
Abstract
Background:
South Africa adopted the ward-based outreach team (WBOT) program as one aspect of the three-stream approach to primary health care (PHC) re-engineering. PHC re-engineering seeks to modify the hospicentric and curative approach into a more preventive and promotive approach to improve health outcomes. There has not been an evaluation of the implementation of the WBOTs in Nkangala District since its inception in 2012.
Methods:
A process evaluation approach using qualitative methods was used to examine and describe the contextual, organizational, health provider, and program-related barriers considered to affect the implementation of the WBOTs 3 sub-districts in one of the health districts in Mpumalanga Province, South Africa. The framework for this evaluation was informed by the logic model framework developed by the Center for Disease Control as well as the 3 domains of evaluation recommended by the Medical Research Council Guidance on process evaluation. Data were collected through in-depth interviews with multiple data sources directly involved in the implementation of the WBOTs. A thematic analysis was done using NVivo 11.
Results:
The key critical barriers identified by the evaluation include the inadequate provision of resources, the lack of supervision, the heavy workload for outreach teams, the inadequate and irregular payment of stipends, threats to the safety of the CHWs, and the cultural beliefs and practices of the communities who are to receive the services. The lack of adequate financial resources was the main challenge, and will continue to pose a risk to the successful implementation of the WBOTs.
Conclusions:
Although the barriers are being reported as separate contextual factors, the internal and external contexts are interdependent, interact with one each other, and should not be considered in isolation. The need to improve stakeholder engagement on the WBOT program underscores the importance of the external context in the successful implementation of WBOTs.
Keywords
Introduction
South Africa’s health transition is characterized by a quadruple burden of communicable, non-communicable, perinatal and maternal, and injury-related disorders. The country faces relentless burden of infectious and non-communicable diseases that the health system fails to combat due to fragmentation of the healthcare system. The high burden of the HIV and AIDS epidemic coincide with high burden of tuberculosis, high maternal and child mortality, high levels of violence and injuries, and a growing burden of non-communicable diseases.1,2
In response to the national health crisis, the South African Government had developed a comprehensive plan to transform its health system by strengthening primary health care (PHC). Improving the quality of health care is central to the proposed health care reforms in South Africa. In 2011, the National Department of Health (NDoH) introduced the re-engineering of PHC strategy and adopted the three-stream approach to PHC re-engineering. 3 The PHC re-engineering model emerged from experiences in other countries showing that the provision of home- and community-based health services and their links with the fixed PHC facilities in particular, are critical to good health outcomes. 4 The PHC re-engineering model established in South Africa puts strong emphasis on community- based care and includes social determinants of health in its approach. 5 PHC re-engineering seeks to modify the hospicentric and curative approach into a more preventive and promotive approach with the aim of improving health outcomes. 6
The 3 streams of PHC re-engineering are a ward-based PHC outreach team for each electoral ward (WBOT), strengthening school health services, and district-based clinical specialist teams. 6 The WBOT program was designed to correct limitations in the way community-based health services were provided in the country. 6 Although South Africa already has about 72 000 community health workers (CHWs), 7 the country is unable to generate better health outcomes and suboptimal health outcomes in the areas of maternal and child health persist. 5 Thus the activities of WBOTs are household focused, with preventive maternal-child health interventions and follow-up of chronic lifelong conditions in adults forming the 2 key components. 8 The WBOT program plays a critical role in extending PHC services to community and household level and making health accessible in terms of distance and information. 9
The WBOT is attached to a primary health facility and operates within a municipal ward to provide promotive and preventive services to individuals at community level. 10 Each team is composed of a professional nurse, environmental health practitioners, health promotion practitioners, and community health care workers (CHWs). 5 The main functions of these teams are to promote good health and prevent ill health through a variety of interventions based on the concept of a healthy community, a healthy family, a healthy individual, and a healthy environment. 11 The national norm indicates that each team should serve a population of about 6 000 with at least 1000-1500 households (depending on the density of the population, the burden of disease, and the geography). 3
The NDoH defines and standardizes the CHW’s scope of work, roles and responsibilities, training, supervision, and remuneration packages as well as other working conditions. 3 Each HCW is responsible for about 250 households; however, in Mpumalanga province this number is 150 because of the rural nature of the province. The CHWs conduct household visits and register the households. During the household visits they are expected to identify people at risk and to take appropriate steps to link them to care. 6 The team leader is responsible for 6 CHWs, for ensuring that their work is targeted and linked to service delivery targets, and for ensuring that they are adequately supported and supervised. 3
The WBOT program was introduced in Mpumalanga Province in 2011 and Nkangala district established its first WBOT teams in 2012 in a phased approach commencing with 3 sub-districts. The selection of the 3 sub-districts was based on the prioritization of the comprehensive rural development program (CRDP) sites.
