de services communautaires (CLSCs), network clinics, or traditional models. We also included the local health network (identified from A to E; Table 2) and the number of physicians who had attached GACO patients in a given clinic as covariates because we hypothesized that local context and peer pressure from other physicians in the clinic might influence the relationship between our explanatory variables and main outcomes.
Description of the 5 Local Health Networks Included in This Study.
Statistical Analysis
Descriptive statistics were performed for all variables. We developed multiple linear regression models to test the association between the explanatory variables and the main outcomes, adjusted for covariates. All statistical analyses were conducted using SAS 9.3.
Results
A total of 580 family physicians in 124 clinics had attached at least 1 patient from the GACO. The family physicians’ characteristics are shown in Table 3. Physicians with 21 to 30 years and ⩾31 years of practices and those in traditional models of primary care and FMG represented the largest number of physicians who had attached at least 1 GACO patient during the study period. The percentage of physicians who attached at least one patient per local health network represented a large proportion of all full-time equivalent physicians, ranging from 48% to 87% in different local health networks.
Characteristics of Family Physicians Who Attached GACO Patients (n = 580 Physicians) in 2013-2015.

Abbreviations: GACO, Guichets d’accès aux clientèles orphelines; FMG, family medicine group; FMU, family medicine unit; CLSC, Centres locaux de services communautaires.
Traditional models (eg, solo or group practice, etc); network clinics (walk-in clinics with access to laboratory and radiology equipment; FMGs (team-based models); CLSC (community health and social services centers); FMUs (teaching units for residents).
Number of GACO Patients Attached per Physician
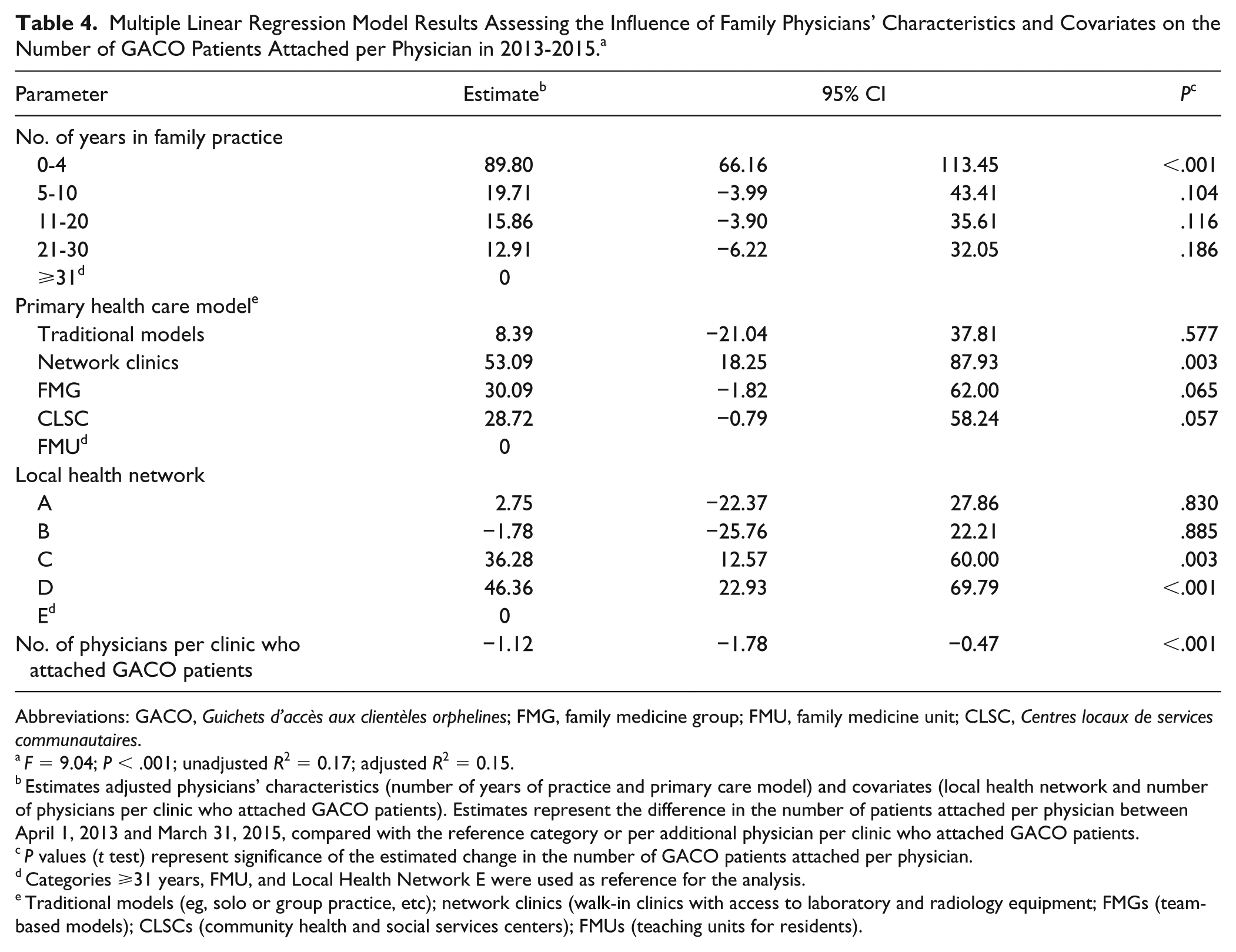
