
Abstract
Objectives:
High-quality primary care is associated with improved patient experience (PX). Continuity of care is a driver of PX but often relies on complex indices. Whether a simple measure—years of attendance—captures PX remains unclear, especially in free-access systems lacking formal registration such as Japan, South Korea, and Germany. We aimed to investigate the association between “years-of-attendance” and PX, measured by the validated Japanese Person-Centered Primary Care Measure (PCPCM), among adults with a usual source of care (USC).
Methods:
In 2022, we conducted a nationwide, cross-sectional, web survey of Japanese adults (20-74 years). Of 800 respondents (response rate: 71.9%), we analyzed data from the 423 participants who reported having a USC. Exposures were log-transformed years since respondents began visiting their usual institution and physician. The outcome was the mean PCPCM score (11 domains, range: 1-4). Multivariable linear regression adjusted for age, sex, education, household income, self-rated health, number of chronic conditions, type of USC (clinic vs hospital), and rurality. We conducted stratified analyses by type of USC (clinic vs hospital) and rurality (urban vs rural/remote) to assess contextual robustness.
Results:
The median PCPCM was 2.47. Longer continuity showed a positive, dose-responsive association with PCPCM scores. The effect was strongest for physician-level continuity (β = .20, 95% CI: 0.09-0.31, P < .001). Stratified analyses revealed that the continuity-PX gradient was steepest for clinics in urban settings and hospitals in rural or remote settings.
Conclusions:
Among Japanese adults with a USC, longer continuity correlates with better PX. “Years of attendance” works as a practical quality indicator, with interpersonal continuity mattering more than institutional continuity. These findings do not extend to adults without a USC and should be interpreted within this population. Future longitudinal studies are required to inform policies aimed at sustaining continuity.
Introduction
Primary care is widely recognized as the foundation of an effective, efficient, and equitable health system. 1 Robust primary care is linked to better population health and narrower inequities than specialty-focused systems. 2 It is central to achieving the Quintuple Aim of improved health, enhanced patient experience (PX), lower costs, clinician well-being, and equity.3-5 The core functions—accessibility, comprehensiveness, coordination, and continuity—operate synergistically to deliver system-level quality.6-8
This study is set in Japan’s health system, which combines universal coverage with free access, allowing patients to attend clinics and hospital outpatient departments without referral or gatekeeping. Similar “free-access” (or low-barrier) systems exist in countries such as South Korea and Germany, although their insurance and registration structures differ from Japan’s national universal coverage model. Japan lacks formal registration with a named primary care physician; patients instead self-identify a clinic physician or a hospital specialist as their usual doctor, producing heterogeneous patterns of usual source of care (USC) across urban and rural settings.6,7,9 Hospitals often deliver front-line ambulatory care—particularly in rural or remote regions—whereas clinics more commonly provide longitudinal, person-centered care in urban areas.10,11 These structural features may shape how continuity relates to PX by facility type and geography.
We foreground PX because it is both a core quality domain and a proximal mechanism through which primary care influences safety, utilization, equity, and costs.6-8,12 The Person-Centered Primary Care Measure (PCPCM) parsimoniously captures high-value functions (eg, access, coordination, continuity, and comprehensiveness) that mediate downstream outcomes, making PX a theory-consistent outcome for assessing primary care quality.13,14 Across Organization for Economic Co-operation and Development (OECD) countries, PCPCM and related patient-reported measures have been linked to preventive care uptake, avoidable hospitalizations, and health-system performance.13-15 Studies from registration-based systems (eg, the United Kingdom (UK) and Canada) and other OECD settings have reported that having a USC and higher continuity indices are associated with better patient-reported experiences, but these analyses typically rely on claims-based continuity measures or formal patient lists and rarely use the PCPCM.16-23
Among the 4 core functions of primary care, continuity includes interpersonal (relational), longitudinal, informational, and management components. 24 Interpersonal continuity is most proximal to PX because it accumulates tacit knowledge, trust, and coordination efficiency that patients directly experience.24-29 In Japan’s non-registration, free-access context—where both clinics and hospital outpatient departments can function as USCs—variation in relationship duration offers a pragmatic lever to test whether sustained relationships map onto better person-centered care.10,11 In such free-access systems, administrative visit-based indices (eg, the Usual Provider of Care index or Bice-Boxerman Continuity of Care Index) may be unavailable or unstable because patients can attend multiple providers ad libitum.29-32 Patient-reported years since first visiting their usual facility or physician therefore provide a simple, comprehensible continuity indicator continuity that is directly meaningful to patients. Although tenure-based measures sacrifice some comparability with visit-based indices, they capture the lived duration of relationships in non-registration settings such as Japan, South Korea, and Germany. In this study, our physician-level exposure primarily captures interpersonal (relational) continuity, whereas the facility-level exposure also reflects longitudinal continuity at the institution level.
