
Abstract
Introduction:
Providing self-management education for residents with cardiometabolic conditions in remote islands is a challenge due to the shortage of primary care practitioners (PCPs), specialist physicians, and nurses. Therefore, we applied telenursing with lifestyle-related chronic diseases in remote island residents in Japan. This project aimed to improve the self-management behavior, cardiometabolic indicators, self-efficacy, and quality of life (QoL) of residents with cardiometabolic risks.
Methods:
We chose Ōsakikamijima Island, Hiroshima Prefecture, Japan, which is designated under the Remote Islands Development Act. The project was conducted from 2013 to 2014. The residents aged over 40 and under 75 years old, selected from the annual specific health check-up examination and from PCPs for screening cardiometabolic risks (urinary protein, glycohemoglobin A1c, systolic and diastolic blood pressure (BP), Low-density lipoprotein cholesterol, High-density lipoprotein cholesterol, and triglyceride) were included. The effectiveness of telenursing for self-management education was 6-month-long with a 6-month follow-up and evaluated by a single-group pre-and post-test design. Face-to-face health education was applied at the initial interview followed by telenursing (biweekly telephone calls till third-month, and a monthly telephone call during the fourth and fifth-month) by the trained nurses outside the island. To enhance participants’ self-monitoring health behavior changes, the nurses used motivational interviewing and behavior change techniques based on the transtheoretical model.
Results:
A total of 130 residents, 42 agreed to participate, 41 finished the 6-month program, and 33 completed the 12-month follow-up. Most of their behavior changes like self-management behaviors, cardiometabolic indicators, and self-efficacy at 6-month were improved significantly except QoL. Among the 12-month study periods, self-management behaviors, body mass index, systolic BP, diastolic BP, and self-efficacy (sense of control), (all P < .05) showed significant improvement.
Conclusion:
This study results indicated that telenursing might be effective to improve the lifestyles-related behaviors in chronic diseases on the remote island of Ōsakikamijima, Japan.
Keywords
Introduction
Cardiovascular diseases represent a high prevalence of chronic illness which are related to the decrease in quality of life (QoL), high mortality rate, and high health care costs. 1 Cardiometabolic risk refers to risk factors that increase the likelihood of experiencing vascular events. The relationships among the cardiometabolic risk factors that contribute to the metabolic syndrome like obesity, insulin resistance, atherogenic dyslipidemia, and hypertension. 2 The global prevalence of cardiometabolic syndrome has been increasing over the last 20 years. 3 The cardiometabolic risks may affect individual self-health perception, QoL, productivity, and health care resource consumption. Therefore, primary care providers are best suited to systematically screen patients, identify those at high risk, and intervene to prevent cardiovascular diseases (CVDs).
Studies found that lifestyle modifications and self-management (SM) programs typically confer larger improvements in cardiometabolic risk factors especially for high-risk populations and resource-limited settings.4-6 Self-management is defined as the day-to-day management of chronic conditions by the patient, in collaboration with nurses and other healthcare providers throughout an illness practice where the patient will have to acquire and use to manage effectively. 7 In particular, residents living in remote islands or rural areas have been experiencing challenges regarding access to medical services including nurses, and poorer health outcomes compared to urban residents.8,9 To solve these issues efficiently and effectively, telenursing can help to improve their accessibility of services and health outcomes. With regards, SM education for the lifestyle-related disease is critically important in controlling disease onset and aggravation. Thus, telenursing implementing SM education on a regular basis has the potential to address many of the key challenges to provide health care on the remote island.
Telenursing refers to the use of telecommunications and information technology in the provision of nursing services whenever a large physical distance exists between patient and nurse, or between any number of nurses. 10 Telenursing can increase nurse productivity because it might cover shortages of nurses, reduce time to visit remote areas, 11 and allow patients to remain in their neighborhood or home. 12 Therefore, telenursing SM education has a beneficial effect on nurses and patients.