Collectively, 31 526 GACO patients had been attached, for an average of 54 patients per physician (SD ±90 patients; median, 22; interquartile range, 7-56; range 1-939). The results of the multivariate regression (Table 4) suggest that being a family physician with less than 5 years of practice was significantly associated with an increase in the number of GACO patients attached (P < .001), with early career physician having attached nearly 90 patients more than physicians with more than 30 years of practice. With regard to model of primary care, physicians in network clinics attached significantly more GACO patients than those in FMUs (β = 53.09, P = .003). Moreover, with every additional physician in a clinic who had attached GACO patients, the number of GACO patients attached per physician decreased by one. The R2 statistic indicates that 15% of the variation in the number of GACO patients attached per physician was explained by the independent variables included.
Multiple Linear Regression Model Results Assessing the Influence of Family Physicians’ Characteristics and Covariates on the Number of GACO Patients Attached per Physician in 2013-2015. a
Abbreviations: GACO, Guichets d’accès aux clientèles orphelines; FMG, family medicine group; FMU, family medicine unit; CLSC, Centres locaux de services communautaires.
F = 9.04; P < .001; unadjusted R2 = 0.17; adjusted R2 = 0.15.
Estimates adjusted physicians’ characteristics (number of years of practice and primary care model) and covariates (local health network and number of physicians per clinic who attached GACO patients). Estimates represent the difference in the number of patients attached per physician between April 1, 2013 and March 31, 2015, compared with the reference category or per additional physician per clinic who attached GACO patients.
P values (t test) represent significance of the estimated change in the number of GACO patients attached per physician.
Categories ⩾31 years, FMU, and Local Health Network E were used as reference for the analysis.
Traditional models (eg, solo or group practice, etc); network clinics (walk-in clinics with access to laboratory and radiology equipment; FMGs (team-based models); CLSCs (community health and social services centers); FMUs (teaching units for residents).