To our knowledge, no prior study has examined tenure-based continuity in relation to a validated, multi-domain PX measure in a nationally distributed sample from a non-registration, free-access health system.13-15 As Japan and other countries debate policies to formalize primary care functions (eg, through primary care function reporting systems and implicit registration), 11 quantifying how simple continuity indicators relate to PX is timely. Therefore, this study aimed to investigate whether, among adults with a USC in Japan, longer duration with the usual facility or physician is associated with higher PX, as measured by PCPCM. We hypothesized that longer duration with the usual facility or physician would be associated with higher PCPCM scores, with the strongest signal for interpersonal (physician-level) continuity, and prespecified stratified analyses by facility type (clinic vs hospital) and rurality.
Methods
We conducted a nationally distributed, cross-sectional web survey (November to December 2022) administered by RJC Research (n.d.), which maintains a profiled panel (≈1.5 million adults) spanning all 47 prefectures with demographic and geographic quotas.6,7,9,33 We followed STROBE guidance (EQUATOR).
Target Population and Analytic Sample
Using sex- and age-stratified random sampling, we invited 1112 adults aged 20 to 74 years (the PCPCM validation range) via automated e-mail from the survey company’s secure platform; investigators had no direct contact with potential participants. 9 Responses were submitted through anonymized online forms, and the research team received de-identified data only. Respondents were first asked, “Do you have a medical facility that you usually visit when ill or for health advice?” Those answering yes (USC = 1; n = 423) proceeded to the PCPCM and comprised the analytic sample for outcome models. Those answering no (USC = 0; n = 377) did not receive PCPCM items and were excluded from outcome analyses, consistent with recommended gating in non-registration systems.8,9 Within the analytic sample (USC = 1), there were no missing data on exposure or outcome.
Exposure: Duration-Based Continuity
Continuity was measured as years since first attending the usual institution and years since first consulting the usual physician, reported by USC = 1 respondents. Relationship duration has been used as a patient-centered proxy for interpersonal continuity with supportive associations to preventive care, utilization, and mortality.29-32 When respondents had more than 1 potential USC, instructions specified the facility used most often for general health problems; ties were resolved by selecting the most recently visited facility. To accommodate 0 years (<1 year) and reduce right-skew, we modeled ln(years+1) (“log1p”) as a continuous predictor, as illustrated in Figure 1.

Distributions of years since starting to visit: (a) a regular medical institution (“Years with regular institution”), (b) natural log-transformed “years with regular institution,” (c) a regular physician (“Years with regular physician”), and (d) natural log-transformed “years with regular physician.”
Outcome: PX
PX was assessed using the validated Japanese PCPCM (11 domains; each 1-4). 9 Consistent with prior PCPCM studies,13,14 the composite score used in analyses was the mean of the 11 items (range: 1-4), not the sum; thus, values in figures and tables represent average item scores. The eleven items cover accessibility, comprehensiveness, integration, coordination, relationship, continuity, advocacy, family and community context, goal-orientation, and health promotion. The continuity item (“My doctor and I have been through a lot together”) does not include relationship length. The Japanese and original versions of all items are provided in Supplemental Tables S1 and S2.
