
Abstract
Introduction/Objectives
Project ECHO COVID-19 was launched nationwide on March 4, 2020 to disseminate guidance about COVID-19 in a timely and scalable manner to meet the urgent needs of primary care settings, the first line of defense in a pandemic.
Methods
Data from post-session surveys were analyzed to assess participant satisfaction, knowledge gaps, change in knowledge, and anticipated changes in practice as a result of Project ECHO COVID-19. A content analysis was conducted of the 243 questions and concerns posted by over 2000 participants in the Question and Answer function of Zoom during the first 8 sessions (March 4-April 29, 2020).
Results
Of 5243 registrants, 49% attended at least one session. Respondents agreed or strongly agreed that didactic sessions (97%) and case presentations (96%) met their learning needs; 93% reported gaining new knowledge, and 88% would implement that knowledge. Only 32% and 53% of respondents anticipated changing workflows and adapting to telehealth, respectively, despite the need for both as the pandemic continued. The content analysis identified 3 categories: clinical operations (eg, testing, triage, telehealth, billing); patient care (diagnosis and treatment of COVID-19, management of high-risk vulnerable populations); and epidemiology (viral spread, implications for public health).
Conclusions
Care of vulnerable populations and clinical operations should be addressed when planning education and clinical interventions for public health crises. Adapting the Project ECHO model to be more scalable was an effective means of creating a community of practice among health professionals when evidence-based guidance was not available to manage the implications of a pandemic.
Introduction
When the World Health Organization (WHO) described the coronavirus disease 2019 (COVID-19) outbreak as a public health emergency of international concern on January 30, 2020, 1 there were no guidelines for prevention, diagnosis, treatment, testing, or how to minimize exposure to staff while maintaining high quality patient care. 2 As a nationwide shut down loomed, the immediate need for evidence-based guidance was urgent in primary care settings, deemed the “first line of defense” in a pandemic. 3 Keeping primary care sites operational during a pandemic is of critical importance, 4 yet some were forced to close or cut back on services.
Dissemination of guidance about COVID-19 needed to be rapid, timely, and scalable, and needed to take advantage of e-learning platforms, as recommended by a 2019 United Nations conference on pandemic preparedness. 5 Project Extension for Community Healthcare Outcomes (ECHO) was well-suited to respond to the needs of the moment. Project ECHO is an evidence-based telehealth intervention developed at the University of New Mexico to improve management of hepatitis C by primary care providers in rural areas.6,7 Project ECHO uses didactic presentations by expert faculty, case-based learning, and guided practice to enhance the capacity of health care professionals to better manage challenging conditions in their patients. Participation in a Project ECHO has improved provider knowledge and self-efficacy, as well as outcomes in patients with HIV, 8 chronic pain,9,10 and substance use disorder, 11 and children with behavioral health disorders. 12 These outcomes have been shown across a variety of settings, including major medical centers, small healthcare systems, and safety-net settings.
This paper evaluates the first 8 sessions of a Project ECHO COVID-19 series that occurred in March and April 2020. (The series continued to be offered as the crisis evolved more than a year later.) Although it was hosted by a large Federally Qualified Health Center (FQHC) with deep experience in this telehealth intervention, primarily with safety-net primary care clinicians, launching the series as the pandemic unfolded was fraught with unknowns. Information about the virus, its prevention, detection, and treatment seemed to change every day, requiring the curriculum to evolve as new information and questions emerged. Recruitment efforts cast a wide net with a goal to disseminate credible information to as many people in the health sector as possible as quickly as possible, and for as long as necessary. This paper aims to: (1) provide a snapshot in time of the needs and concerns of health care professionals across the United States during the onset of the COVID-19 pandemic; (2) provide evidence that adaptations of the Project ECHO model can be effective for disseminating guidance to primary care workers during a public health crisis; and (3) provide recommendations on how to better prepare primary care settings, especially those serving vulnerable populations, for public health emergencies in the future.
Methods
Setting
The Weitzman Institute (WI), founded in 2007, is embedded within the Community Health Center, Inc. (CHCI) in Connecticut, which provides comprehensive medical, behavioral health, dental, and nursing care to 105, 000 patients. In 2012, CHCI/WI was the first FQHC in the country to replicate Project ECHO to help promote coordinated, evidence-based care for chronic conditions commonly seen and managed by providers in safety net primary care. As of March 2020, WI had over 12 active programs on a variety of chronic and complex conditions, and over 2000 primary care providers and care team members from 47 states, Washington, DC, and Puerto Rico had participated in ECHO programs.
