
Abstract
Introduction/Objective:
Community health workers (CHWs) can play a vital role in many aspects of healthcare, particularly for underserved communities, but it is unclear what factors are most important in determining the success of CHW-based programs. We wanted to assess what factors contribute to the effectiveness of CHWs in a smoking cessation program.
Methods:
We trained CHWs in 3 areas regarding smoking cessation: knowledge, attitude, and practice (KAP). The training program utilized the 5A’s as approach. CHWs actively sought out people addicted to cigarettes to participate. Patients received support from CHWs and a team of medical professionals for a year. At the conclusion of the program, focus group discussions with a group of CHWs, a group of patients, and a group of medical professionals were conducted.
Results:
On average, patients reduced their cigarettes/day by 7.2% and 29% of patients were completely cigarette free at a 1-year follow-up. Patients marginally decreased exhalation CO levels and increased lung capacity. CHWs gained a good understanding of health risks associated with smoking and common methods to help quit. Their attitude became more sympathetic and caring. CHWs exhibited patient-specific solutions to help with smoking cessation and actively sought out people to participate in the smoking cessation program.
Conclusions:
A smoking cessation program combining CHWs and pharmacists was effective. Key factors were having CHWs that are respected and established in their communities, using CHWs who know their patients and can provide individually tailored solutions, and empowering CHWs with intensive training.
Introduction
Smoking cessation is an important public health goal because smoking is a risk factor for many Non-Communicable diseases (NCDs). In Thailand, 17.9% of adults are current tobacco users. 1 Each year 50 000 people in Thailand die of smoking-related diseases, and approximately 1.0 million people are sick or disabled with serious chronic diseases from smoking. 2 Although pharmacist interventions have been shown to help, these programs have not been widely adopted.3-8 Patients often miss follow-ups. Staffing is inadequate. Pharmacists do not have enough time. And perhaps most importantly, very few people request smoking cessation services in the first place. 9
A cheap and effective addition to pharmacist care may be programs involving community health workers (CHWs). CHWs have sometimes been found to improve the effectiveness of smoking cessation programs. 10 However, as is true of the overall literature on CHWs, individual studies have reported mixed results. Some programs yield no improvement in quit rates with CHWs, 11 but others have found dramatic improvement with quit rates of as high as 26%. 12 The specific characteristics of CHWs may play an important role, but what characteristics matter and how these characteristics impact the ultimate goal of smoking cessation remains unclear.
We created a community smoking cessation program involving pharmacists and CHWs. We report quantitative evidence of the program’s success. In addition, we conducted a series of focus group discussions with pharmacists, CHWs, and patients to assess which factors were most important. The main lessons learned and recommendations for the implementation of future programs are discussed.
Method
Setting
This study was conducted in a rural community in Phayao province in Northern Thailand. All methods were approved by the Institutional Review Board at the University of Phayao.
Smoking Cessation Program
CHWs were recruited from 11 villages. There were 3 volunteers from each village for a total of 33 CHWs. All CHWs participated in 4 seminars led by pharmacist (the third author) During these training sessions, we focused on knowledge, attitudes, and practice (KAP).
Knowledge training focused on teaching CHWs about the harms of smoking, laws regulating the sale and access to cigarettes, and various techniques that have been found effective for helping people quit smoking. Attitude training focused on making people more open minded to helping others. The goal was to make CHWs more willing to offer help to potential patients. We also addressed some misconceptions that CHWs might have had about people who smoke. Practice training utilized the 5A’s model 13 and involved integration of CHWs with pharmacists and the Sub-district health promoting hospital (SHPH) staff. First, CHWs (A)sked potential patients about their smoking habits and health history. Second, CHWs (A)dvised potential patients about how to quit smoking and told them about available resources in the community. Third, CHWs coordinated with pharmacists so that patients could be scheduled for (A)ssessment in the clinic. Fourth, pharmacists (A)ssisted patients in their efforts to quit smoking by providing treatment as needed (eg, medicine, nicotine replacement therapy, counseling etc). Fifth, pharmacists and CHWs coordinated to (A)rrange follow-up treatment to ensure their success, see Supplemental Appendix file for Smoking cessation program.