We conducted a process evaluation of the implementation of the WBOTs in 3 sub-districts which have implemented the program since its inception in 2012 in Nkangala District. If well implemented, the ward-based outreach program has the potential to address limitations experienced previously with community based health services, to improve access to PHC services, and subsequently to improve health outcomes. Similarly, when CHWs have a manageable workload, the needed supplies and equipment, a supportive supervisor, and respect and acceptance, they function more productively and contribute to an effective community-based strategy. Barriers and facilitators in community-based services are tied mainly to program acceptability, appropriateness, credibility and health system constraints. 12
There has not been a previous evaluation of the implementation of the program in this district. It should also be noted that the implementation of the program in Nkangala District has been incremental in the different areas. The program can therefore not be viewed as mature, despite its having been operational for 5 years. Process evaluations is an essential part of community-based interventions 13 which is needed to provide insight into how well program activities are implemented and are performing in the context in which implementation occurs. Process evaluation assumes greater importance in the case of large, complex community-based intervention such as the WBOT program, which deliver multiple, non-standardized interventions tailored to specific communities. 14
The purpose of the evaluation was to assess how the ward-based outreach team program is being implemented by managers, team leaders and CHWs, as well as to assess the acceptability of the program.
The process evaluation answered the following questions:
How is the primary health care WBOT program currently being implemented in Nkangala district?
How acceptable is the WBOT program to managers, community health workers, and clients in the district?
What are the barriers against and facilitators of the implementation of the WBOT?
What are the recommendations of managers, CHWs, and clients for the improvement of the implementation of the WBOT program in the district?
This paper reports on the analysis of the barriers against the implementation of the WBOTs in Nkangala district from the perspectives of those involved in implementing the WBOT program, and describes how and why each contextual factor is important in the implementation and uptake of the WBOT.
Methods
The framework for this evaluation was informed by the logic model framework developed by the Center for Disease Control. The logic model framework inform evaluation practice and is composed of 6 steps, but in a process evaluation, the focus is on the first 3 segments of the logic model (inputs, activities, and outputs) and how they work together. Inputs, describe resources needed to operate a program or resources a program has available to implement its activities and attain the desired outputs and outcomes. In the current evaluation, inputs include human, material, financial, and infrastructure resources essential for program activities such as training, stakeholder engagement meetings, community awareness campaigns, and household registration visits. Activities describe what the program does with the resources. They are the processes, actions, and steps in implementing a program. In the current evaluation, activities include establishing WBOTs, conducting trainings, procurement of equipment, and household calls by WBOTs. Outputs provide information derived from the completion of program activities. They are tangible process-oriented results typically expressed in numbers. In the current evaluation, these include number of program staff trained, house calls, outreach teams established, and material resources procured. The framework was used as a theory of change to present and share the understanding of the relationships among the program inputs or resources available to implement the program, the activities and their links to the anticipated outcomes of WBOTs 15 (Figure 1).

WBOT logic model.