There are limited reports of interventions that efficiently and effectively change the intensity of telenursing according to the individual risk characteristics of residents at community-based. We have developed various nurse-led disease management programs at community-based and collaborating with primary care physicians.13-16 We assumed by combining this method with telenursing, it was possible to provide support to encourage SM education to prevent the onset and exacerbation of cardiometabolic risks among residents, even in remote islands with limited medical resources.
For this reason, we tried to apply telenursing for the risk of residents with cardiometabolic conditions who live on depopulating, aging, remote islands, as a pilot project in Japan. This project aimed to improve the SM behavior, cardiometabolic indicators, self-efficacy, and QoL of the residents with cardiometabolic risks. This pilot study is significant in working with a local government (national health insurer) to focus on behavior modification of people at risk for cardiometabolic status to prevent aggravation. This framework could be applicable in rural and remote areas that are medically underserved.
Methods
Study Design
As this study was a joint project with Ōsakikamijima, we decided not to have the control group. Therefore, the quasi-experimental (pre-and-post) design was adopted to evaluate the SM education program.
The Description of Ōsakikamijima Island
Ōsakikamijima Island was selected for our research field. It is located in Hiroshima Prefecture, Japan, and has been designated under the Remote Islands Development Act. In 2013 when the research was commenced, the population was 8126 (7320 in 2020) 17 ; 46.1% (47.8% in 2020) of them were aged 65 or over, and 27.2% (28.8% in 2020) were aged 75 or over. The population has decreased by about 47% since 1985. There were 5 primary care clinics with 5 active physicians, and 23 nurses at the clinics, a home-visiting nursing station, and a nursing home. They were mostly 50 years and over, and no new healthcare providers have been moved in even until 2020. In addition, there were no specialists and nurses specialized in chronic care management. Since medical treatment was not performed at nighttime and on holidays, residents in an emergency must be transported to medical institutions on the mainland by helicopter or boat, which occurred 276 times in 2013.
When this study began, the prevalence of hypertension, chronic renal failure with dialysis per population was high among residents aged 40 and over. In addition, more than 60% of the residents aged 60 and over had lifestyle-related diseases and were being treated for them. 18
Development of the SM Education System
