
Abstract
Objective
In recent years, family medicine (FM) has shown many changes, including the development of sub-specialization. This study aimed to explore the opinions, preferences, and practices of Saudi family physicians with regard to sub-specialization within family practice.
Methods
This cross-sectional study was conducted from January to May 2018. Data were collected from 561 Saudi FM board-certified physicians and family medicine residents from all over SA via personal emails using a self-administered questionnaire consisting of questions aimed at examining participants’ opinions, preferences, and practices with regard to sub-specialization in family practice.
Results
Only 48 family doctors (20.2%) had the qualification of subspecialist. Diabetology was the most common clinical subspecialty. The majority of participants agreed with the statements in favor of sub-specialization in FM. About 73% approved of the idea of sub-specialization in FM, while 89% thought that sub-specialization would provide a source of expertise within the FM context. The most stated reasons to go for FM subspecialties were to earn more experience (65.1%), gain some sense of control of huge knowledge and skills of FM (53.7%), and earning extra money (47.8%).
Conclusions
This study revealed that majority of certified family physicians and FM residents in SA have positive attitude towards sub-specialization in FM and support the idea of sub-specialization to be practiced within the context of FM
Introduction
Since 1969, family medicine (FM) has undergone development as a core specialty following the continuous specialization, sub-, and sub sub-specialized in medical practice in the early 20th, leading to doctor-centered, and patient-fragmented care.1-3
Family physicians are general physicians who take care of all age groups and both genders for common acute and chronic illnesses in a biopsychosocial approach. This approach has proven to be cost-effective with good clinical outcomes and high patient satisfaction.4-11
In recent years, FM has shown changes in many aspects, including worldwide sub-specialization.
In the United States (US), family doctors who have completed their training through the American Board of Family Medicine have the opportunity to subspecialize in certain areas of interest and are recognized and privileged by their institutions,12-14 while many Canadian family physicians are practicing subspecialties either part- or full-time. 15
Likewise, in the United Kingdom (UK), a general practitioner (GP) with a Special Interest (GPwSI) is a pathway for certified general practitioners (GPs). 16
FM in Saudi Arabia (SA) was recognized as a medical specialty in 1982. FM training was started in few universities as fellowship after that time. The Saudi Board of Family Medicine (SBFM) was launched in 1995 by Saudi Commission for Health Specialties (SCFHS) as 1 of the first 5 postgraduate medical specialties.17,18
Recent reports have revealed that there are more than 1500 certified family physicians although the country still faces shortages in family physicians as the total need is estimated to be 15,000.19,20
Despite the high need for qualified family doctors, the debate continues regarding the concept of sub-specialization in FM.1,14,21-27 SA is not an exception regarding this debate as it is a hot topic of debate among family physicians, and at higher levels in Ministry of Health and Scientific Council of Family Medicine.
To our knowledge, no studies done in SA have examined the opinions and preferences of family physicians regarding the concept of sub-specialization in FM or to identify the current situation of practicing FM subspecialties.
This study aimed to explore the opinions, preferences, and practices of family physicians with regard to sub-specialization in family practice in SA.
Methods
This cross-sectional study was conducted from Jan to May 2018. The study population consisted of Saudi FM board-certified physicians and family medicine residents throughout the country.
A list of 1994 board-certified, board-eligible, and active trainee family physicians with their emails was obtained from different resources. Using www.Raosoft.com for calculating the sample size for this study with margin error of 5%, confidence interval of 95%, total targeted participants of 1994, and 50% of respondents to have positive attitude or opinions towards sub-specialization in family medicine, the minimum sample size was 323 participants. The sample sized was increased to compensate for incomplete data.
Data were collected using a self-administered questionnaire. In developing the study questionnaire and to achieve the study objectives, the investigators reviewed relevant literature and developed and validated a two-section questionnaire. The first section included questions related to participants’ demographic data (age, gender, region, current title, sector, qualification, duration after certification, qualification, and practice of sub-specialties in FM) while the second section included questions examining participants’ opinions and preferences with regard to sub-specialization in family practice.