We also integrated the 3 domains of evaluation recommended by the Medical Research Council (MRC) guidance on process evaluation, namely, implementation, intervention mechanisms and contextual factors. 13 This paper focusses on the third domain, which involves the identification of contextual elements that positively or negatively affect implementation and outcomes. The updated MRC guidelines stress the relevance of taking into account the contextual factors associated with variations in implementation, intervention mechanisms and outcomes. 13
Evaluation Sites
The evaluation was conducted in 3 sub-districts implementing the WBOTs in Nkangala District, one of the 3 health districts in Mpumalanga Province, South Africa. The district is rural and the second largest populated district in the province with a population estimated at 1 433 047. The 3 sub-districts were selected on the basis that they had commenced the implementation of the WBOT program in 2012.
Sampling and Data Sources
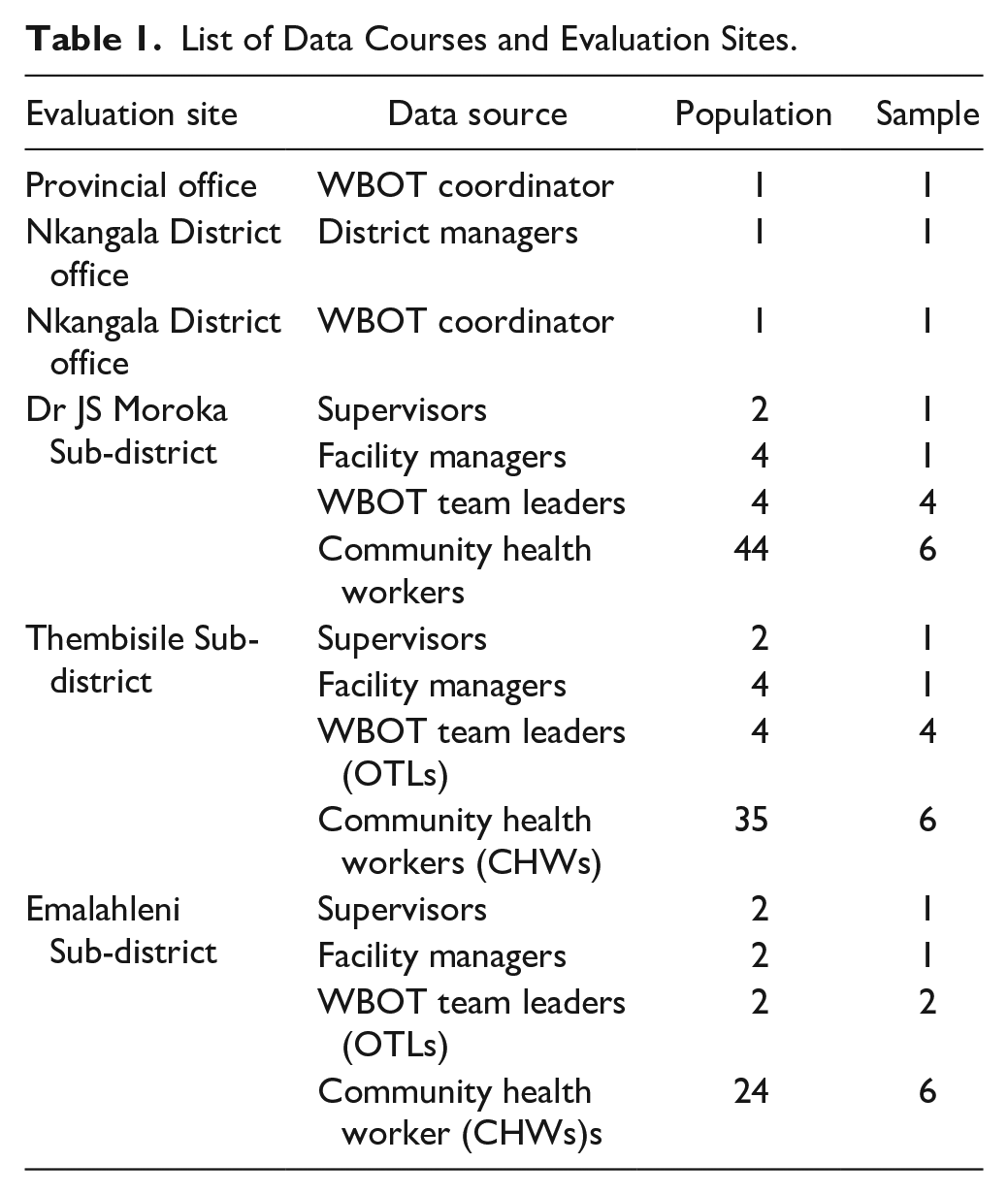
The data sources consisted of healthcare workers involved in the WBOT program and included the provincial and district WBOT coordinators, the District manager, the facility supervisors, the facility managers, the WBOT team leaders, and CHWs. Only those directly involved in the implementation of the WBOT program and who could provide rich answers to the evaluation questions were included in the study (Table 1). The evaluation excluded managers, supervisors, and CHWs who had been performing WBOT-related activities for fewer than 6 months.
List of Data Courses and Evaluation Sites.
Data Collection
Data were collected during November and December 2016 following the receipt of ethics approval from Sefako Makgatho University’s Research and Ethics Committee (SMUREC), the receipt of all relevant permits from Mpumalanga Province Research and Ethics Committee and the support of the management of the Nkangala District. The data collection methods for this evaluation were in-depth interviews (IDIs) with multiple data sources; managers, OTLs, and CHWs to explore the barriers to the implementation of the WBOT program. The interview sites for the provincial and district managers were the district offices, the sub-district offices for the supervisors, and PHC centers for the facility managers, the outreach team leaders (OTLs) and CHWs.
The interviews were conducted by the lead author and trained field workers with experience in qualitative studies. The field workers underwent a day’s training on the evaluation protocol prior to the data collection.
A semi-structured interview guide was developed by the investigators to address 3 components of the process evaluation. To explore the barriers against and the facilitators of the implementation of the WBOT program, the guide addressed the external context in which implementation was taking place, the organizational features, the characteristics of the CHWs involved, and the characteristics of the WBOT program. The CHWs were also asked to make recommendations to mitigate the effects of barriers against implementation.
Digital voice recorders were used to record the interviews, with the consent of the participants. Each interview lasted for about 60 minutes, was conducted in English and the local language. Signed, informed consent was obtained from all participants prior to data collection, and they were assured of the confidentiality and anonymity of the process.
Data Analysis
The interviews were recorded, transcribed verbatim from IsiZulu and Sepedi, later translated into English by the field workers, and then analyzed using the framework analysis approach. Following the researcher’s repeated readings of the transcripts to familiarize herself and to immerse herself in the data, initial codes were identified from the data. A thematic analysis was done and priori themes related to the evaluation research questions and the 4-level framework defined by Lau et al 16 provided a starting point for the development of these codes. After the authors had familiarized themselves with the data and the initial codes had been discussed and agreed upon, all transcripts were coded using the NVivo 11 qualitative data analysis software. 17 The authors held regular meetings to continue discussing the codes in order to develop a shared understanding of them, and to refine and finalize the coding framework. The codes were further discussed and merged into emerging themes, and further themes were added and refined and barriers and facilitators verified.