Recruitment of Participants
Recruitment strategies included eBlasts to the CHCI master list of over 47, 975 contacts, including staff from community health centers and state Primary Care Associations. There was group outreach to over 700 participants who were enrolled in any WI Project ECHO series at the time and personal outreach via email to partners, including the National Association of Community Health Centers (NACHC). The series was also posted on the CHCI and WI websites.
Description of Intervention
Planning for Project ECHO COVID-19 began on February 27, 2020, with the first session on March 4, and with the initial 8 sessions occurring March 4 to April 29, 2020.
To anticipate learner needs before launch, WI reached out to Community Health Best Practices, LLC, a nonprofit network comprised of 16 of the nation’s leading community health centers, including CHCI, to learn from others’ experiences. As the series continued, cases, presentations, and didactic topics were chosen based on emerging information from government agencies, researchers, and leading medical experts. Additionally, participant post-session comments were reviewed weekly to identify participant needs, which informed content development. Topics included, but were not limited to: epidemiology and clinical presentations of COVID-19; triage, including a nurse interview guide; COVID testing and inventory policies; telehealth strategies; caring for vulnerable populations; crisis counseling and self-care; vaccine development.
Each ECHO session lasted 60 minutes, including a 20-minute didactic presentation by expert faculty, an update on the status of COVID-19 in the United States, and a discussion of cases, questions, and answers. Whereas previous Project ECHOs allowed for verbal interactions between faculty and participants in real time, the size of the audience for Project ECHO COVID-19 required that faculty engage with participants through Question/Answer and Chat functions. Recurring faculty for all 8 sessions included clinicians from CHCI: Director of the Weitzman Institute, who is a physician; Chief Medical Officer; Chief Nursing Officer; and Chief Behavioral Health Officer, a clinical psychologist. External faculty included an infectious disease physician from MidState Medical Center in Connecticut; an epidemiologist and vaccinologist, who is Director of the Yale Institute for Global Health; and Chief Medical Officer of Northeast Emergency Medicine Specialists, whose expertise was in the roll-out of COVID-19 testing across the region.
Study of the Intervention
Evaluation methods included analysis of registration forms, attendance reports, post-session surveys, and entries in the Question/Answer function. Prior to attending a session on COVID-19 ECHO, participants completed a registration form asking for their contact information, role type, and organization type. Attendance reports were pulled from the zoom videoconference platform after each session. These attendance reports include all self-identified data from our registration form and were used to conduct analysis on the participants of each session.
Post-session surveys addressed implementation outcomes rated on Likert scales: satisfaction with the didactic and case presentations; self-reported changes in knowledge; and likelihood to implement this knowledge. Also, participants were asked what changes, from a list of 9 possibilities, they would make in their practice as a result of attending the session. Lastly, responses collected from an open-ended comments field in the post session survey yielded 118 responses, which were categorized simply as “feedback about session” or “suggestions for future sessions” by 2 of the authors.
Entries into the Question/Answer function were transcribed, yielding 243 discrete units of data for a content analysis. [Entries into the Chat function were not used because not all entries were retrievable.] Two researchers analyzed these data using a text-driven deductive approach to content analysis,13,14 discussing the assignment of data to the categories until there was mutual agreement.
This study was approved by the Community Health Center, Inc. Institutional Review Board.
Results
Of the 5243 individuals from all 50 states plus Guam, Puerto Rico, and the District of Columbia who registered for at least one Project ECHO COVID-19 session, 2560 (49%) attended at least one or more of the initial 8 sessions. Although our target audience had traditionally been primary care providers in the 14, 000 safety-net primary care sites, including 1368 FQHCs, only 40% of participants were from FQHCs or look-alike community health centers. To our surprise, 60% included hospital systems, government agencies, universities, and community-based organizations nationwide. Of the 2650 participants, approximately 33% attended at least 2 of the 8 sessions. The range for attendance was 332 to 1007 per session, with an average of 655 attendees. There were a total of 454 responses to the post-session surveys ranging from 34 to 98 per session, with an average of 57 responses per session.