The content validity was determined by 3 subject matter experts. A pilot study was conducted to determine the reliability, whereby the questionnaire was distributed among a convenient sample of 30 participants. The reliability of the questionnaire was evaluated using the Cronbach’s alpha test to assess the internal consistency of the questionnaire and the split-half technique was used to assess the homogeneity of the questionnaire.
Data were entered and analyzed using Statistical Package for Social Sciences version 20 (SPSS, 20) software. Descriptive statistics was performed in the form of frequencies and percentage for categorical variables of gender and social status, while mean and standard deviation (SD) were used for description of continuous variables. Analytical statistics were done using a chi-square test (χ2) to assess differences between categorical variables. Means were compared using independent student-t test (analysis of variance when applicable). Statistical significance was set to ≤ .05.
Ethical Considerations
Approval of the study was obtained from King Abdullah International Medical Research Center, Ministry of National Guard, Riyadh, SA with approval number RC17/255/R, dated 2 Nov 2017. Consent was obtained from participants when the questionnaires were distributed. All data were kept confidential and used only for research purposes.
Results
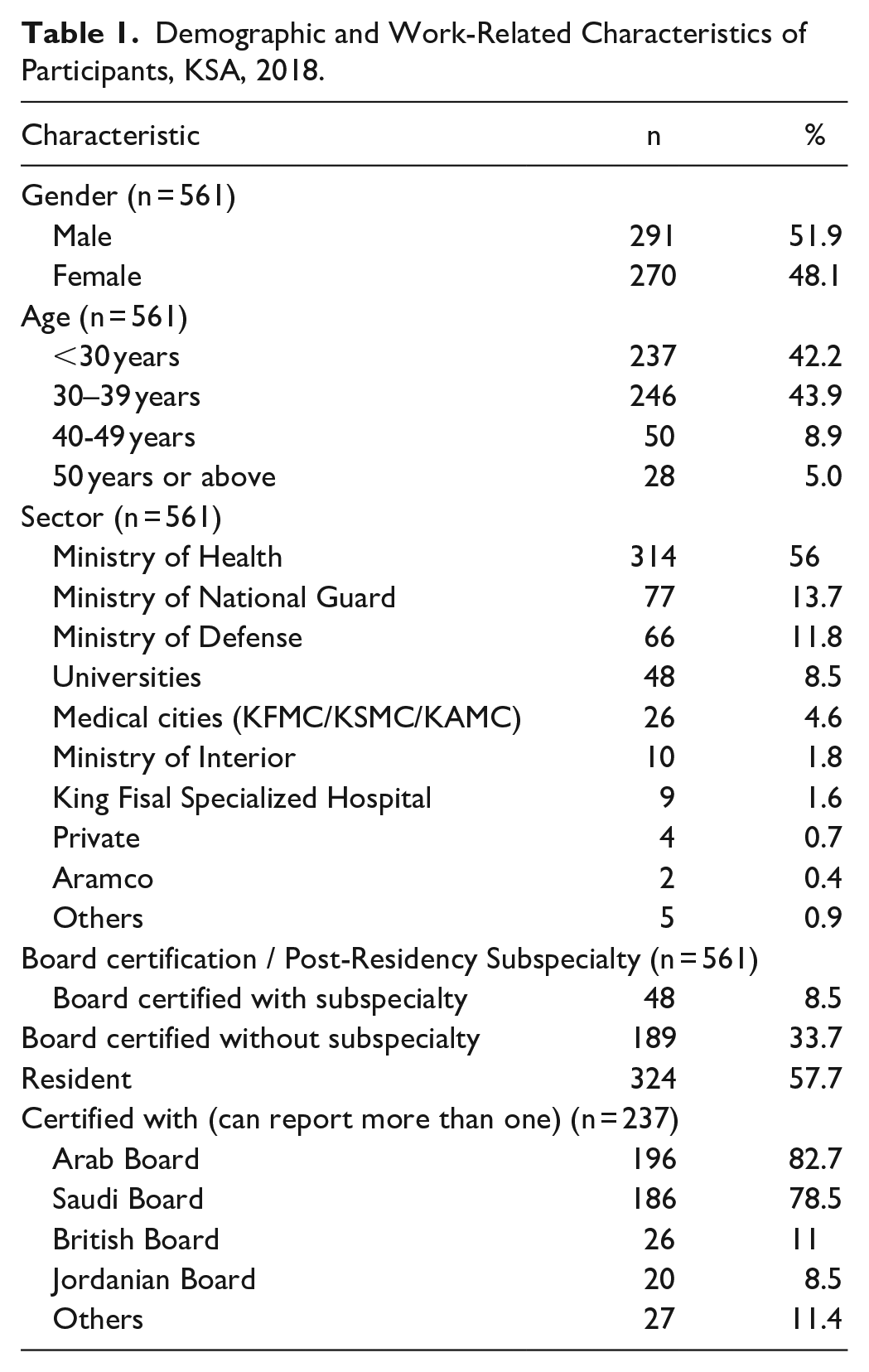
Total of 561 completed the study questionnaire. Table 1 summarizes the participants characteristics.