Covariates
Based on prior associations with continuity and PX, we adjusted for age, sex, education, household income, marital status, occupation, self-rated health, multimorbidity (count of 20 chronic conditions), USC type (clinic vs hospital), and rurality using the Rurality Index for Japan (RIJ; 1-100; higher = rural/remote).10,34-37 Age was grouped into 5-year bands to align with sampling strata and reduce functional form misspecification. Multimorbidity was defined as the count of 20 self-reported chronic conditions (eg, hypertension, diabetes, dyslipidemia, chronic lung disease, mental illness), and entered as a categorical covariate (0, 1, and ≥2 conditions) in the main models to reflect overall burden while avoiding over-interpretation of specific disease combinations sharing the same count.
Sample Size Planning
From prior studies we anticipated a USC prevalence of ~55% and a PCPCM standard deviation of ~0.6.9,14,15 Power calculations targeting a small effect for the continuity term (Cohen’s f 2 = 0.02) in multiple regression with ~12 to 14 covariates (α = .05, 1 − β = .80) indicated the need for ≈380 to 420 USC respondents, using the standard sample-size formula for multiple linear regression based on Cohen’s f 2 . Assuming ~70% response and 55% USC prevalence, we issued ≈1100 invitations to reach this target while satisfying the ≥10 observations-per-parameter heuristic.
Statistical Analysis
Categorical variables were summarized as counts and percentages; continuous variables as medians and interquartile ranges. We first fitted multivariable linear regression models of PCPCM on ln(years+1) continuity, separately for institution- and physician-level exposures, adjusting for covariates: age, sex, education, household income, marital status, occupation, self-rated health, multimorbidity, USC type, and RIJ. In the primary specification, multimorbidity was included as a categorical variable (0, 1, and ≥2 conditions). As a sensitivity analysis, we re-estimated all models with multimorbidity entered as a continuous count variable (0-20 conditions) to assess the robustness of continuity estimates to this modelling choice. The PCPCM mean score was treated as a continuous outcome. Model assumptions (linearity, homoscedasticity, normality of residuals) were checked using diagnostic plots, and variance inflation factors (VIFs) were examined (threshold 2.5).38,39 Two-sided P < .05 denoted statistical significance. Analyses used Stata/SE 17.0.
Stratified Analysis
To examine potential effect modification and contextual robustness, we stratified the main models by (a) USC type (clinic vs hospital) and (b) rurality (RIJ 1-20 vs RIJ 21-100, corresponding to urban vs rural/remote). Facility type and geography are known to shape primary care delivery patterns, resource availability, and patient-provider relationships in Japan.10,11
Sensitivity Analyses
Sensitivity analyses addressed potential construct overlap, alternative exposure specifications, nonlinearity, heteroskedasticity and outliers, missing data, and a negative-control outcome. To address potential construct overlap, we recomputed the PCPCM composite after excluding the continuity item (No. 6) and repeated the primary models. Details of all sensitivity-analysis specifications, including categorical exposures, trimming/winsorization, spline modeling, and missing-data handling, are provided in the Supplemental Material. We also repeated all models with multimorbidity entered as a continuous count variable (0-20 chronic conditions) instead of categories; continuity coefficients were very similar, indicating robustness to this modelling choice. Unless otherwise noted, models used heteroskedasticity-consistent covariance estimator type 3 (HC3) robust standard errors.
Ethical Approval and Consent to Participate
The study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Yokohama City University (approval number: F220900057). All participants provided electronic informed consent and were allowed to terminate the survey at any time without penalty.
Results
Of 1112 invitees, 800 completed the survey (response 71.9%); 399 were men (49.8%) and 400 women (50.0%). A USC was reported by 423 respondents (52.9%); this group formed the analytic sample for all PCPCM analyses. Participant characteristics for those with and without a USC are presented separately in Table 1, together with P-values for between-group comparisons. Among USC holders, ≈70% used clinics and ≈30% hospitals as their USC. All VIFs were <2.5, and residual diagnostics did not suggest marked heteroscedasticity, and we reported HC3-robust standard errors.
Participant Characteristics (N = 800).

Abbreviations: RIJ, Rurality Index for Japan; USC, usual source of care.
“Others” indicates respondents who selected the “Other” option because they did not fit the specific categories listed.
