
Abstract
Background:
In this report, we outline our approach to implementing a hybrid in-person and virtual clinic model at a student-run free clinic (SRFC) during the COVID-19 pandemic. Individuals of low socioeconomic status (SES) are at an increased risk for COVID-19 infection and severe clinical outcomes. It is unclear if telehealth is a viable continuity of care enabler for the underserved.
Methods:
The Weill Cornell Community Clinic (WCCC) implemented a novel telehealth clinic model to serve uninsured patients in May 2020. A phone survey of was conducted to assess WCCC patients access to technology needed for telehealth visits (eg, personal computers, smartphones). Patient no-show rates were retrospectively assessed for both in-person (pre-pandemic) and hybrid continuity of care models.
Results:
The phone survey found that 90% of WCCC patients had access to technology needed for telehealth visits. In the 8 months following implementation of the hybrid model, telehealth and in-person no-show rates were 11% (14/128) and 15% (10/67) respectively; the combined hybrid no-show rate was 12% (24/195). For comparison, the in-person 2019 no-show rate was 23% (84/367). This study aligns with previous reports that telehealth improves patient attendance.
Conclusion:
Literature on the transition of SRFCs from in-person to telehealth care delivery models is limited. At the WCCC, the reduction in no-show rates supports the feasibility and benefits of adopting telehealth for the delivery of care to underserved patient populations. We believe the hybrid telehealth model described here is a viable model for other student run free clinics to increase access to care in low SES communities.
Background
The Weill Cornell Community Clinic (WCCC) is a student-run free clinic (SRFC), which provides longitudinal primary care to uninsured New York City residents earning less than 400% of the Federal Poverty Line. WCCC patients are predominantly racial or ethnic minorities and are non- native English speakers. WCCC is a rotation site for Weill Cornell’s required Primary Care Clerkship. In March 2020, because of the COVID-19 pandemic, WCCC temporarily suspended in-person clinical care for the safety of both patients and providers. In May 2020, WCCC rolled out a novel telehealth clinic model to maintain access to care for our patients (Figure 1).
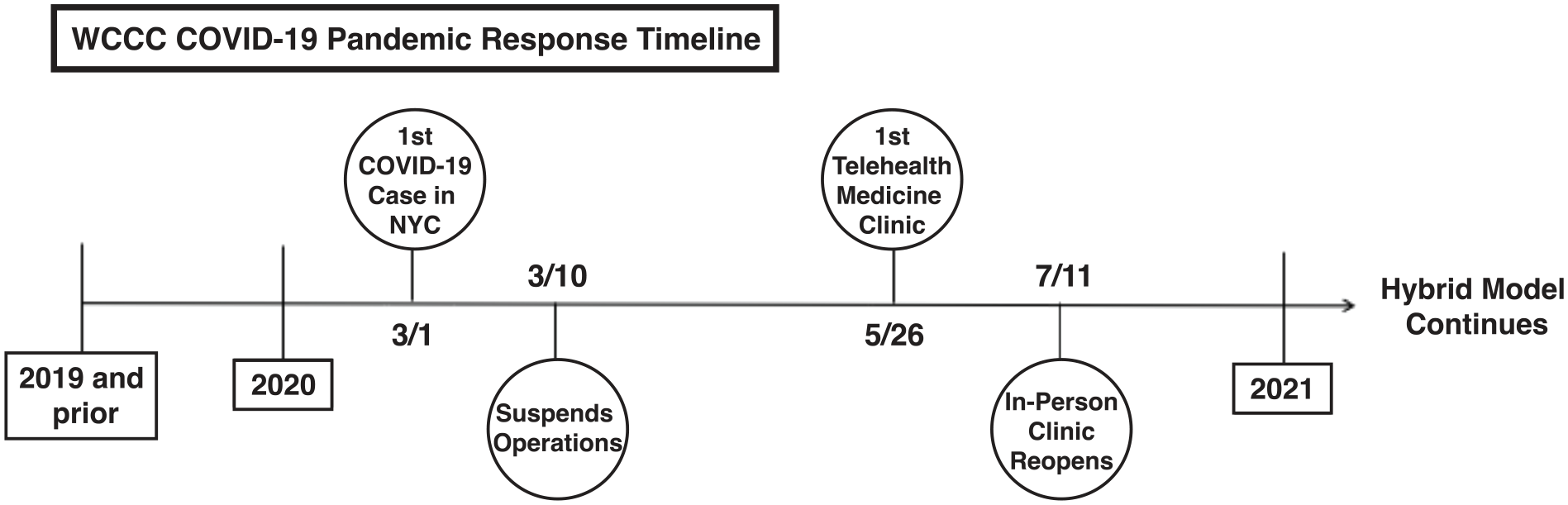
Timeline of Weill Cornell Community Clinic’s transition to telehealth.