After training, CHWs announced the program to their villages. Each volunteer had a group of houses that they were responsible for. They announced that smoking is not healthy and offered that there was a smoking cessation program at SHPH. In addition to general announcements, CHWs invited individual people who smoked one by one.
At SHPH, the program was facilitated by 2 pharmacists (the first and third authors) and SHPH staff. CHWs coordinated with SHPH staff and patients to facilitate patient assessments. In total, 42 patients joined the program.
After initial assessment and assistance from pharmacists and SHPH staff, CHWs arranged follow ups with patients and checked in with them at least once a month. Because volunteers all lived near their recruited patients, they were able to give patients constant encouragement at home. Specifically, CHWs saw patients at local markets and in the street. They could enquire frequently after patients’ health and progress with smoking cessation. Finally, CHWs facilitated final follow-up appointments with patients after 12 months.
At baseline and follow up appointments, patients reported their average number of daily cigarettes. In addition, we measured carbon monoxide (CO) and percentage of peak expiratory flow rate (%PEFR). Patients were given 7 opportunities for follow up appointments with the pharmacist. These follow up appointments occurred at 1 week, 2 weeks, 1 month, 2 months, 4 months, 6 months, and 1 year.
Data Analysis
Descriptive statistics were computed for all study variables. One-way within subjects ANOVA was used to test for changes in cigarettes per day between the baseline, 6 month, and 1 year time points. Due to incomplete follow-up data, changes in CO concentration and %PEFR were assessed using within samples t-tests comparing baseline to 1-year follow-up only. Formal analysis and figure generation were conducted using custom written code in R.
Qualitative Assessment
Qualitative assessment was based on 3 focus group discussions (total n = 21). The first had 11 CHWs, 1 from each village. The second group had 8 patients. The final group was 1 pharmacist and 1 nurse from SHPH, who both took part in the smoking cessation program. Focus group discussions took place after all follow ups.
The first author and an outside consultant moderated our focus groups. Our moderator was an experienced smoking cessation councilor in the community.
The moderator’s guide materials were co-written by members of the research team (the first and third authors) to provide a semi-structured framework for discussion. We asked open-ended questions and used extensive probing to explore topics relevant to the community. The 3 main topics were (1) what knowledge did you get from the program; (2) what attitude change did you have after participating in the program; and (3) what was your experience when practicing in the community? Most of the questions were the same in each interview, while the follow-up questions varied as the focus group moderator followed the flow of the group discussion.
All focus-group interviews were in a central location for all participants and lasted about 90 minutes. Data collection took place between April 2019 and March 2020.
We followed generally accepted guidelines for thematic analysis. 14 Finally, participants were given an opportunity to comment on conclusions to ensure that nothing had been misinterpreted.
Results
Quantitative Results
Table 1 shows the baseline characteristics for the 42 patients in the smoking cessation program. Median age was 62 years (IQR 57-67). 95.2% smoked ≤ 20 cigarettes per day. 52.4% of patients exhibited medium level nicotine dependence (Fagerstrom score 4-6),15,16 64.3% of them listed family as their primary reason to quit smoking.
Baseline Characteristics of Patients in Smoking Cessation Program.