The distributions of years since first attending the usual institution and years since first consulting the usual physician peaked around 5 to 10 years, with some relationships extending beyond 40 years (Figure 1). After log transformation, distributions approximated normality. PCPCM scores centered between 2 and 3; the median was 2.47 (interquartile range = 2.00-3.00; Figure 2).

Distribution of PCPCM mean score (average of 11 PCPCM items; each item 1-4, so composite range: 1-4).
In adjusted models restricted to USC holders, longer continuity was associated with higher PCPCM scores at both levels (Tables 2 and 3). The association was strongest for physician-level continuity (β = .20; 95% CI: 0.09-0.31; P < .001), with a smaller but positive association for institution-level continuity. Given the log-transformed exposure, this coefficient implies that, holding covariates constant, increasing continuity with the same physician from 1 to 10 years is associated with an estimated 0.34-point higher PCPCM score on the 1 to 4 scale—approximately half a standard deviation—suggesting a clinically meaningful gradient rather than a trivial effect.
Multivariable Linear Regression of PCPCM Score on Natural Log-transformed Years With a Regular Institution: Overall and Subgroup Analyses (Hospital vs Clinic).
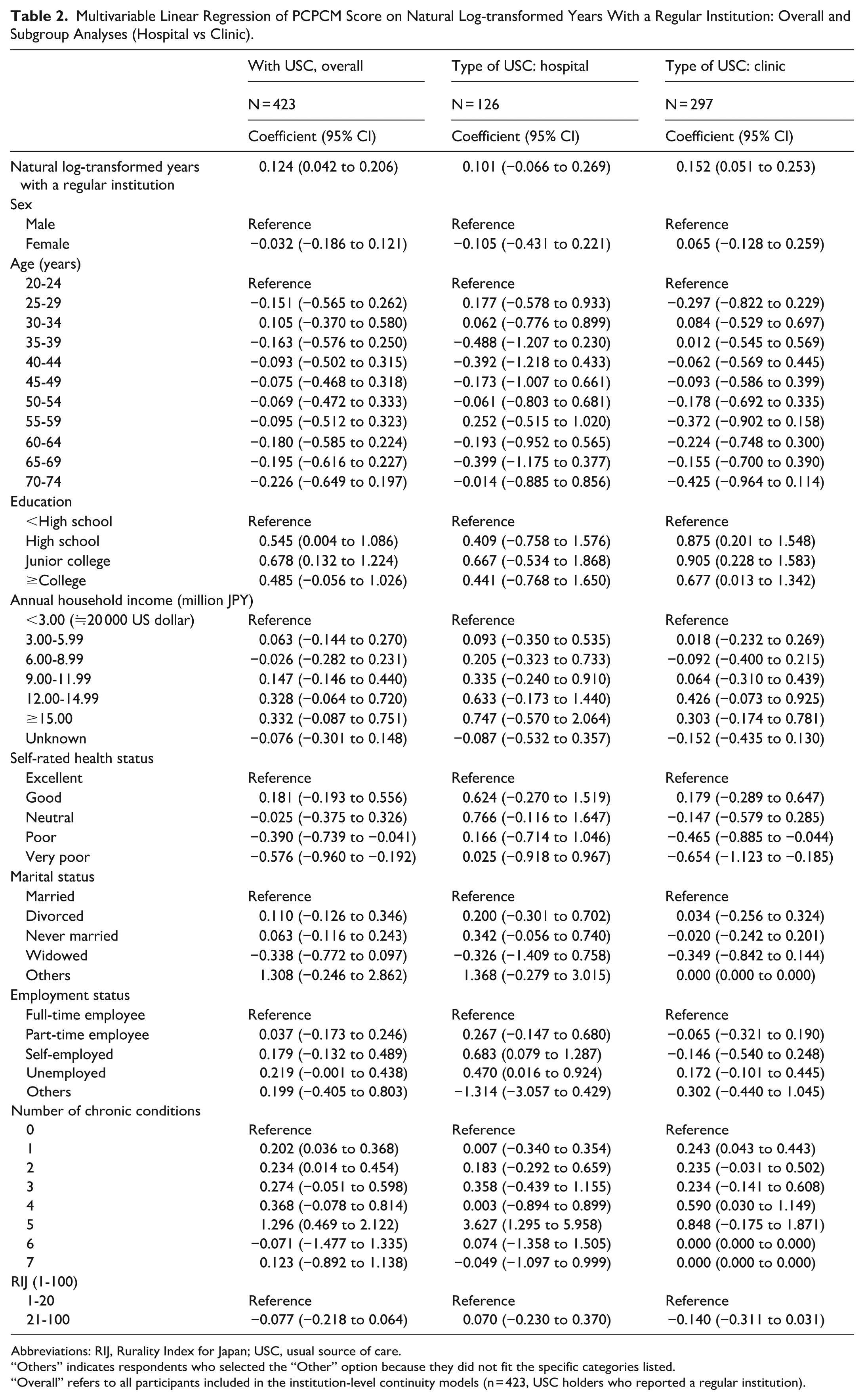
Abbreviations: RIJ, Rurality Index for Japan; USC, usual source of care.