The system of telenursing for SM education was developed by clinical nurse specialists in chronic care nursing, a public health nurse (PHN), and primary care physicians (PCPs) of Ōsakikamijima. The telenursing center providing SM education was placed at Hiroshima University for a pilot trial. We set 2 ways of targeting residents. Since the Japanese government started the “Specific Health Checkups” annual metabolic screening examination by municipal governments (which is the National Health Insurer, covering eligible individuals, that is, those aged over 40 and under 75) in 2008, one target was the metabolic-syndrome population, and the other targets included the population with lifestyle-related chronic diseases referred from PCPs. At the telenursing center, the nurses provided the SM program, monitored self-monitoring data (including BP, weight, and behavioral changes), connected participants to PCPs and specialists, and evaluated the outcomes.
Description of the SM Education Program
The project was conducted from 2013 to 2014. The telenursing SM education provided in this system followed the steps shown in Figure 1. The program was designed for the target population to acquire SM skills and control their health risk factors based on our previous disease management programs, which showed significant effectiveness.13,14
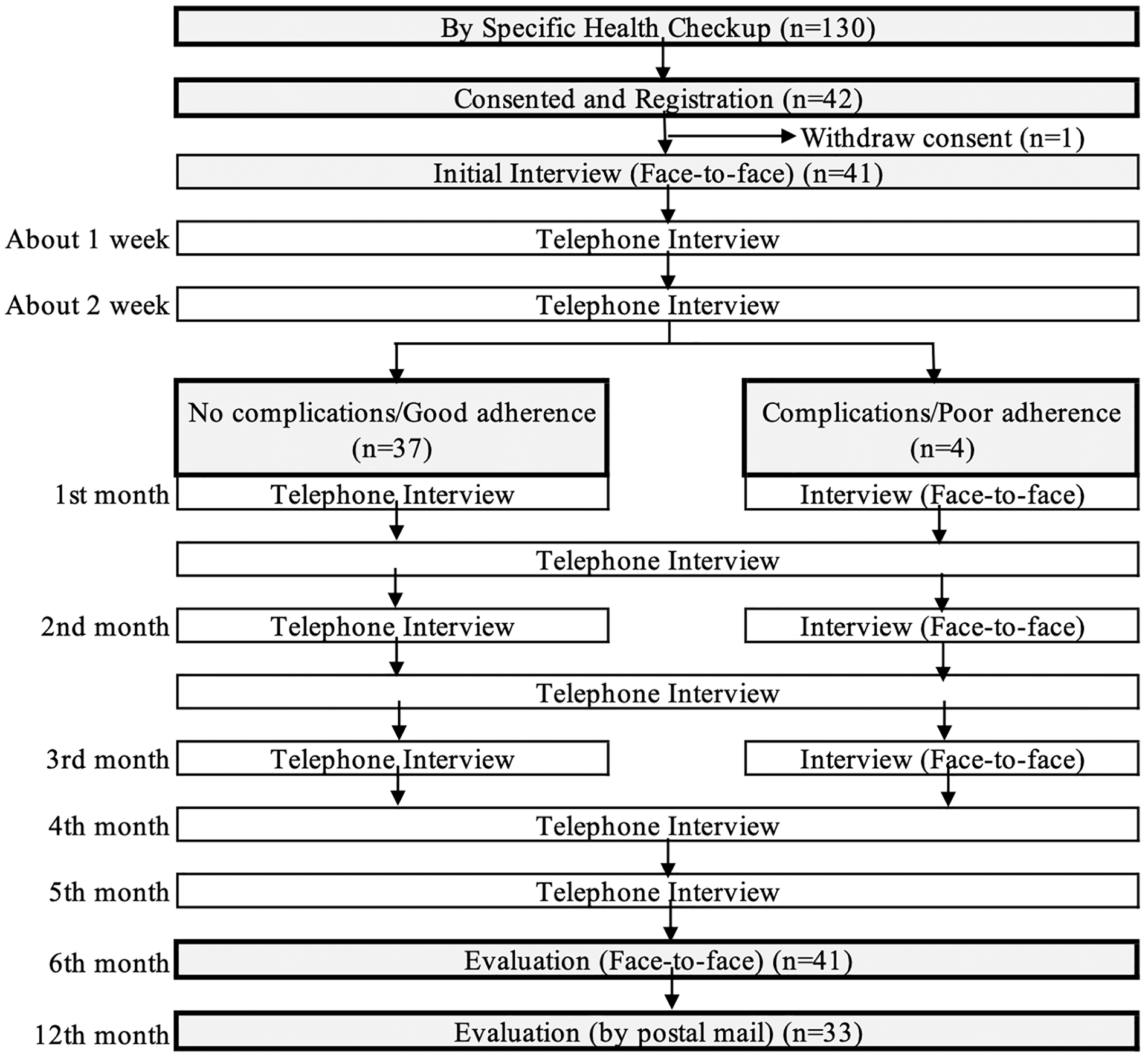
Study procedure and participants’ flow of this study.
The behavioral modification requires at least 6 months of implementation based on the transtheoretical model 19 ; therefore, we set the duration at 6 months. Education was provided mainly by telenursing. To establish trust and a holistic assessment including lifestyle, diet, physical and mental examination, family, and environment, we decided on conducting face-to-face sessions for better compliance. At the initial session, the participants and nurses discussed and decided on an individual long-term goal (purpose of life), and short-term goals (6-month goal), and action plans for the following month such as diet and exercise based on their individual daily practices. The nurses evaluated their behavioral stages of change, self-monitoring data, and laboratory test data, and added SM education using the telephone.
The basic intervention was a biweekly telephone call until the third month and a monthly telephone call during the fourth and fifth months. Face-to-face education sessions on the second and third months were set for participants with complications and poor adherence. For the final evaluation, we set a face-to-face interview when the program ended. At the initial session, participants were provided with a researcher-made educational booklet, and a daily self-recording and referral notebook.