Percentage of Vulnerable Patients Among GACO Patients Attached per Physician
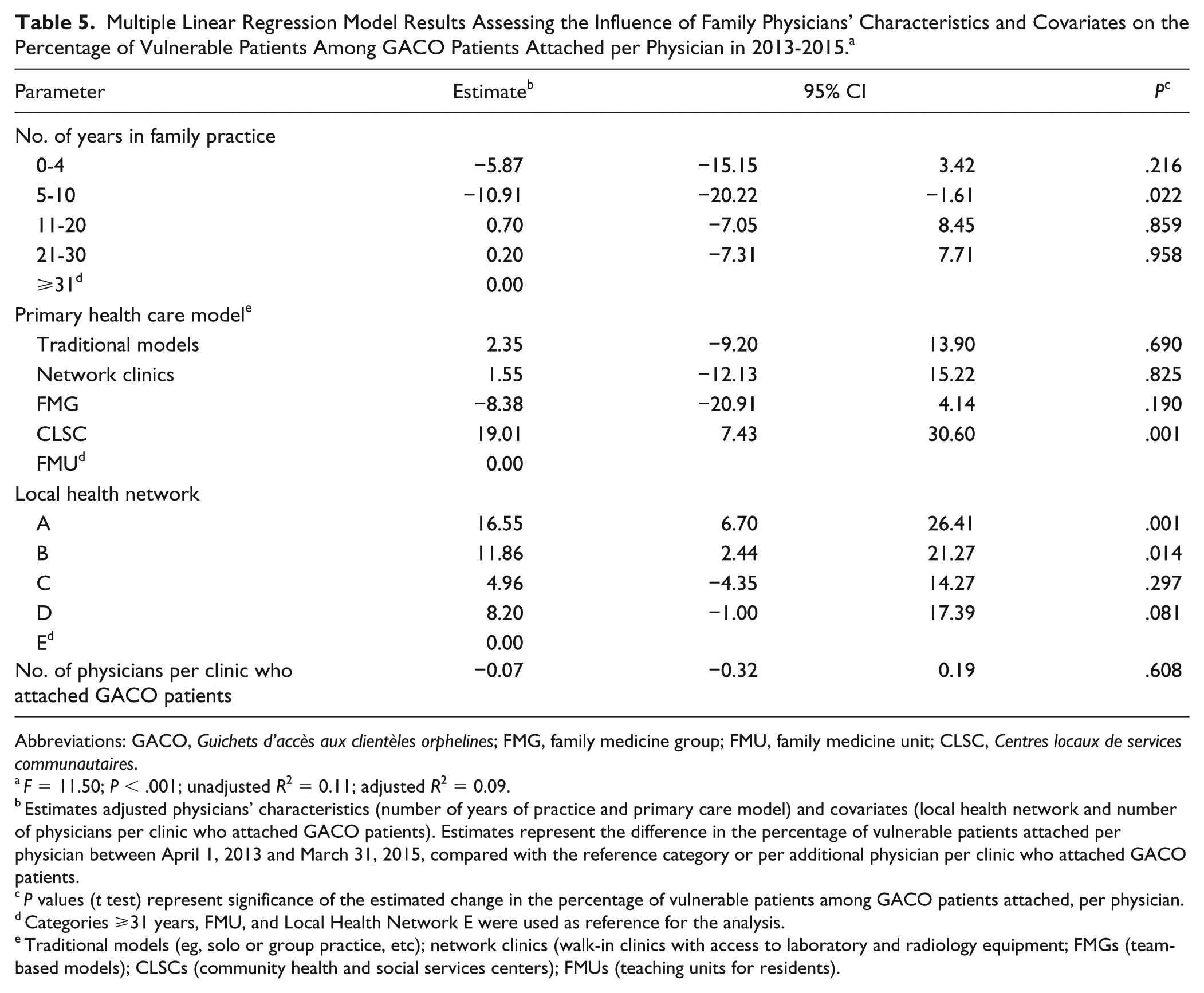
On average, 41.84% of GACO patients attached per physician were vulnerable (SD ±34.19%; range 0%-100%). The results of the multivariate regression (Table 5) show that being a family physician with 5 to 10 years of practice was significantly associated with a decrease in the percentage of vulnerable patients attached (P = .022), with these physicians having attached nearly 11% less vulnerable patients than physicians with more than 30 years of practice. With regards to model of primary care, physicians in CLSCs attached a significantly larger proportion of vulnerable patients than those in FMUs (β = 19.01, P = .001). The number of physicians who attached GACO patients in the clinic was not significantly associated with the percentage of vulnerable patients. The R2 statistic indicates that 9% of the variation in the percentage of vulnerable patients among GACO patients per physician was explained by the independent variables included.