“Others” indicates respondents who selected the “Other” option because they did not fit the specific categories listed.
“Overall” refers to all participants included in the institution-level continuity models (n = 423, USC holders who reported a regular institution).
Multivariable Linear Regression of PCPCM Score on Natural Log-transformed Years With a Regular Physician: Overall and Subgroup Analyses (Hospital vs Clinic).

Abbreviations: RIJ, Rurality Index for Japan; USC, usual source of care.
“Others” indicates respondents who selected the “Other” option because they did not fit the specific categories listed.
“Overall” refers to all participants included in the physician-level continuity models (n = 315, USC holders who reported a usual physician).
Stratified analyses supported context dependence (Figure 3; Table 4). In urban areas (low RIJ), clinic-based continuity showed the steepest gradient, consistent with clinics’ person-centered longitudinal role. In rural/remote areas (high RIJ), hospital-based continuity showed the strongest association, reflecting hospitals’ de facto primary care role in resource-limited regions. “Overall” in Tables 2 to 4 denotes the combined USC analytic sample (USC = 1). Across sensitivity analyses—including recomputation of the PCPCM composite excluding the continuity item (pcpcm_6), alternative exposure specifications, outlier handling, nonlinearity checks, quantile regression, and multiple imputation—the direction and magnitude of the association were consistent. For example, when pcpcm_6 was excluded, coefficients were β = .12 (95% CI: 0.03-0.20) for institution-level and β = .15 (95% CI: 0.05-0.25) for physician-level continuity.

Forest plot of adjusted associations between continuity (natural log-transformed years with a regular institution/physician) and PCPCM mean score.
Crude and Adjusted Coefficients of Natural Log-transformed Years With a Regular Institution/Physician for PCPCM.

Abbreviations: RIJ, Rurality Index for Japan; USC, usual source of care.
P < .05.
However, when we recomputed the PCPCM composite excluding the continuity item (10-item mean), the associations changed little: institution-level continuity β = .12 (95% CI: 0.03-0.20) and physician-level continuity β = .15 (95% CI: 0.05-0.25). These findings suggest that construct overlap does not fully explain the observed gradients, although some inflation of effect sizes remains possible.
Discussion
In a nationally distributed sample of Japanese adults with a USC, a simple continuity indicator—years of attendance—showed a clear, dose-responsive association with better PX as measured by the PCPCM, with effect sizes that are moderate in magnitude and likely meaningful for patients. The pattern held for both institution- and physician-level continuity, with a larger coefficient for physician-level continuity (β = .20) than for institution-level continuity (β = .11), indicating that the association with PX was strongest for interpersonal (physician-level) continuity. This finding aligns with prior evidence that continuity is associated with higher satisfaction, lower utilization, and reduced mortality.16-23 Regarding the magnitude of the association, a coefficient of approximately 0.20 on the 4-point PCPCM scale may appear small numerically. However, in the context of this measure, this effect size is meaningful. For comparison within our sample, the adjusted difference in PCPCM scores between participants reporting “Good” health versus those reporting “Poor” health was of a similar magnitude. This suggests that the “continuity effect” is as impactful on the patient’s experience of quality as their self-rated health status.