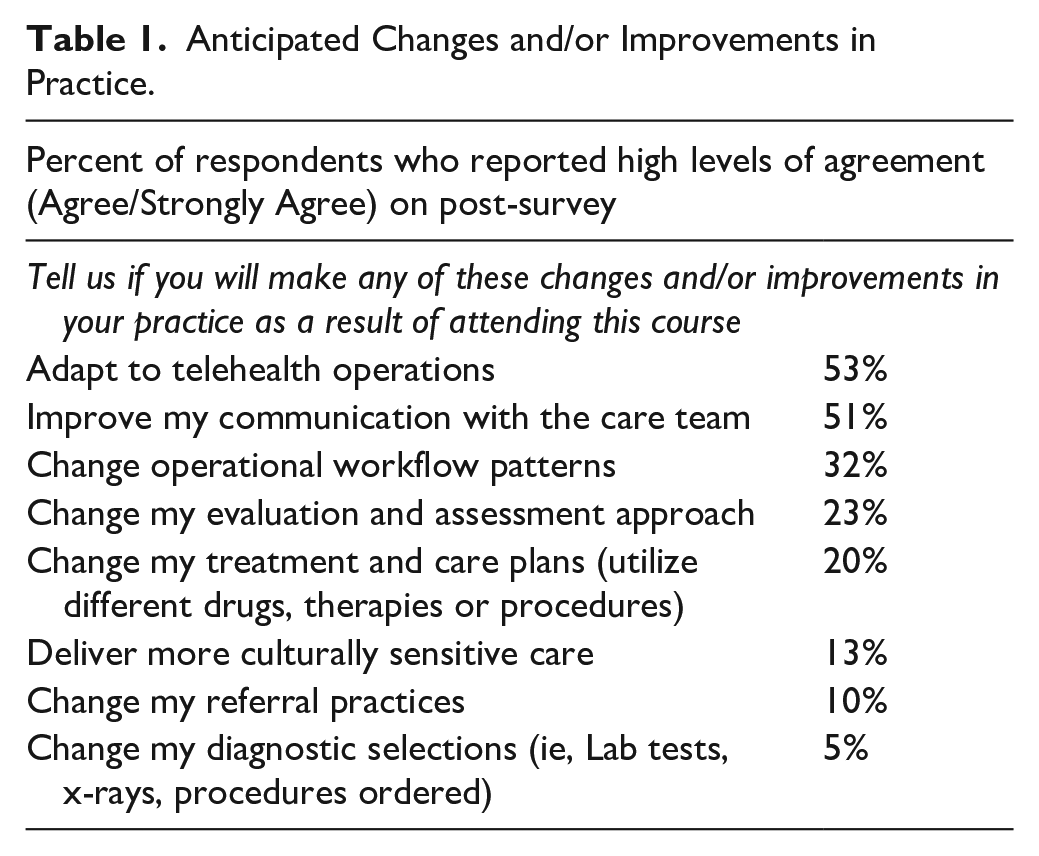
Respondents overwhelmingly agreed or strongly agreed that the didactic sessions (97%) and case presentations (96%) met their learning needs. On average 93% to 94% of respondents reported gaining new knowledge, and another 88% reported that they would implement what they had learned. When asked what practice changes they would make as a result of attending Project ECHO COVID-19, 53% would adapt to telehealth, 51% would improve communication with staff, and 32% would change workflow. The responses reported in Table 1 were made at the end of April 2020, just as these changes became necessary. Of the 118 comments in the post-session surveys, 62% were “feedback about session,” all of which were positive comments about the timeliness and excellence of the presentations and faculty: “one of the best informational webinars I have been on. . .. very helpful to have medical, nursing, behavioral health input. . .Dr. X was excellent. . . Very important and up-to-date information.” The remaining 48% of comments addressed “suggestions for future sessions,” most of which were incorporated in the curriculum, as noted earlier.
Anticipated Changes and/or Improvements in Practice.
Content Analysis
The content analysis of the 243 entries into the Question/Answer function was guided by 2 questions: What do participants need help with? What are they concerned about? The entries were broken down into 3 broad categories: operations, patient care, and epidemiology/policy. Examples of the categories and themes within them are in Table 2.
Content Analysis of Participants’ Questions and Concerns.

Operations (n = 122)
In the initial ECHO sessions in March 2020, participants had questions about changes in day-to-day operations needed to ensure safety of patients and personnel. These included: disinfecting workspaces and equipment; appropriate use—or re-use—of personal protective equipment (PPE) given low supplies; and staff safety during in-person encounters with patients. By April 2020, operational issues turned to the logistics of in-person testing, phone triage, and telehealth workflow and billing codes. Telehealth presented challenges with staffing and patients unfamiliar with technology.
Patient care (n = 84)
Early in the pandemic in March 2020, participants’ greatest concern was how to find a balance between caring for individual patients and public health concerns. If patients quarantined at home, there was no way to assess for severity of illness or to test them, and thus no confirmation of a COVID-19 diagnosis. But primary care providers were hesitant about sending all but the sickest patients (eg, high fever) to urgent and emergency care centers, which were overcrowded and where risk of exposure was increased. Mitigating risk for COVID-19 among those with complex health conditions, such as diabetes, asthma, and compromised immunity, as well as treating these patients should they become symptomatic, generated much discussion, especially in light of the promotion in the media of COVID-19 therapeutics—unproven and otherwise. There were questions about special populations: children, pregnant women, the homeless, and behavioral health patients, especially those receiving medication assisted treatment (MAT) for opioid dependence, which requires face-to-face visits.