Regarding communication skills, preparation levels of behavioral change were carried out in stages in reference to the transtheoretical model. 19 The nurses used the motivational interviewing 20 and behavior change 21 techniques based on participants’ psychological stages: (1) pre-contemplation; (2) contemplation; (3) preparation; (4) action; and (5) maintenance of items related to diet, exercise, alcohol consumption, and smoking (Supplemental Table S1).
Study Participants
The participants were residents of Ōsakikamijima who met the criteria. The inclusion criteria were: residents aged over 40 and under 75 years, who received abnormal values on a specific health check-up examination in the 2013 fiscal year, and laboratory testing by PCPs. Those were: (1) urinary protein 2+ and over; (2) glycohemoglobin A1c (HbA1c) of ≥ 6.5%; (3) systolic blood pressure (SBP) of ≥160 mmHg or diastolic blood pressure (DBP) of ≥100 mm Hg; (4) Low-density lipoprotein cholesterol (LDL-C) ≥140 mg/dl, High-density lipoprotein cholesterol (HDL-C) <40 mg/dl, or triglyceride (TG) ≥200 mg/dl. These were decided with the PHN and PCHs, and based on the health check-up guideline. 22 Residents were targeted from (1) to (4) order since many of them had multiple comorbidities. The exclusion criteria were residents who were hospitalized at the time of registration and were unfit because of cognitively impaired or severe physical conditions (judged by PCPs).
Recruitment and Registration
The PHN who belonged to the health division selected eligible residents, then the PHN contacted and received informed consent from the residents. Subsequently, the nurses contacted the participants by an initial home visit and received the order sheets from the PCPs sharing the treatment goals, and PCPs began using a specialist reference system. If the participants had no history of clinic visits regarding the risks, the nurses recommended them to visit PCPs. After the nurses confirmed that they had visited the PCPs, the nurses began the program.
Outcomes of the Project
The hypothetical process of the outcomes emerging was: after nurses’ education based on psychological preparation,
23
participants’ psychological stages progressed, their behavior changed, and their self-efficacy and physiological parameters improved (weight, body mass index [BMI], SBP, DBP, HDL-C and LDL-C, TG, fasting blood glucose [FBS], HbA1c, aspartate transaminase [AST], alanine transaminase [ALT], gamma-glutamyl transferase [γGT], and estimated glomerular filtration rate [eGFR]). Self-efficacy
24
and QoL (the QoL
Data Analysis
Descriptive statistics as frequencies and percentages were used to summarize categorical measures. After confirming the distribution, paired t-test, one-way ANOVA, Wilcoxon signed-rank test, and Friedman’s test were performed from baseline, 6-month, and 12-month follow-ups. For statistical analysis, Statistical Package for the Social Sciences (SPSS) for Windows version 25.0 was used, and the significance level was set at <.05.
Results
Of all 130 residents who met the eligible criteria, 42 participants agreed to participate in the study (consent rate, 32.3%). Most of the residents who did not consent said they did not feel necessary because they were already in consultation with physicians and busy. Of these 42, one dropped out right after giving consent because of chemotherapy, and 41 began and completed the 6-month program. As another 6-month follow-up, 33 of 41 participants were traceable at 12-month by postal mail (Figure 1).
Regarding modification of intervention, 4 participants were unaware that their renal function had declined at the time of the first interview and had more time to comprehend and acknowledge the disease condition before SM education that did not worsen renal function. Thus, the nurses exchanged the subsequent 3 telephone interviews to face-to-face instruction and provided information so that they could understand their physical condition and comprehend the significance of behavior change. Additionally, we discussed self-management behavior regarding dietary goals and motivated them to maintain a healthy diet (eg, reduce salt intake, reduce the amount of fatty and oily foods, maintain total energy intake and nutritional balance).
Table 1 showed the baseline characteristics of the participants (n = 41 and n = 33). The majority of the participants were male. At baseline, the largest age group was 60 to 69 years old. Among them, 85% of participants lived with other family members, about 71% did not work. Participants with HbA1c ≥6.5% was 26.8%, BP ≥160, or ≥110 mmHg was about 30%, and hyperlipidemia was 46.3%.
Outline of the Participants at Baseline.