Demographic and Work-Related Characteristics of Participants, KSA, 2018.
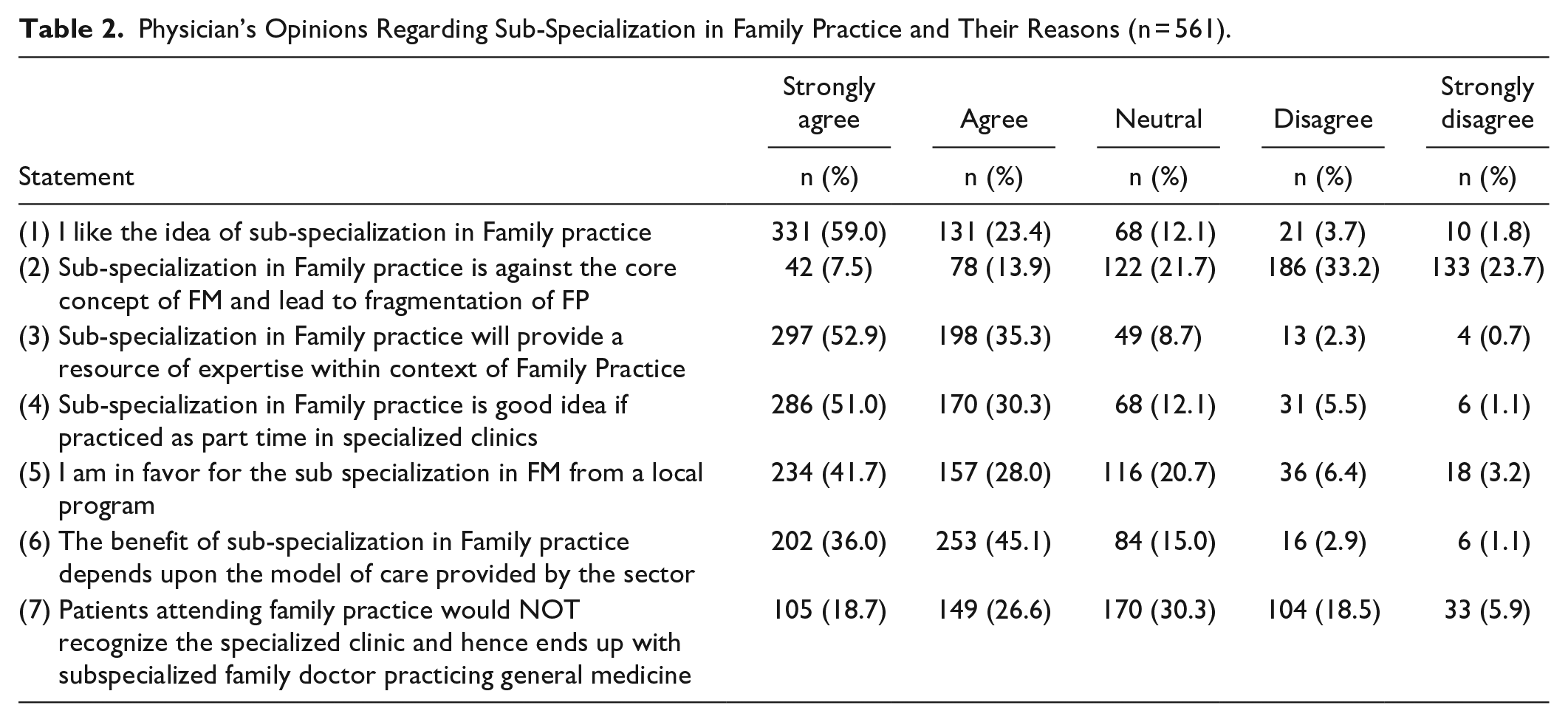
The majority of participants agreed with the statements in favor of sub-specialization in FM. About 73% approved of the idea of sub-specialization in family medicine, while 89% thought that sub-specialization would provide a source of expertise within the context of family practice (Table 2).