We triangulated different data sources to enhance the credibility of the data by exploring the perspectives of the CHWs and different categories of health professionals involved in the outreach program. 18 Rigour was further enhanced by using an efficient electronic recorder to facilitate verbatim transcription and thus to ensure that the views of the participants were accurately represented. Data quality checks were conducted during the transcribing of the scripts, the coding, and the development of the themes. The evaluator provided a full description of the context of the evaluation by keeping an audit trail that described all the procedures and processes followed during the conduct of the evaluation. 19
Results
Description of the Study Sample
The evaluation data sources included the provincial WBOT coordinator, the district manager, the district WBOT coordinator, 2 supervisors, 3 facility managers, 11 outreach team leaders (OTLs), and 14 CHWs. The characteristics of the data sources included in the study are shown in the table below. Most were in the age group 30-40 and were female (Table 2).
Characteristics of Data Sources.

Thematic Areas
Themes that were found to influence the implementation of the WBOT program were aligned to the conceptual framework that was developed by Lau et al. 16 The framework emphasizes the importance and inter-dependence of (1) the internal and external implementation context, (2) organizational features, (3) the characteristics of the health care providers involved, and (4) the characteristics of the WBOT program (Figure 2).

Thematic areas based on Lau et al’s conceptual framework.
Organization-Related Factors
Three organization-related themes were found to be barriers to the successful implementation of the WBOT program. These were a lack of policy guidelines for WBOTs, inadequate resources, and a lack of supervision.
Lack of Policy Guidelines for the WBOT Program
The lack of policy guidelines was reported as being a barrier to the implementation of the WBOT program. The supervisors, whose responsibility it is to monitor compliance with prescripts were not sure about the availability of guidelines for the WBOTs. Consequently, some facility managers did not understand the program and were unable to provide supervision and support to the outreach teams.
“There is no policy for the WBOTs from the national level. It’s still drafts; I don’t know when it is going to be approved.” District WBOT Coordinator
“There are no guidelines; I think there is an SOP which was written by the district WBOT.” Supervisor
“The very same operational managers that you are supposed to report to, don’t understand the programme very well.” OTL
Inadequate Resources
OTLs stressed the lack of transport, kit bags, cell phones or airtime, medical equipment, uniforms for CHWs, and workspaces for administrative work. They pointed out that they use their personal phones and airtime to call the CHWs for various work-related reasons. This has a negative impact on their supervisory function and the provision of services to the community they serve. In a similar manner, the lack of airtime affects the work of the CHWs.
“I suffer as a team leader because I have to call them [CHWs] using my own personal airtime. Airtime is a very serious challenge.” OTL
“The CHWs, they do not have kit bags, they do not have uniform and nametags. These are some of the resources that we are short of.” District coordinator
“I wish they could provide more resources for the programme and what we want is for them to give us cell phones and airtime because this thing of doing call backs it’s not working.” CHW
The CHWs reported that they do not have adequate resources and workspace for administrative work.
“We don’t have an office. When we do our stats, we sit outside under the car shelter. Whether it is raining or windy or cold, we sit outside.” CHW
“I need uniform. The one that I am wearing now is embarrassing me. They gave us t-shirts some time ago, but mine is now worn out. They gave us jackets, umbrellas, hats so that we can wear them when it’s hot, but we last had these things in 2013. . ., we did not receive them again.” CHW
The lack of transport was a common barrier to the implementation of the WBOTs. The OTLs indicated that they share transport with OTLs from other wards, which impacts on the smooth running of the outreach services.
“The CHWs are covering a vast area and they are not being supported with transport, because the OTL take them in the morning and drop them off, and they walk to different households.” Facility manager
“Each and every team should have its own transport that is not used for anything. But it must be strictly for the programme.” OTL
Shortage of staff was also identified by OTLs and managers as a barrier to the implementation of the WBOTs. One OTL is responsible for more than 1 outreach team and up to 16 CHWs, when the norm is 1 team and 6 HCWs.
“I have 16 CHW’s. They were scattered all over. I couldn’t meet all of them. My workload was too much.” OTL
“At times when there is a shortage of nurses at the clinic then I will have to leave the outreach duty then get into the clinic and assist there.” OTL
Lack of Supervision
The supervisors indicated that the orientation they had received had not adequately prepared them to conduct WBOT supervisory functions effectively. This lack was viewed negatively by the CHWs, who need supervision to gain the knowledge and clarity required to enable them perform their work adequately.
“Our supervisor does not come to check if we are doing our work properly or if we have problems.” CHW
“If we can be with the supervisor at least once a week, the community can accept us, especially when they see that occasionally we come with nurses. But if a long time passes without the team leader showing up, it does not work out okay. They think we are lying about working with nurses. At least if they come once a week.” CHW
On the other hand, the OTLs feel that they are unable to do supervision due to their involvement in other competing activities such as campaigns. They further reported that some facility managers do not understand the program and therefore are unable to provide supervision and support, whereas supervisors reported that they do not have a supervision tool, adequate training, and enough time to support the outreach team. Facility managers were of the same view. They indicated that they needed guidance and support.