Figure 2 shows the behavior stages at baseline (n = 41) in the number of participants and change for 6 months with statistical significance. In terms of the changing stages of diet and exercise, the number of participants in the “maintain stage” or “action stage” increased significantly (P < .001). Furthermore, the frequency of action is different (n = 33). As for the frequency of BP and weight measurements, dietary, and exercise target behaviors, the participants in the “maintain stage” or “action stage” improved significantly (P < .01) (Table 2). Regarding dietary target behavior, the participants who carried out 4 or more days a week increased from 24.2% at the baseline to 69.7% after 12 months of follow-up. Drinking frequency and alcohol consumption decreased, although there were no statistically significant differences. There was no change in smoking before and after the intervention program.
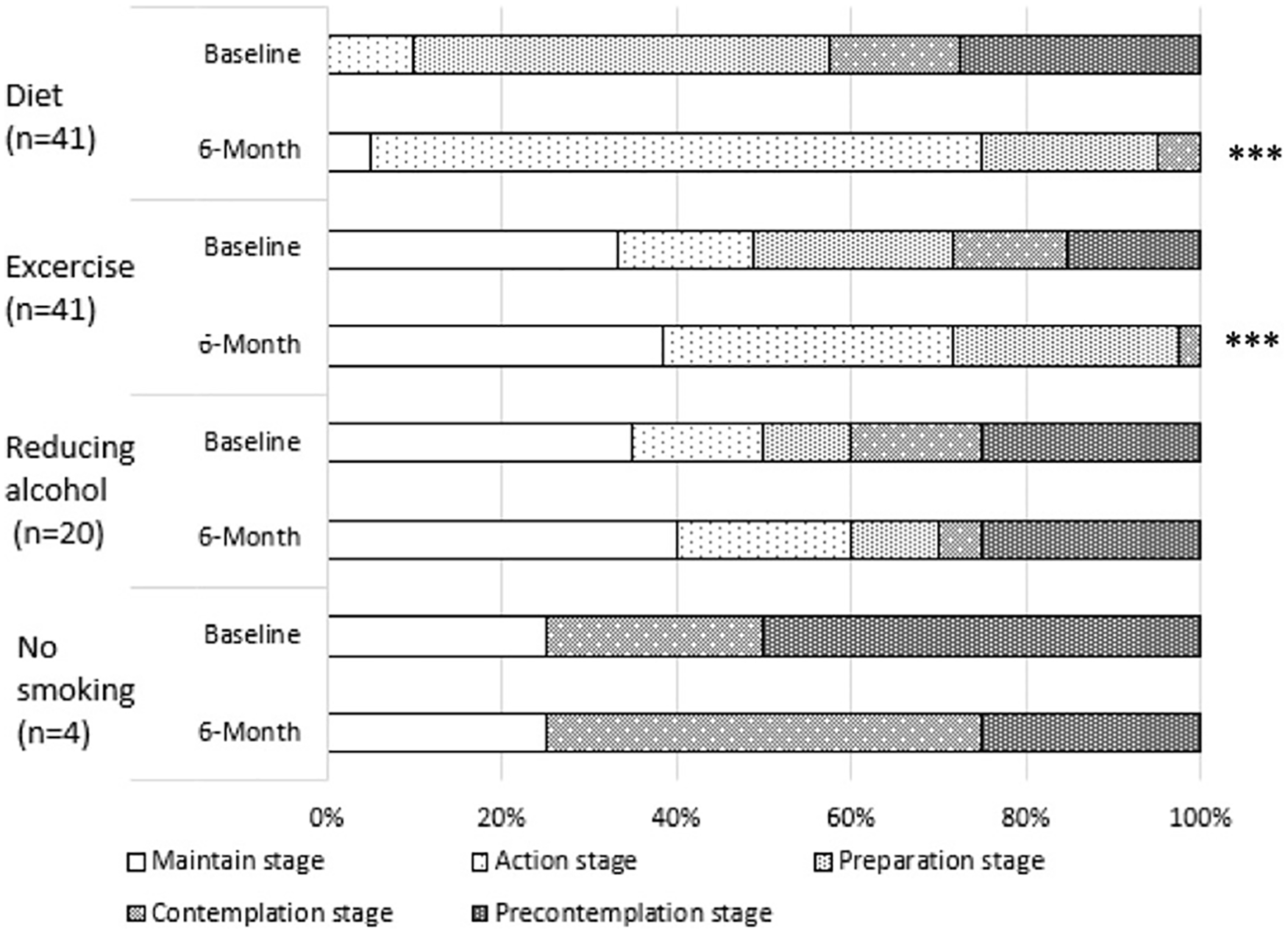
Proportion of participants with self-management behavioral stage changes at baseline and 6-month.