COVID-19 Disproportionately Affected the Health of Low Socioeconomic Status Patients
Previous studies show that minorities and individuals with low socioeconomic status (SES) have poorer health outcomes at baseline, are at an increased risk for both COVID-19 infection and if infected with SARS-CoV-2, are more likely to have worse clinical outcomes.1 -7 The increased risk of COVID-19 in the minority and low SES communities is thought to be due to a combination of structural factors such as the higher proportion of essential workers that are unable to work remotely and higher rates of public transportation use during the pandemic (ie, exposure to dense public spaces).4,5
Among individuals infected with SARS-C-19, minority and low SES patients are more likely to experience severe COVID-19 infection, hospitalization, and death1 -3; this is attributed to the higher baseline prevalence of comorbidities such as diabetes, hypertension, and obesity, all of which are independent risk factors for worse outcomes in COVID-19. Another contributing factor to poor COVID-19 outcomes among minority and low SES individuals, which is the focus of this paper, is reduced access to care. 2
The COVID-19 Pandemic Decreased Access to Care Amongst Low SES Patients
The COVID-19 pandemic led to a broad-based decrease in primary care access that was more pronounced among low SES patient populations. In the primary care setting, a recent cross- sectional analysis of the US National Disease and Therapeutic Index audit of more than 125.8 million primary care visits showed decreased visits by 21.4% during the second quarter of 2020 compared to pre-pandemic quarters.8,9 Furthermore, between April and July 2020, over 3 million adults lost employer-sponsored health insurance and the number of uninsured adults increased by nearly 2 million. 10 The steepest declines in access to care during the pandemic were seen among minorities and low SES individuals. 10 Taken together, pandemic-related decreases access to care disproportionately affected already vulnerable patient populations. 11
The Telehealth Boom
The rapid uptake of telehealth, a safe and socially-distanced health care modality, during the COVID-19 pandemic was an important mitigating factor against the decline in in-person care availability.12 -15 The use rate of telehealth services increased substantially across the US in the early weeks of March 2020, coinciding with rising rates of COVID-19 cases.16,17 This rapid expansion of telehealth services offered by healthcare providers in 2020 intersected with an expanding network of patients with access to smartphone technology. This could not have occurred without a substantial increase in smartphone access from 2011 to 2019.18,19
Among low SES individuals, there have been large gains in access to smartphones and telehealth-enabling technologies in the previous decade. The percentage of U.S. adults, including those of low SES, with access to a smartphone has increased from 35% to over 80% from 2011 to 2019.18,19 That said, among low SES individuals, there is limited data on telehealth engagement. At WCCC, the COVID-19 pandemic necessitated rollout of a hybrid model to maintain access to care for our patients. In this study we report on the impact of the hybrid model on primary care access in a low SES patient population.
The Importance of Sharing Telehealth Models
A clear understanding of effective strategies for deploying telehealth in low SES populations is needed. 20 Multiple telehealth models have been trialed by SRFCs during the COVID-19 pandemic to maintain access to care among vulnerable populations.21 -23 One of these studies reported a decrease in no show rates following the implementation of telehealth, albeit with limited data only spanning 2 months. 21 Here, we provide an in-depth discussion on the implementation of a telehealth model with fully remote visits and the impact on clinic attendance rates. To our knowledge this is the first study to report on primary care attendance rates (stratified by no-shows and cancellation) among low SES patients during the pandemic in conjunction with survey information on their access to telehealth-enabling technologies.
Primary Outcomes
WCCC patient no-show rates were assessed over an 8-month period starting in May 2020; for comparison, no-show rates during the 12-month pre-pandemic period from January through December 2019 were also assessed.
A telephone-based survey was used to assess WCCC patients’ access to technology needed for telehealth visits such as computers, tablets, smartphones and other devices.
Methods and Materials
Telehealth Model Design
In-person clinic operations were suspended for 3 months due to COVID-19 in the spring of 2020. To safely enable primary care access for our SRFC patients, a HIPAA-compliant telehealth clinic model was rolled out using Zoom and Doximity Dialer in May 2020 (Figure 2). Detailed information on our clinic workflow and set-up is included in the Supplemental Information.

Weill Cornell Community Clinic’s Telehealth Clinic workflow overview.
Virtual Clinic Set-Up
To maintain both the patient care and educational structure of our in-person clinic, several Zoom features were utilized such as the “Waiting Room” and “Breakout Room” to enable HIPAA compliant discussions among the interdisciplinary healthcare team. A “Front Desk Coordinator” admitted each patient from the virtual waiting room to a private Zoom session their care team.