“The campaigns take almost one month. . ., therefore the supervisions - you are not be able to do them.” OTL
“It will be good for us to have a tool for supervising the outreach teams, and also if we can get enough time to support them and also some intensive training.” Supervisor
Characteristics of the WBOT Intervention
The heavy workload of outreach teams, the poorly defined referral protocols, and the poor uptake of the WBOTs were the key intervention-related factors that were identified as influencing the implementation of the WBOTs.
High Workload for Outreach Teams
The CHWs are expected to visit 5 households per day and 25 households per week as part of their key functions in the WBOTs. However, the number of households per CHW increases annually as additional households are established within their wards. This increases the workload of both the OLTs and the CHWs. They therefore perceived the process of registering the households as demanding.
“Each one of us has 250 allocated households, but these households increase yearly as new households are developed.” CHW
“At least each person must have 100 or 150 because 250 households is a lot for us.” CHW
The District managers were of the same view about the workload of the CHWs. They reported that CHWs are over-burdened. Whereas they are supposed to be responsible for 150 households, the reality is that they are required to provide services for more than 200 households.
“They visit the households and cover them, but yooo! It is too much. They are working under a lot of stress and they walk to these households.” Facility manager
“In Emalahleni sub-district there are urban and informal settlements. That is why the CHWs are stretched. . ., you find that they go as far as two hundred households per CHWs because the population is big.” District manager
The problem of the heavy workload is compounded by the fact that CHWs walk to the households, and some are far away. The long distance to households and the number of households CHWs have to visit results in their working for more than 5 hours per day when they are expected to work for only 4 hours.
“The thing that make us to work 6 hours is because we do so many things when we get into that home and you can’t just leave without finishing.” CHW
The OTLs indicated that the high number of CHWs they are allocated made it difficult for them to provide effective supervision. They supervise between 6 and 16 CHWs, which is more than the national norm of 6 CHWs.
“There are 15 CHWs and I must make sure that I do on-site visits [supervision visits]. If the CHW sees 30 patients, I must at least see 10.” OTL
Over and above their high outreach workload, the OTLs have to perform a lot of administrative work, campaigns, school visits, and early child development duties, and clinic-related work. All this influences their ability to implement the program.
“There is a lot of work in admin and admin work, and most of the time they introduce new programmes and all of them come to us as WBOTs.” OTL
The OTLs reported that campaigns take a lot of their time. Sometimes they spend an entire month busy with campaigns, and this affects their outreach and supervision functions negatively.
“The campaigns. . ., they take more time than our outreach duties. They limit the time you spend in the community because a campaign might take a month, meaning that for that month you will not be doing your OTL duties.” OTL
The supervisors and facility managers confirmed that many different tasks are delegated to the OTLs in addition to those in their job descriptions.
“We involve them in many other activities that disturbs their programme.” Supervisor
“Outreach team leaders are also expected to assist in the clinic during busy days or when there is a staffing crisis.” Facility manager
The evaluation discovered that the team did not have Environmental Health Officers as part of the WBOT as outlined in the NDoH guidelines. This leaves the OTLs with the responsibility of conducting environmental assessments outside of their scope of work, and in the process increases their workload.
“Outreach teams should have a health inspector, but we do not have one, and we do our job and that of the environmental health officers and update the health inspector on our findings.” OTL
Poorly Defined Referral Protocols
The relationship with some of the nursing staff in the facilities is not good and makes the work of the CHWs difficult. They indicated that the nurses’ attitudes and ignorance of their referrals makes them feel very discouraged.
“It’s rare for the nurses to give us feedback. . ., there is a back referral that they should fill in, but they don’t do that.” CHW
“They undermine us. They say we are not trained, we don’t know this job and then they ignore us.” CHW
Poor Uptake of WBOTs
The evaluation established that the nature of the WBOT program was a barrier to its uptake. The CHWs reported that some communities associated the WBOT with HIV and felt that having the team in their households was stigmatizing.
“There were households where we were chased away by the sick person. They wanted to know how the Department chose their home out of all the households in the community. They said we come to their house with vans and cause people to watch them and conclude that HIV is in their household. Only out of the whole village, you mean we were the only ones sleeping around. You dare come in here you will know me better.” OTL
The CHWs also indicated that visiting households in the mornings was a barrier to uptake. They reported that some households denied them entry because they felt that it was too early.
“Community members get angry especially in winter because when we start our home visit at 08h00 most people are still sleeping and people sleep all over the house as family members. So we must have the right time for coming to households.” CHW
In addition, the OTLs and CHWs reported that they were denied access to some households; particularly those of white farming communities as well as those of middle class status such as teachers, police officers, and nurses.
“Some community members don’t allow us access to their homes especially in the white farms. This makes it difficult to get access.” OTL
“You know people who have issues are those who are educated. . ., they have an attitude most of the time.” OTL
The CHWs further explained that they are not readily received in households, as they do not have uniforms and nametags as a form of identification.