Differences in Number of Participants in Self-Management Behaviors at Baseline, 6-Month and 12-Month Follow-Ups.
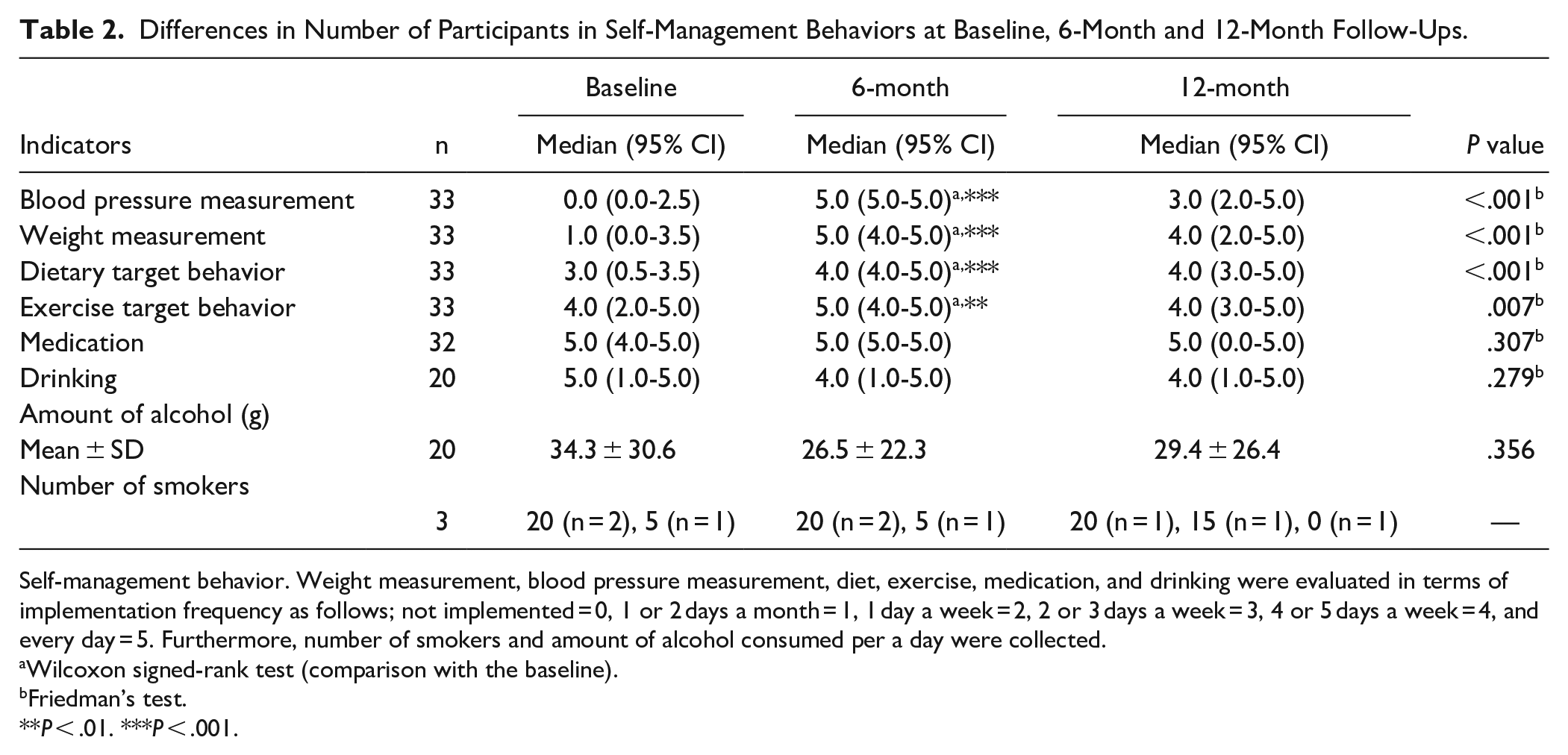
Self-management behavior. Weight measurement, blood pressure measurement, diet, exercise, medication, and drinking were evaluated in terms of implementation frequency as follows; not implemented = 0, 1 or 2 days a month = 1, 1 day a week = 2, 2 or 3 days a week = 3, 4 or 5 days a week = 4, and every day = 5. Furthermore, number of smokers and amount of alcohol consumed per a day were collected.