Our findings complement existing work showing that higher PCPCM scores are associated with better preventive care, reduced emergency department use, and improved system performance in other countries.13-15 Whereas most prior studies have focused on structural or organizational determinants of PCPCM, our study highlights continuity—measured simply as relationship duration—as an important correlate of person-centered primary care quality in a non-registration system.
Adults who reported a USC were older and had a higher burden of chronic conditions than those without a USC (Table 1), consistent with evidence that people with multimorbidity value continuity more strongly than healthier adults. This selection pattern likely concentrates continuity among those with greater need, which may bias the continuity-PX gradient toward a more positive association within the USC-holding population.
System Context and International Comparison
Regarding the scope and utility of the PCPCM, validation studies in the United States and Canada have established it as a robust measure of high-value primary care functions,13,15 and cross-national analyses across 35 OECD countries have linked national PCPCM scores to health system performance. 14 Our findings suggest that the PCPCM also captures the benefits of continuity in Japan, supporting its use beyond the Western cultural and health system contexts in which it was developed.
In registration systems (eg, the UK), list-based assignment and gatekeeping structurally protect interpersonal continuity, which is associated with fewer ambulatory care-sensitive admissions and lower mortality.20,40 In Canada, administrative data separating physician- from clinic-level continuity show stronger reductions in acute care use for the former. 23 Our results indicate that even without registration, relationship duration tracks higher PCPCM in Japan, implying that policy tools which approximate registration—such as formal designation of a family physician responsible for first-contact care, preventive services, and longitudinal panel management, together with stable provider assignment in clinics and hospital outpatient departments—could enhance PX under free access. 11
In Japan’s free-access system, patients can self-select both clinics and hospital outpatient departments as their USC. This self-selection may encourage those with positive experiences to maintain long-term relationships and affords patients greater autonomy over whom they regard as their usual doctor or facility. However, self-selection is unlikely to operate uniformly across demographic groups: for example, rural residents and individuals with multimorbidity may place greater value on stable relationships and therefore be more likely to identify a USC than healthy urban adults. 41 These structural features of the Japanese system may thus concentrate continuity among higher-need groups and should be considered when interpreting continuity-PX gradients and designing continuity-enhancing policies.
Facility Type and Geography
The continuity-PX gradient differed by facility and rurality: clinics in urban areas and hospitals in rural/remote areas showed the steepest associations. This pattern is consistent with rural populations’ higher valuation of interpersonal relationships 41 and with the reality that regional hospitals often serve as primary contact points in remote areas. In urban settings, clinics typically provide person-centered, longitudinal care with smaller panels and appointment systems, so physician continuity may be easier to maintain and more salient for PX. In contrast, in rural and remote regions of Japan, hospital outpatient departments often function as de facto primary care clinics with limited provider choice; within this context, sustained relationships with hospital-based physicians can play a similar interpersonal role, explaining the strong continuity-PX gradients we observed. These contextual differences argue against one-size-fits-all approaches and suggest facility-specific strategies to bolster continuity.
Interpretation Boundaries and Covariates
Our covariates served to control confounding; we deliberately avoid interpreting their coefficients causally to prevent over-reading adjustment variables as determinants of PX. Estimates for sex, age, income, occupation, and health status should not be over-read. For multimorbidity, we chose a simple categorical specification (0, 1, and ≥2 conditions) because very different disease combinations can share the same count, and the marginal impact of “1 additional condition” is unlikely to be strictly linear. Sensitivity analyses modelling multimorbidity as a continuous count yielded similar continuity estimates, suggesting that our conclusions are not driven by this coding choice.
Conceptual Overlap
The PCPCM includes a domain labeled continuity/relationship, which is conceptually adjacent to our exposure. This raises the possibility of partial construct overlap inflating the association. We therefore caution readers in interpreting the magnitude of effects. However, our sensitivity analysis excluding the continuity item yielded estimates that were substantively similar to the primary results (as detailed in the Results section). These findings suggest that construct overlap does not fully explain the observed gradients, although some inflation of effect sizes remains possible.