Multiple Linear Regression Model Results Assessing the Influence of Family Physicians’ Characteristics and Covariates on the Percentage of Vulnerable Patients Among GACO Patients Attached per Physician in 2013-2015. a
Abbreviations: GACO, Guichets d’accès aux clientèles orphelines; FMG, family medicine group; FMU, family medicine unit; CLSC, Centres locaux de services communautaires.
F = 11.50; P < .001; unadjusted R2 = 0.11; adjusted R2 = 0.09.
Estimates adjusted physicians’ characteristics (number of years of practice and primary care model) and covariates (local health network and number of physicians per clinic who attached GACO patients). Estimates represent the difference in the percentage of vulnerable patients attached per physician between April 1, 2013 and March 31, 2015, compared with the reference category or per additional physician per clinic who attached GACO patients.
P values (t test) represent significance of the estimated change in the percentage of vulnerable patients among GACO patients attached, per physician.
Categories ⩾31 years, FMU, and Local Health Network E were used as reference for the analysis.
Traditional models (eg, solo or group practice, etc); network clinics (walk-in clinics with access to laboratory and radiology equipment; FMGs (team-based models); CLSCs (community health and social services centers); FMUs (teaching units for residents).
Discussion
Main Findings
Our results show that early career physicians (0-4 years) attached a larger number of GACO patients (90 patients more, P < .001) and that physicians with 5 to 10 years of experience attached a smaller proportion of vulnerable patients (11% less, P = .022) compared with physicians who had been practicing for 30 years or more. Moreover, our regression models showed significant differences in GACO participation according to both local health network and models of primary care (network clinics physicians attaching more patients (β = 53.09, P = .003) and CLSC physicians attaching a larger proportion of vulnerable patients (β = 19.01, P = .001) compared with FMU physicians). The participation of a high number of family physicians in 2 local health networks (C and D) may be influenced by the leadership of the local medical coordinator and the involvement of the family physicians in the community. In a previous study, local dynamics have been shown to influence the implementation of new models of primary health care the establishment of interorganizational collaborations among primary health care practices. 27
Centralized Waiting Lists and Patient Panels
To our knowledge, our study is the first to examine individual physician level factors associated with the attachment of new patients through centralized waiting lists. However, because centralized waiting lists are a mechanism through which physicians can add new patients to their panels, it is relevant to compare our findings to studies on patient panels. The scientific and gray literature suggests that early career physicians’ patient panels are generally smaller than those of more experienced physicians but tend to increase over time as physicians build their panels.28-33 This is consistent with our finding that early career physicians (0-4 years of experience) attach more GACO patients as they are building their panels, while physicians with more experience attach fewer. Additional analysis conducted among this group (0-4 years of experience) showed that only 9% of early career physicians attached more than 150 patients per year even if there is no limitation for these physicians regarding the number of patients attached per physician. Interestingly, we also found that after 5 years of practice this effect is no longer significant and that physicians with 5 to 10 years of experience actually attach a smaller proportion of vulnerable patients compared with physicians with 30 or more years of experience. One hypothesis for this is that physicians with 0 to 4 years of experience are looking to build a diversified patient panel and therefore are attaching a proportion of vulnerable patients similar to that of physicians with 30 or more years of experience, whereas physicians with 5 to 10 years may be avoiding adding vulnerable patients to their panels, although we did not find anything on this in the literature. In Quebec, physicians with more than 20 years of experience are exempted from particular medical activities and, therefore do not have to practice in the emergency room or other regional priority settings. 23 These doctors might therefore have more time to see new patients and prefer to attach less patients with more complex health profiles. It has also been reported that older physicians tend to care for patients who are older.34,35 Therefore, another possible explanation is that older physicians might be more likely to attach patients who are 70 years and older—a criterion for medical vulnerability—which may have led them to attach a larger proportion of vulnerable patient.