“You know this thing of going with a nurse; it helps a lot, because they don’t take us seriously with the clothes we are wearing.” CHW
Characteristics of HCWs Involved
The low and irregular pay out of stipends and inadequate training were the key CHWs related barriers to the successful implementation of the WBOTs.
Low and Irregular Stipend Pay-Outs
The evaluation highlighted several frustrations experienced by CHWs regarding the low stipends. In addition to the stipend’s being low, the CHWs reported that the stipends were irregular and not paid out every month. The low stipends caused them a lot of difficulty and affected them and their outreach work on several levels.
“I do not have enough taxi fare to be able to sustain travelling from my home to the office on a daily basis.” CHW
“We use the little money that we have to buy pens to write down whatever is happening in the households that we visit.” CHW
“We sometimes go 9 months without getting a stipend. But when you visit households you must have eaten to protect your body from TB because you don’t know what is happening in the households.” CHW
The OTLs, supervisors, and managers agreed that the payment of stipends for the CHWs was a big challenge and a barrier against the successful implementation of the WBOTs.
“Sometimes our CHWs can spend five to six months not being paid. . . It also affects us in terms of reports. They don’t produce reports because they will tell you that we are hungry we can’t go to work while we are hungry.” OTL
Inadequate Training
Most of the CHWs had undergone Phase 2 training; however, they felt that the training they had received was inadequate. This was echoed by the OTLs, the managers and the supervisors, who felt that the CHWs are not adequately trained.
“The two weeks training is not enough for them, so I don’t know - I would recommend that they extend the period of training, because it is only for two weeks to cover all those modules.” OTL
“The training that they were given, it assisted in a way, but one does not need to relax and say they’ve got enough information. As an OTL you need to keep on in-servicing them, supervise them, and see if they doing things correctly, they giving the right information.” OTL
The OTLs further indicated that because of the inadequate training it was not easy to work with the CHWs. They mentioned it was difficult for the CHWs to carry out certain tasks, as it took a long time for them to understand instructions.
“When you work with the CHWs it’s a little bit hard because their thinking is different. They don’t think like us. I don’t know how to explain them. If you say to them ‘Let’s try this, let’s do that’, they take time.” OTL
The External Context in Which WBOT is Taking Place
Safety threats against the outreach teams and the community cultural beliefs and practices were identified as the most common barriers against the uptake and implementation of the WBOTs.
Safety Threats
The evaluation showed that the CHWs work under conditions that put them at risk of physical and emotional harm.
“They risk their lives you know. . . It’s not safe in the communities where they work. That is why we pair them. . . Most of the time they go two by two or three.” District manager
“We advise the CHWs not to get in households where there is a patient who is mentally ill alone, but they must go in there being two.” OTL
The risk of contracting communicable diseases when performing their work was raised, and the fear evoked by the risk of harm affects the implementation of the WBOT program.
“I feel that I am a victim, when I go to a household and there is a patient with MDR TB, and because I work on an empty stomach, I am hungry and struggling.” CHW
The CHWs suggested that the department should provide them with adequate protective equipment and provide policies regarding their health in case they contract any of the prevalent diseases.
“We need to have protective clothing in case an accident happens while you are bathing a patient.” CHW
Widespread substance abuse is a major concern for the CHWs and OTLs and has a negative impact on the implementation of the WBOTs.
“Nyaope [a novel drug] has destroyed our community. We try our best but we are scared to enter households where we see them sitting in groups and smoking. We don’t feel safe because we might be raped.” CHW
“We go in pairs when we enter households. We find it difficult to enter the house because of the Nyaope [a novel drug] addicts.” CHW
Cultural Beliefs and Practices
The evaluation revealed some cultural practices and beliefs that are considered barriers against the implementation of the WBOT program. For example, the popularly held belief that when people are ill they have been bewitched was commonly identified as a barrier against the uptake of WBOT services.