Epidemiology and policy (n = 37)
The first questions asked by participants in March 2020 addressed how the coronavirus spread—for example, airborne droplets and on surfaces—and how easily it spread. Virus spread had implications for restrictions on personal behavior—travel, exercise, gathering in groups indoors and outside—and if the virus would be less virulent in warmer weather conditions. Information—and misinformation—about immunity and vaccines were also discussed. Finally, there was confusion about the role of government, such as local health departments, the Centers for Disease Control (CDC), and OSHA (Occupational Safety and Health Administration).
Discussion
Our findings are a snapshot in time of the preparedness of primary care settings and other organizations to deal with the novel coronavirus just before the nationwide shutdown in March and through the early weeks of the pandemic in April, 2020. As expected, participants asked questions about infection control, staff safety/PPE, and disease identification, treatment, and management, consistent with the information needs anticipated by the United Nations conference on pandemic preparedness and by the Centers for Disease Control pandemic response plan.4,5 However, those guidelines did not and could not prepare participants for the realities of the COVID-19 pandemic.
Of significant concern were vulnerable populations at disproportionately high risk for developing and dying from COVID-19 including: individuals with chronic health conditions, individuals in key populations (eg, the homeless), and individuals whose lives exposed them to high exposure risk situations such as employment in low-income essential jobs with high contact with the public, crowded or unstable housing conditions, and reliance on public transportation. While many of these “high-touch, high risk” patients are served by safety-net settings, 2 vulnerable populations also are found in private practices and practices affiliated with health systems.3,15 Regardless of setting, primary care has been encouraged to identify and account for the effects of exposure to high risk social and economic circumstances in vulnerable populations in order to better identify barriers to and facilitators of better clinical outcomes.16-18
Indeed, defining “at risk” patients has been identified as a component of future primary care pandemic preparedness so that clinicians can better anticipate which patients would require more attention. 19
That participants in Project ECHO COVID-19 sought to find a balance between caring for individual patients and public health safety reflects decades of effort before the pandemic to foster a better partnership between these 2 sectors of health care.20-23 Despite evidence that collaboration can improve outcomes, especially for chronic and communicable diseases, barriers have persisted, most notably a lack of a “common agenda” for health. 20 Perhaps COVID-19 has allowed primary care and public health to find common ground, as evidenced by more recent papers addressing the lessons learned from the pandemic thus far.24,25 Those lessons are reflected in the concerns raised by our participants as their focus shifted from patient care to operations. They include: adapt care delivery operations, such as telehealth, triage, and testing; leverage the electronic health record for population-level data; redeploy and retrain staff and ensure their safety; secure supply chain for equipment and medications; and optimize communication during a crisis, especially at the community level among health care agencies.24,25
Finally, there is a need for leadership to implement policies that will ensure not only preparedness in primary care settings for the next pandemic, but better health care overall through public health-primary care partnerships.2,19,24,25 Had this Project ECHO been limited to clinical care only, it would have missed participants’ shift in focus to these pressing issues, and the opportunity to confirm that their concerns and questions are reflected in lessons learned across the country.
A limitation of this study is the lack of clinical data from participants about the outcomes that resulted from practice changes they made as a result of participating in our program. Given the size of the audience, the variability in attendance, and the lack of clinical guidelines, this limitation is to be expected. Additionally, our analysis of the Q&A data was not linked to the role type of the participants. As such, our findings do not showcase the needs and concerns raised solely by primary care providers, but instead shows the concerns raised by a diverse group of health care professionals.
Conclusion
Public health epidemic preparedness programs do not typically address the issues of caring for vulnerable populations and adapting clinical operations, yet they were top of mind issues for participants in Project ECHO COVID-19. Our results confirm the importance of a partnership between primary care and public health organizations when communities prepare for public health crises. Doing so will enable clinicians and communities to quickly tailor health services to meet critical needs, not just in the midst of a pandemic but as best practice in general.
Adapting the Project ECHO model to be a more scalable learning community for health care professionals to receive timely information during an evolving public health crisis was critical. Project ECHO COVID-19 was able to share relevant and timely information while providing a space for health care workers to have urgent questions answered by experts in the field when limited evidence-based guidance was available. Future studies should investigate to what extent adapting the Project ECHO model to unique circumstance such as a health crisis undermines its effectiveness or expands on it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.