Within Zoom, Breakout Rooms were leveraged as virtual examination rooms for individual patients and marked with patient’s initials to maintain privacy. A separate Breakout Room was used as work room for medical students to present their findings to attending physicians, to facilitate both patient-care component and student education.
For non-English encounters, contracted telephone interpreter services or certified student translators were seamlessly conferenced into Zoom or Doximity Dialer. Also, in addition to primary care, patients the telehealth workflow allowed patients to meet virtually with registered social workers between their initial medical student and attending physician encounters.
Clinic-Day Preparations and Protocols
WCCC patient scheduling coordinators sent confirmation emails with the clinic Zoom link and patient-centric Zoom guides to each scheduled patient the day of their appointments (Supplemental Figures). These coordinators also provided instructions over the telephone if patients did not have access to a working email address. An interdisciplinary team comprised of attending physicians, medical students, social workers, pharmacists, pharmacy students, and nutritionists provided comprehensive care to clinic patients during each session. Clinical Directors provided provider-centric Zoom guides to the clinical team prior to each session to establish expectations and establish a workflow for the patient care team (Supplemental Figures). The medical student clinicians conducted follow up patient phone calls to confirm medical management plans and provide any needed clarifications and/or counseling. If labs, vaccines, imaging or other in-person procedures were indicated, clinic Referrals Coordinators scheduled patients for procedure-specific appointments. When a return to in-person clinic operations was permitted, WCCC transitioned to a hybrid model, which supported telehealth and in-person clinics on alternating weeks. Detailed information on our clinic workflow and set-up is included in the supplementary information.
Study Design and Data Collection
Demographic information and clinic attendance (ie, no shows and cancelations) was collected from clinic records. Prior to each clinic session, trained medical students surveyed scheduled patients about their access to telehealth-enabling technologies. This study was reviewed and evaluated by our Institutional Review Board.
Sample Details and Statistical Analysis
In a retrospective analysis, 367 and 195 patients attended, cancelled, and or missed Internal Medicine clinics between January 2019-December 2019 and May 2020-December 2020 respectively. Statistical significance was determined with the 2-population proportion Z test. The P-value threshold of significance was set at .01 for all analyses.
Results
The WCCC patients included in these analyses were 23% white, 18% as Hispanic/Latino, 13% Black or African American, 6% as Asian, and 23% as “Other.” A quarter of the study population were non-English speakers; the 6 primary languages reported were Spanish, Russian, Portuguese, French, Bengali, and Mandarin.
From May to December 2020, 195 Internal Medicine, 65 Gynecology, and 54 Mental Health clinic visits were scheduled. This visit volume in 2020 (n = 314) was comparable to the visit volume during the same period in 2019 (n = 308).
Among patients seen using telehealth, 90% had devices that supported a video component (47% smartphone; 43% computer); the remaining 10% of patients used a conventional phone for audio-only visits. Notably, no telehealth visit were declined by WCCC patients.
The no-show rate for Internal Medicine telehealth visits was 11% (14/128); From May to December 2020 the in-person no-show rate was 15% (10/67) and the combined telehealth and in-person no-show rate was 12% (24/195), the latter a decrease from the in-person 2019 annual rate of 23% (84/367), (P < .01) (Figure 3).