“When a person has diabetes, they say he/she is bewitched and when a person has HIV/AIDS they say he/she is cursed by ancestors and they don’t allow him/her to take treatment.” CHW
Discussion
In this paper, a process evaluation approach was used to examine and describe the contextual, organizational, health provider, and program related barriers considered to affect the implementation of the WBOT program in the first 6 outreach teams established in 2012 in 1 district of Mpumalanga Province, South Africa. A fundamental barrier revealed by the evaluation was the lack of a dedicated budget allocated for the WBOTs at district and sub-district level. The poor funding of the outreach teams has a negative impact on the implementation of the program because sub-districts cannot supply the outreach teams with the resources that they need in order to be able to perform their functions. Similarly, evaluations of the WBOTs conducted in other provinces of South Africa found that no specific budget was set aside for the WBOTs.11,20-23
The lack of an adequate budget resulted in shortages of equipment, supplies, transport and human resources, and acted as a barrier against the successful implementation of the WBOTs. 20 In many instances, the outreach teams were not able to conclude the services provided to the households due to a lack of resources. Similar observations were reported in rapid assessments of the WBOTS in other provinces.11,24 For OTLs, the lack of transport affected their ability to visit households for supervision. Although 69 outreach teams have been established in the district, only 20 vehicles have been allocated to them. When a vehicle is not available for OTLs, they are unable to carry out household visits and clients are not able to receive outreach services. The lack of transport for OTLs results in poor supervision of CHWs and undermines the efforts to implement the WBOTs. 25
The evaluation showed that the OTLs’ workload was demanding since they had to find a balance between their administrative activities, their supervision of household visits, and their clinic work. The outreach services are hindered when there is a shortage of staff in the clinics from which the OTLs were recruited. Since the WBOT is attached to a clinic, the difficulty in recruiting professional nurses to lead outreach teams and the severe shortage of staff in the clinics hinder the OTLs’ outreach activities. The OTLs are compelled to perform clinical work because the clinic takes priority over their OTL outreach duties. This is particularly prevalent in facilities where the facility managers are not up to date with the functions of the outreach team and insist that OTLs prioritize their clinic services. In an earlier rapid appraisal of WBOT programs in South Africa Marcus et al 26 reported that when OTLs are faced with a choice of clinical and outreach services they are inclined to prioritize clinic work at the expense of outreach activities. Given the high turnover of staff in rural clinics, prioritizing clinic duties is common, suggesting that the implementation of the outreach programs is often negatively affected.
The high number of CHWs allocated to OTLs is contrary to the National guidelines. OTLs in other studies reported being unable to support CHWs adequately as a result of their excessively high workloads. 27 The evaluation established that the supervision of outreach teams was inconsistent and inadequate and compromised the ability of CHWs to perform their duties.23,28,29 OTLs’ planned house visits with the CHWs were hampered by the lack of transport, which affected the actual supervision session with the CHWs. In addition, the expectation that the OTLs work in clinics as well as in the community outreach program short-changes the WBOT program and leaves the CHWs under-supervised.20,26 Staff shortages and competing demands on supervisors’ time contribute to implementation failure for outreach teams. 30 The problem of the heavy workload is likely to persist because of the difficulty in recruiting professional nurses to lead outreach teams 20 and the expectation that those working in the outreach program should also work in the clinics.
According to the National guidelines, facility managers are expected to supervise OTLs, but research suggests that their support is generally lacking.20,31 Some of them felt that the WBOT was an added burden, that their roles were not clearly defined, and that there was a lack of specific tools and guidelines on the provision of supervision.11,20,31 The poor support and supervision of the outreach teams from senior managers is among the key challenges that hinder the implementation of the WBOTs. 32 The quality of the supervision of CHWs affects the performance of the outreach teams.33,34 Evidence from an assessment of WBOTs in 5 provinces in South Africa reveals that the facility managers were unable to provide effective supervision to OTLs because the clinics were under-resourced and underperforming. 35 It is important that facility managers should be adequately prepared and supported to fulfill their supervisory and support role. 31
Like that of the OTLs, the workloads of the CHWs were exceptionally heavy. Whereas they are expected to visit 5 households per day, they do much more despite the lack of resources, the poor training, the difficult working conditions, and the suboptimal supervision.22,27,31,36 CHWs spend a lot of time walking from 1 house to another, and they are affected by the sun or the rain, as they lack protective clothing. 37 In addition to their outreach activities, they conduct campaigns, assist in immunization, and deliver pre-packed medicines for chronic clients. CHWs therefore cannot visit the allocated number of households as these activities take them out of their routine of household visits. This suggests that the high workload of the CHWs has a negative impact on the implementation of the WBOTs. Similarly, in Limpopo Province of South Africa the workload of CHWs was found to be much higher than at the inception of the program, as they visit more households than they used to and offer more services than the stipulated norm. 25
The evaluation showed significant gaps in the referral of clients from the outreach teams to the next level of care. CHWs seldom received feedback from the referral sites on the clients that they referred. The nurses in the clinics often ignored their referral letters. Challenges with referrals were similarly reported in other studies.20,32 Similar observations that CHWs struggled to make referrals and experienced dismissive attitudes from clinical staff were reported in an Ethiopian outreach program. 35 The poorly defined system of referrals between the CHWs and other sectors affects the outreach services. Non-acceptance of referrals from CHWs by other sectors and the inability of the referral site to assist clients creates a lack of confidence in the outreach teams among the members of the community. Additionally, CHWs find it difficult to refer clients to clinics when the clients need to be transported, given the poor ambulance services in rural districts. This has a negative effect on how the communities perceive the WBOT program and their trust that the program will serve their needs.
CHWs were dissatisfied with and demotivated by the irregular payment of their stipends, and the inadequacy of the payments. Inadequate remuneration for CHWs is reported in other studies.27,29 The irregular payment of the stipend has a huge impact on the quality of the outreach services. In addition, the CHWs’ morale, self-confidence, and credibility in the community were negatively affected by their lack of uniforms, which hinders the performance of their outreach duties. 37 The evaluation learned that during the long period when the CHWs did not receive their stipends, the implementation of the WBOT was compromised because the CHWs did not submit reports.