Causal Direction and Bidirectionality
Cross-sectional design limits causal inference. Better PX could promote continuity by reducing switching, while continuity could improve PX by enabling accumulated knowledge and coordination. Unmeasured preferences and local supply may shape both. Longitudinal designs with time-varying exposures, or interventional approaches (eg, dedicated attending-physician models or fixed provider assignment), are needed to disentangle directionality.
Implications
Interventions that preserve and extend continuity are expected to support better PX and, according to prior longitudinal and interventional studies, may also contribute to lower utilization and costs.16-23 Given our cross-sectional design, these possibilities should be interpreted as hypotheses for future research rather than causal conclusions. In Japan, strengthening the Family Physician Function Reporting System and piloting stable provider assignment in hospital outpatient departments—especially in rural regions—could operationalize continuity at scale. For clinics, this could include explicitly assigning each patient a regular physician, documenting this in medical records, and aligning appointment systems and after-hours coverage to maintain that relationship. For hospitals, continuity could be supported by small, stable outpatient teams 42 with named lead physicians, structured handovers when staffing changes, and communication to patients about which clinician is responsible for their ongoing care. Telemedicine and panel management may help sustain continuity where workforce is scarce.
Limitations
This study has several limitations. First, as noted above, its cross-sectional design and the potential bidirectionality of the continuity-PX association limit causal inference. Second, because PCPCM items were only administered to respondents who reported a USC, and USC holders differed from non-holders on several sociodemographic and clinical characteristics (Table 1), our analytic sample over-represents individuals who have already established a usual place of care. This likely reflects selective uptake of continuity by people with greater healthcare needs and limits the generalizability of our findings beyond adults with a USC. Third, regarding our sampling method, although we used age- and sex-stratified quotas, our web-based panel is not a probability sample. Relative to face-to-face national surveys, web-based sampling offers rapid recruitment and lower cost but is more vulnerable to selection bias related to internet access and digital literacy. Unlike administrative-data studies, our design captures patient-reported PX but cannot provide population-level estimates. Consequently, we may underrepresent digitally marginalized groups, which could lead to overestimation of continuity and PX among USC holders. Fourth, self-reported relationship duration may be affected by recall error, especially in hospitals with rotating staff. 43 Such error is likely to be nondifferential with respect to PCPCM scores and would therefore tend to attenuate continuity-PX associations rather than create spurious ones; however, some respondents may over-estimate very long relationships, which could modestly inflate effect estimates at the upper end of the duration distribution. Finally, as discussed above, potential conceptual overlap between our continuity exposure and the PCPCM continuity/relationship domain and our use of a simple multimorbidity count (0, 1, and ≥2 conditions) may partially inflate associations, though sensitivity analyses excluding the continuity item and modelling multimorbidity as a continuous count yielded substantively similar estimates. These limitations should be considered when interpreting the magnitude and generalizability of our findings.
Conclusion
Among Japanese adults with a usual physician or institution, longer years of attendance are associated with higher PCPCM-measured PX. The association is strongest for interpersonal physician-level continuity and varies by facility type and rurality, reflecting Japan’s free-access structure. “Years of attendance” is a practical quality indicator that can inform continuity-enhancing strategies in both clinics and hospital outpatient departments. Longitudinal and interventional studies are warranted to establish causality and guide policy.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251413952 – Supplemental material for Association Between Duration of Usual Source of Care and Patient-reported Primary Care Quality in Japan: A Nationwide Cross-sectional Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319251413952 for Association Between Duration of Usual Source of Care and Patient-reported Primary Care Quality in Japan: A Nationwide Cross-sectional Study by Hironori Yamada and Makoto Kaneko in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
Ethical Considerations
The study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Yokohama City University (approval number: F220900057).
Consent to Participate
All participants provided electronic informed consent and were allowed to terminate the survey at any time without penalty.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI, grant number 20 K18847, and a grant from the 2023 to 2024 Research Development Fund of Yokohama City University (grant number not applicable). The study sponsor played no role in the study design, data collection, analysis, interpretation, writing of the report, or decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed in the current study are not publicly available as we did not receive written informed consent for data sharing.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.