Physician’s Opinions Regarding Sub-Specialization in Family Practice and Their Reasons (n = 561).
The most stated reason to apply for an FM subspecialist was to earn more experience (65.1%) followed by gaining a sense of control over the huge amount of knowledge and skills within FM (53.7%), and earning extra money (47.8%), as shown in Figure 1.

Most reasons why family physicians go for subspecilaities.
Table 3 shows the subspecialty related characteristics among family physicians with sub-specialties. Only 48 family doctors (20.2%) were having such qualifications. Diabetology was the most common clinical subspecialty (29.2%). Around two thirds were recognized by Saudi Commission for Health Specialties for their subspecialty degree, 68.8% are privileged by their institutions, and 87.5% are practicing their subspecialties.
Clinical Profile of Family Physicians Holding Post-Board Certificates in Subspecialties (n = 48).

Among physicians with no subspecialty, the 2 most common reasons were either not having an opportunity (32.0%) or they were applying soon. About 8% did not believe in sub-specialization in FM, and 6.4% were not interested in this aspect of FM (Table 4).
Choice of Preferences for an Opportunity for Subspecialty Among Physicians Who Are Board Certified and Residents in Saudi Board Family Medicine, KSA.

In regard to board certified doctors without subspecialty, local programs for sub specialization were mostly preferred by younger doctors (less than 30 years age) and female group (P = .019 and .037, respectively), while abroad programs (outside scholarship) were preferred more by 30 to 39 years group with P = .000. For the mode of study for subspecialty, part time was the most preferred option again among young doctors (less than 30 years), and the least preferred option in age group 30 to 39 years (P = .000). In regard to mode of practice after getting the sub-specialization board, part time was the preferred mode among all age groups with no significant difference. No significant difference was found between male and female doctors in regard to the preferred mode of study or mode of practice of subspecialty.
Among residents, no significant difference was found between different age groups or male and female doctors in regard to preferred program of study, mode of study or mode of practice.
Discussion
This is the first study in SA investigating the opinions, preferences and practices of family physicians in regard to sub-specialization.
The study clearly revealed that the majority of Saudi family physicians are in favor of sub-specialization in FM. This feeling is clear from the agreement or strong agreement with the listed statements in favor of sub-specialization and from the reasons listed as to why the majority of board-certified physicians do not yet subspecialize. The 2 main listed reasons were either no opportunity yet or planning on applying soon. For example, the vast majority had the idea that sub-specialization in FM will provide a source of expertise within the context of family practice.
This finding indicates that most of participants not only support the idea of sub-specialization in FM would practice a sub-specialty within the context of FM. This finding also is relevant for residents in training in which almost 60% certainly would go for sub-specialization if they are presented with the opportunity to study in a local or outside program.
The issue of sub-specialization in FM is very debatable, both locally and internationally. On one side, supporters think that sub-specialization in FM would provide family physicians with extra training in a focused area, making them experts in certain fields in the context of FM, providing a source of expertise within the family practice, and gaining more recognition and a good reputation among health professionals.1,22-25 On the other hand, those against the concept argue that sub-specialization in FM is against the core concept of FM, which is general practice. It is felt that sub-specialization would eventually lead to fragmented patient care, a requirement for monitoring and recertification by mother sub-specialties, creation of confusion among patients about physician qualifications, and discourage family physicians from pursuing the specialty.14,22-28
Among the reasons participants stated for going to sub-specialization in FM, the main 1 reason was “to earn more experience while keeping FM” followed by “to gain some sense of control of huge knowledge and skills of FM,” and “earning more money.” The least reported reasons were to have Western qualifications and a better reputation and prestige. These reasons are similar to what has been reported in other studies. 1
While the number of board-certified physicians who have subspecialties in this study was low (20.2%), the majority of board-certified physicians without subspecialties stated that they certainly would go for a sub-specialization if the opportunity presented itself, either in a local or outside program.