Moreover, the CHWs use their own funds to pay for transport to reach households they cannot access on foot.27,37 Since the taxi fare is at their own cost, the lack of a stipend affects the implementation of the WBOTs, as the CHWs are unable to meet the minimum required number of allocated households. The lack of dedicated workspaces in clinics for the outreach teams to do administrative work puts a damper on their morale because they have to work under the trees to compile their weekly and monthly reports. 20 The fact that supervision is not consistently performed and CHWs often cannot reach the OTLs when they encounter a challenge affects their morale and credibility in the community.33,34 The literature suggests that CHWs derive important motivation from various non-financial incentives such as uniforms, nametags, and certificates. 29
The working conditions of CHWs expose them to risks of contracting communicable diseases and to threats to their safety which deter them from visiting some communities. The threats of violence and of being mugged put a strain on the resources allocated to the outreach teams because CHWs feel unsafe to visit households alone, and have to work in pairs. The implication is that instead of the 2 CHWs visiting 50 households each a week, as stipulated, when working as a pair they can see only 25 households. The concerns about the health, security, and safety of CHWs are well founded, since violence and crime are realities in South Africa, and most CHWs are female and therefore particularly vulnerable.20,32,38 The threat to their wellbeing is compounded by the various forms of resistant TB prevalent in the communities.
The participants highlighted that despite extensive community consultation not all households were open to the program. Munshi et al 23 attribute resistance to the uptake of the WBOTs to a lack of awareness about the outreach teams in the community. Race, religion, and middle class status were barriers against the uptake of the program in this evaluation, as in others. 20 Other community-related issues such as stigma, cultural beliefs, and practices were also barriers against the uptake of the outreach program. The stigma attached to TB and HIV makes communities weary of being associated with the outreach teams. In other studies, the fear of being stigmatized was raised by some participants as a barrier against the implementation of the outreach program.27,37
CHWs could not enter some households if they did not cover their head with a doek/head scarf, if they wore pants, or if they were females and had to tend to a male client, and some families would not agree to the referral of their sick to the clinic because they associated the disease with witchcraft. The cultural context of a district in Limpopo Province also presented a barrier against the implementation of the outreach progamme. 27 It is of concern that in some households, children had not been immunized and pregnant women had not attended antenatal care because the households do not believe in western medicine.
Conclusions and Recommendations
This evaluation has identified the barriers against the implementation of WBOTs and provided a clear indication of the status of the WBOT program in Nkangala District. The key critical barriers identified by the evaluation include the inadequate provision of resources, the lack of supervision, the heavy workload, the inadequate and irregular payment of stipends, threats to the safety of the CHWs, and the cultural beliefs and practices of the communities who are to receive the services.
Although the barriers are reported as separate contextual factors, the internal and external contexts are interdependent, interact with one another, and should not be considered in isolation. The need to improve stakeholder engagement and orientation on the WBOT program underscores the importance of the external context in the successful implementation of WBOTs.
The lack of adequate financial resources was the main challenge, and will continue to pose a risk to the successful implementation of the WBOTs. The lack of money affects both the quality and the quantity of the services offered by the outreach teams. It is recommended that there should be a dedicated budget allocation for the WBOTs, that it should be bolstered, and that it should be ring-fenced.
Adequate resourcing of WBOTs and adequate and regular remuneration of CHWs are critical for the sustainability of the WBOTs. The current evaluation supports the call for the formalization and absorption of CHWs into the health system in order to address the problems with their remuneration, training, and role clarification. Well-trained and adequately supervised CHWs will improve the quality of the outreach services and the implementation of the WBOTs.
One of the key external contexts that influence the implementation of the WBOTs is the threat to the safety of the CHWs. There is a need to formalize the pairing of CHWs and the recruitment of male CHWs to address the safety issue. Recruiting male CHWs would also amount to a response to the need to be culturally sensitive to the gender norms and needs of male preferences to be cared for by male HCWs.
The evaluation established that the supervision of CHWs and OTLs appears to be compromised more by the heavy workload of the supervisors than by other contextual factors. It is recommended that the NDoH should consider appointing OTLs who will spend their time fully dedicated to the WBOT program. Furthermore, it is necessary to regulate or standardize the OTL-to-CHW ratio, taking into consideration the geographic area the CHWs serve. Over and above the heavy workload, the transport constraints affect the supervision sessions with the HCWs.
Lastly, the workload and scope of the CHWs should be reviewed, taking into consideration the physically demanding and time-consuming nature of the activities performed by the CHWs to ensure the delivery of good quality WBOT services.
Footnotes
Acknowledgements
The authors would like to thank the outreach team and the community who willingly participated in the evaluation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and consent to participate
Approval was obtained from Sefako Makgatho University’s Research and Ethics Committee (SMUREC/H/157/2016: PG), Mpumalanga Province Research and Ethics Committee (MPHREC) and the support of the management of the Nkangala District was given.
Availability of Data and Resources
All data used in the study are available from the lead author on request