Wilcoxon signed-rank test (comparison with the baseline).
Friedman’s test.
P < .01. ***P < .001.
Table 3 (n = 33) shows that there were significant improvements in BMI, SBP, DBP, HLD-C, LDL-C, HbA1c, and FBS (P < .05), and maintained eGFR at 6-month evaluation. Significant improvement continued until 12-month follow-ups regarding BMI, SBP, and DBP (P ≤ .001).
Cardiometabolic Indicators at Baseline, 6-Month and12-Month Follow-Ups.

Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FBS, fasting blood glucose; HbA1c, glycohemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure.
Mean ± SD.
Paired t-test (comparison with the baseline).
ANOVA.
Friedman’s test.
P < .01. ***P < .001.
Table 4 (n = 32) shows that self-efficacy scores increased according to an improvement in self-management behaviors at 6 months, then decreased afterward. However, the QoL, physical summary, and mental summary scores did not change (P > .05).
The Difference Psychosocial Indicators Measurement from Baseline, 6-Month and 12-Month Follow-Ups.

Mean ± SD.
At 6-month, *P < .05.
Paired t-test (comparison with the baseline).
ANOVA.
Self-efficacy measurement. Self-efficacy was measured for health behavior of chronic disease patients. This measurement (self-efficacy) developed by Kim et al 24 and capable of making desirable health behavior in the course of treating disease. It is composed of the subscale of “aggressiveness of coping behavior in disease” and “sense of control over health.” The reliability and validity of this scale have been confirmed.
QoL measurement. The QoL was measured using QoL-SF-8TM Standard Edition (Fukuhara et al). 25 SF-36 (Medical Outcomes Study 36-item short form) is the most widely used health-related quality of life scale internationally. SF-8 is a scale that can calculate the estimated value of SF-36 with fewer items. This tool measured 8 concepts on health (subscale). Because of the comprehensive scale, health-related QoL of various diseases can be measured, and it can be compared with patients with different diseases. Reliability and validity of this scale have been confirmed.
P < .05.
Discussion
Our study results showed that SM education through telenursing in Ōsakikamijima Island improved the physiological health parameters and lifestyle-related behaviors of participants. In particular, improvements in obesity, BP, lipids, and glucose metabolism have improved cardiometabolic risk factors. In cardiometabolic diseases like hypertension, diabetes, lifestyle choices can exert a substantial effect on the course of the underlying disease. It is therefore essential that the nurse maintains a close relationship with the patient and acts as a source of ongoing support. 27 Telenursing facilitates this relationship and can broaden the scope of nursing services available to patients at home.28-30
Lifestyle-related chronic diseases such as heart disease, stroke, renal failure, diabetes, etc., can be prevented from onset and aggravation by disease management. Cardiometabolic diseases occupy the top ranks among the diseases that require high medical expenses and long-term care. Thus, given the importance of time, cost, and accessibility in determining whether patients pursue and sustain the care of chronic conditions like hypertension, 31 diabetes, 32 telenursing offers promising benefits in this regard. Consequently, this program may contribute to the most cost-effective and efficient implementation of SM educational methods in cardiometabolic diseases.