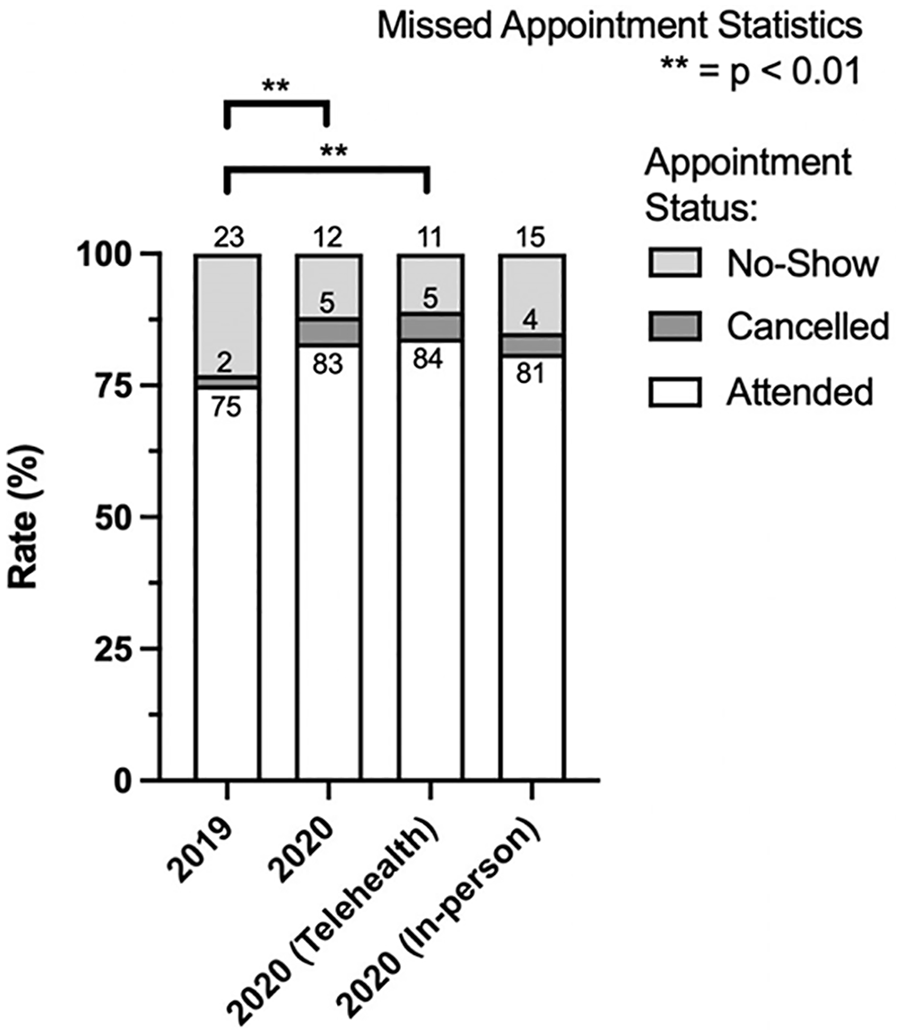
Attendance and No-show /Cancel Rates. Data shown for 2020 telehealth only, 2020 in-person only, 2020 combined total, and 2019 total.
Discussion
The WCCC transition to a telehealth model during the pandemic was borne from necessity—there was a critical need for primary care continuity among our minority and low SES patient population who were at increased risk for being infected with SARS-CoV-2 and experiencing severe COVID-19 disease. SRFCs are a unique type of clinic and, in spite of a strong emphasis on documenting the implementation and outcomes of telehealth models, literature on successful implementation of telehealth models is limited. 20 The reported findings offer useful insights on the viability and sustainability of a telehealth-based SRFC primary care clinic.
During the pandemic, the transition to a telehealth model allowed WCCC to safely maintain patient appointment volume when nationwide primary care access was limited. At WCCC, 90% of the virtual visits were conducted with video-enabled devices. Among patients who did not have access to video-enabled devices, telephone visits were scheduled.
During the study period, there were no recorded patient refusals to participate in the telehealth care model. Furthermore, our data show that our telehealth clinic model improved access to care relative to our pre-pandemic in-person only visit model. As such, the WCCC telehealth clinic model will continue beyond the COVID-19 pandemic.
In a post-pandemic setting, the success of this model is likely due to the convenience it affords. Survey results showed 90% of WCCC patients have access to required technology; the pandemic was a tailwind for encouraging patients to participate in the telehealth; having gained familiarity with telehealth we believe there is value in leveraging this care modality to mitigate longstanding barriers to primary care access such as travel-time, access to child care, and limited paid time off for low-income workers who rely on hourly-wages. 24
Limitations of this study include its retrospective nature, and limited sample size. Despite analyzing attendance rates, this study lacks clinical outcomes data, which will be addressed in future work. Further future aims are to improve upon our telehealth implementation through further assessment of patient experience and examination of clinical outcomes. For example, telehealth visits can be limited by challenges in obtaining objective data such as vital signs. To address this gap, we have initiated the distribution of blood pressure cuffs to hypertensive patients for home blood pressure monitoring as well as thermometers and pulse oximeters to all registered patients with guidance and counseling on proper use.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221114831 – Supplemental material for A Medical Student-Run Telehealth Primary Care Clinic During the COVID-19 Pandemic: Maintaining Care for the Underserved
Supplemental material, sj-docx-1-jpc-10.1177_21501319221114831 for A Medical Student-Run Telehealth Primary Care Clinic During the COVID-19 Pandemic: Maintaining Care for the Underserved by Joshua W. Bliss, Annie Yau, Elena Beideck, Jesse S. S. Novak, Felipe B. d’Andrea, Nicolas J. Blobel, Ashita S. Batavia and Pamela Charney in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank all members of the general and director boards, volunteer student clinicians, volunteer allied professionals, and volunteer attending physicians for their unwavering dedication to the mission of caring for the underserved. J.S.S.N., F.B.D., and N.J.B are predoctoral fellows of the Weill Cornell/Rockefeller/Sloan Kettering Tri-Institutional Medical Scientist Training Program (T32GM007739).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.