Collective Effect of Physician Participation
While late-career physicians (21-30 and 31+ years of practice) are not those attaching the largest number of patients, they represent more than half of physicians who had participated in the GACOs. Similarly, physicians practicing in traditional models of primary care and practicing in FMGs accounted for more than 60% of physicians who had attached at least one GACO patient during the study period. One possible explanation is there are simply more late-career physicians than early-career physicians and more physicians practicing in traditional models and FMGs than in other models in Quebec. 36 The participation of these physicians in the GACOs, although of limited effect individually, accounts for a large number of patients attached through centralized waiting lists collectively and may represent an interesting potential for increasing overall attachment.
Implications for Policy
Our analysis provides new insight on attachment, which may be useful to inform policy. First, because early career physicians seem to be attaching larger numbers of GACO patients to build their patient panels, one way to encourage their participation may be to provide them with administrative support to manage the influx of new patients. Second, compared with other models of primary care, FMU physicians do not seem to be leading in terms of GACO participation. This may be of concern for policy makers as FMUs are intended to be environments in which residents are exposed to best practices that they are to later integrate into their own practice. Third, physicians in CLSCs seem to be attaching a larger percentage of vulnerable patients compared to FMU physicians. While physicians in both models are salaried, it may be that physicians in CLSCs are better supported to attach vulnerable patients because they have access to a range of allied health professionals and programs for complex patients (eg, chronic disease management). Our results therefore suggest that providing physicians with this type of support may lead to increased attachment of vulnerable patients.
Moreover, a recent study in 7 Canadian provinces found that despite variations in the design of centralized waiting lists for unattached patients, provinces faced similar challenges with capacity shortages to meet the demand for attachment and difficulties attaching vulnerable patients. 37 The study also reported that many of the provinces had limited monitoring information to evaluate their centralized waiting lists. 37 Therefore, the results of our study may provide useful insight to other jurisdictions with limited monitoring information, interested in developing strategies to encourage family physician participation in centralized waiting lists.
Strengths and Limitations
The strengths of our study include having data for all physicians who had attached at least 1 GACO patient in the 5 local health networks and selecting local health networks based on performance reducing the risk of a selection bias. However, we were limited to the data available in the administrative database and could not differentiate between solo and group practices within traditional models of primary care. Our multivariate models explain 15% and 9% of the variation of the dependent variables and we were not able to include other physician factors (eg, age, gender, complexity, and size of current patient panel) that could influence physicians’ participation in GACOs.31,33,38 Furthermore, our analysis did not include socioeconomic patient-level variables that have been reported to influence physicians’ panels (eg, migration status, poverty, employment status) 28 and that might have influenced the number and type of patients attached by physicians. We also had no information on physicians who had not attached GACO patients, who could have different characteristics. However, physicians who attached at least 1 GACO patient represented more than 65% of all full-time equivalent family physicians in the 5 local health networks under study. Finally, patients’ vulnerability status was treated as a dichotomous variable (vulnerable/nonvulnerable) as per GACO financial incentives, which does not account for the level of complexity of vulnerable patients.
Conclusion
Centralized waiting lists for unattached patients in primary care have been implemented in 7 Canadian provinces to coordinate the supply and demand for attachment to a primary care provider. The effectiveness of centralized waiting lists to help patients find a family physician greatly depends on family physicians’ participation in these centralized waiting lists. Our results provide a first look at physicians’ participation in these centralized waiting lists in Canada. This analysis may be of interest for other provinces and may provide insight for policy makers across Canada aiming to encourage attachment. Future research using a qualitative approach may help deepen our understanding of the factors influencing attachment of new patients through centralized waiting lists in primary care.
Footnotes
Acknowledgements
We would also like to thank other research team colleague Danièle Roberge and Djamal Berbiche who were of great help at different stages of this research. Finally, we want to thank all the stakeholders involved in the research project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Fonds de recherche du Québec–Santé (FRQ-S Grant #28974). The authors are grateful to the Fonds de Recherche du Québec–Santé (FRQS), which funded Christine Loignon’s young researcher fellowship (J2) and Mélanie Ann Smithman’s and Catherine Lamoureux-Lamarche’s doctoral fellowship, to the CIHR, which funded Mylaine Breton’ Canada Research Chair in Clinical Governance in Primary Health Care and Antoine Boivin’ Canada Research Chair in patient engagement.