For comparison, among certified Canadian family physicians, 30% are family physicians with a focus on parasciences, and almost 80% are family physicians with special interests. 26 Family physicians with special interests are “traditional comprehensive continuing care family practices who act as the personal physicians for their patients and whose practices include 1 or more areas of special interest as integrated parts of the broad scope of services they provide.” The focused practice designation is applicable to family physicians with a “commitment to 1 or more specific clinical areas as major part-time or full-time components of their practices.” 29
Among residents in this study, it is interesting that the majority “certainly” will go for subspecialties if they are given the opportunity. This number is much higher than what is reported, for example, in Canada, in which about 30% of Canadian FM residents plan to have specialized practices, 25 and in the US, in which almost 1 in 5 residents planned to do a fellowship, such as sports medicine, geriatrics, maternity care, and hospice/palliative care being the most actively pursued fellowships choices after the residency.
The 5 top subspecialties among study participants were diabetology, medical education, geriatrics, health management/administration, and healthcare quality. In comparison, the most popular areas of focus among Canadian family physicians are emergency and geriatric medicine followed by obstetrics and palliative care. 26
Fellowship in diabetology is one of the earliest fellowship programs open for family physicians in SA, and this finding may explain why it is the most frequent subspecialty in addition to the fact that diabetes mellitus is a prevalent disease in SA. Family physicians are encouraged to meet the national need and go into this subspecialty. Likewise, medical education, health administration, and quality assurance are open and available as academic master’s programs since there is long-term need for all healthcare professionals. All family physicians pursue a fellowship in geriatrics from outside programs because during the study period, no local programs were started.
Clinical fellowships were obtained by 55%, while 45% had non-clinical specialties, such as healthcare administration, medical education, and quality assurance. Such findings should make the authorities in healthcare sectors alert to maintaining the balance between clinical and non-clinical careers for family doctors who prefer to have post-board qualification as we need to have practicing family physicians rather than administrators or educationalists.
Almost 1 quarter of participants with subspecialties could not obtain recognition of their fellowships by SCFHS. For clinical subspecialties, this finding means that they cannot practice their subspecialties. The possible reason the lack of recognition by SCFHS is lack of clear rules and regulations and lack of unified system of recognition between the Scientific Board of Family Medicine and classification and registration department in SCFHS.
Setting criteria or establishing or recognize subspecialty FM certification in SA is an important need that should be fulfilled by Scientific Board of Family Medicine in SCFHS. This process should be based on real community needs and on the ongoing reform of the healthcare system in SA, which recognizes the increasing role of FM in healthcare delivery. The new model of care and clustering system, as proposed by Saudi Ministry of Health, would be a great opportunity for FM physicians to practice their specialties, where specialized clinics can be operated within the FM premises. This should be considered seriously in the process of re-structuring and re-organizing the service. To ensure comprehensiveness of FM and avoidance of care fragmentation, the specialized clinics should be run in part-time basis and only for difficult or complicated cases with established clear internal referral system.
Most participants reported practicing their subspecialties either as a part-time duties for academic and research interests, in part-time specialized clinics, or within their FM practice (no special clinics). This finding indicates that the majority of FM physicians are eager to keep their main specialty, that of FM.
Only a minority are not practicing their subspecialties. The reasons behind that finding are different. Maybe they have not been recognized for their subspecialties by SCFHS, not granted privilege by their institutions, or there is the lack of a suitable setup in their practices.
Conclusions and Recommendations
This study revealed that the majority of certified family physicians and family medicine residents have positive attitudes toward sub-specialization in family medicine, and support the idea of sub-specializations to be practiced within the context of FM.
On-the-job vocational training for 1 to 2 years may be a good option for board-certified physicians to gain fellowships in highly needed clinical subspecialties.
Limitations
The study data are based on self-reporting by the physicians. Low response rate also is considered a limitation for the present study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.