Studies reported that telemonitoring resulted in reduced use of socio-health resources 33 and reduced mortality (by 24%), readmissions (by 28%) in patients with heart failure, 16 and decreased visits to emergency services, also increased contact with primary care, and patient satisfaction as well as improved their QoL.16,33
The method of identifying risk factors at the first session, evaluating their psychological readiness, and strengthening SM behavior had a positive effect on their behavioral changes. We believe that nurse’s approach according to psychological preparation and motivation interviewing were effective in alleviating the patient’s resistance and improving engagement. Besides, improvements in physiological indicators could be due to daily monitoring at home through telenursing and regular feedback from nurses. Research showed that using telenursing, patients require continuous monitoring of their abilities to cope with their illnesses and learn how to change their lifestyles. 34 In this program, nurses strengthened communication between participants and their PCPs by showing their self-monitoring data to their PCPs and encouraging them to consult about their physical condition management. We believe that this approach prompted positive feedback from PCPs regarding participants’ behavioral changes, the reflection of self-monitoring data in treatment, improved participant’s self-efficacy, and promoted further behavioral changes.
Furthermore, in this study, some participants were not able to accurately understand their own renal dysfunction, but strengthened intervention, and provided specific education, resulting in behavior changes. This led to an improvement in physical indicators. In SM education on remote islands where there is a shortage of healthcare resources, there is a great demand for professional nurses using telenursing.
With regards, it was recognized that collaboration between PCPs and nurses in implementing telenursing was very important in the case of SM education. In this project, we developed SM education and Ōsakikamijima municipal government outsourced telenursing services, connected PCPs and specialists. If SM education is conducted throughout the region, one limitation can be the shortage of specially trained nurses. These results were similar to previous studies where nurses found difficulties in applying telehealth due to lack of personnel, including advanced-practice nurses. 35 It is considered that SM education with telenursing can be applied to remote islands by taking into account the characteristics of the remoteness of the area and the problems of chronic diseases that exist.
Limitation
The limitations of this project were the small sample size and it’s maybe due to most eligible residents were not interested to participate as they had periodic clinic consultations, shorter periods of implementation, and selection bias.
However, as this project was introduced to our government and become one of the nation-wide projects, therefore, larger sample results will be reported in the near future. Moreover, this was the first project providing SM education through telenursing to the remote islands in Japan. So, inside Japan, where the services are unevenly distributed like remote islands and mountainous areas, is considered to develop the SM education effectively by telenursing that flexibly responds to the risk of the residents, which was demonstrated in this study.
Conclusion
In Japan, with the aging of society, the importance of continuous nursing care for chronically ill patients keeps increasing. Against this background, as a pilot study, telenursing shows the promise in providing SM education on remote islands as well as an important means of nursing care in the future. The system helped the residents to acquire SM behaviors and to improve their physiological outcomes. This program could help to promote primary care and health in the maintenance process and to enhance prevention.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211030817 – Supplemental material for The Effectiveness of Telenursing for Self-Management Education on Cardiometabolic Conditions: A Pilot Project on a Remote Island of Ōsakikamijima, Japan
Supplemental material, sj-docx-1-jpc-10.1177_21501327211030817 for The Effectiveness of Telenursing for Self-Management Education on Cardiometabolic Conditions: A Pilot Project on a Remote Island of Ōsakikamijima, Japan by Michiko Moriyama, Kana Kazawa, Yasmin Jahan, Mika Ikeda, Mariko Mizukawa, Yasuko Fukuoka, Koji Harada and Md Moshiur Rahman in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to express our deepest gratitude to the municipal government, primary care physicians, and residents of Ōsakikamijima who collaborated and supported this project. We are also indebted to Ms. Rie Maeda and the disease management nurses for their contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by JSPS KAKENHI, Grant Number JP 24659988.
Ethical Approval
Approval for this project was obtained from the Epidemiological Ethics Committee of Hiroshima University, Japan (the approval number: Eki-848). All participants gave written informed consent for their participation, and the study was performed according to the Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.