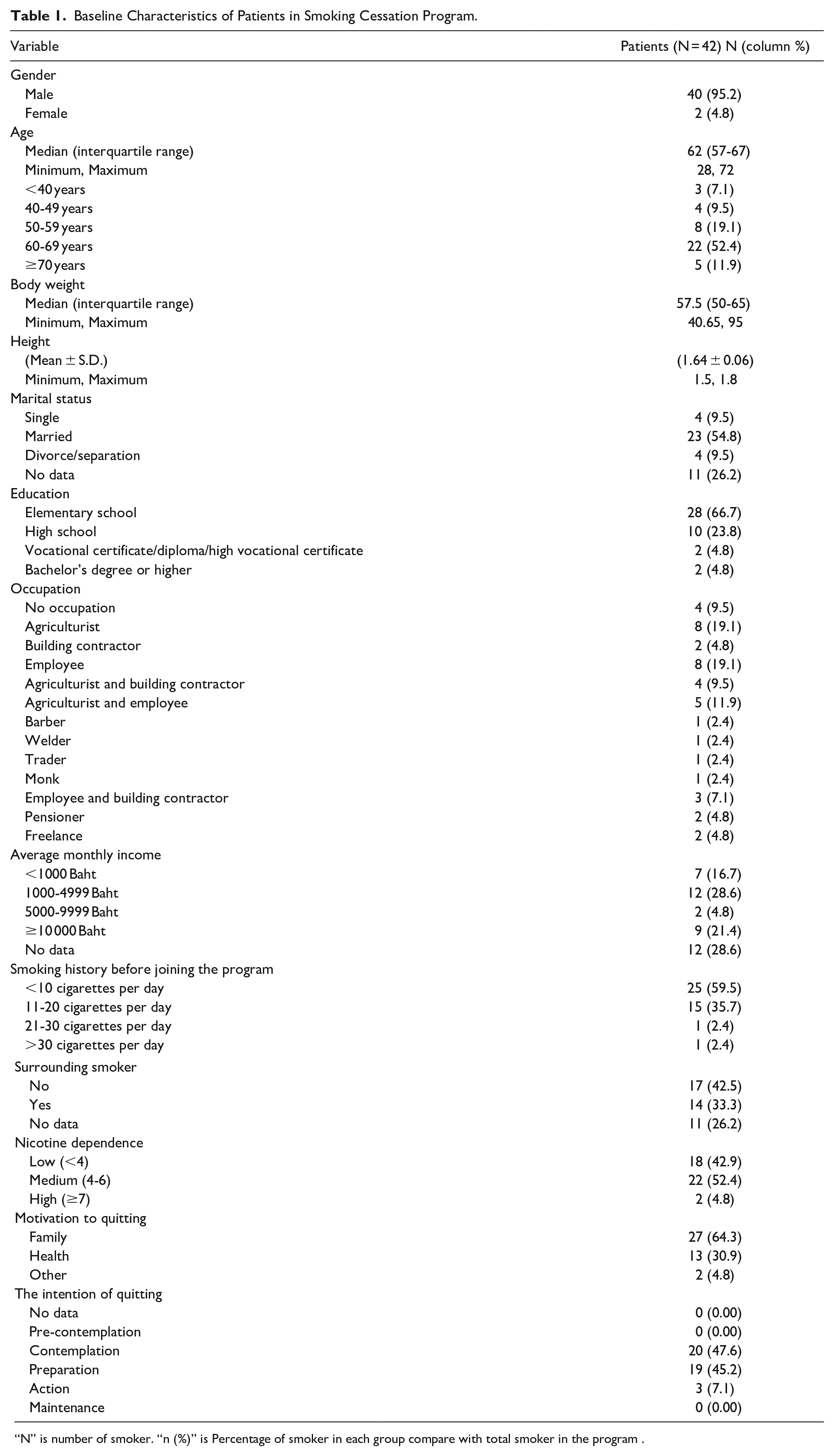
“N” is number of smoker. “n (%)” is Percentage of smoker in each group compare with total smoker in the program .
Table 2 shows key statistics gathered at follow-up appointments. 34/42 (81%) patients were available for 12-month follow-up. There were 12 (28.6%) patients who had quit smoking, and 17 (40.4%) who decreased the number of cigarettes smoked per day.
Abstinence Rate at 6 and 12 Months.

Within subjects ANOVA revealed that there was a significant reduction in cigarettes smoked per day (F(2,60) = 25.6; P < .0001; Figure 1). There was a reduction of 7.2 cigarettes/day between the baseline and 6-month follow-up (t(27) = 4.9; P < .0001; 95% CI: [4.2, 10.3 cig/day]) but no additional decrease at the 12-month follow-up (P > .2). There was a marginal reduction in CO in patients’ breath (t(21) = 2.0; P = .055; 95% CI: [−2.2, 0.03 ppm]; Figure 2), and this was marginally correlated with patients’ reduction in cigarettes/day (F(1,21) = 4.08; P = .056; R2adj = .12). We also observed a marginal increase in lung capacity as measured by PEFR (t(23) = 2.0; P = .055; 95% CI: [−0.6, 55.2 L/min]; Figure 3), but this was not associated with patients’ reduction in cigarettes/day (P > .2).
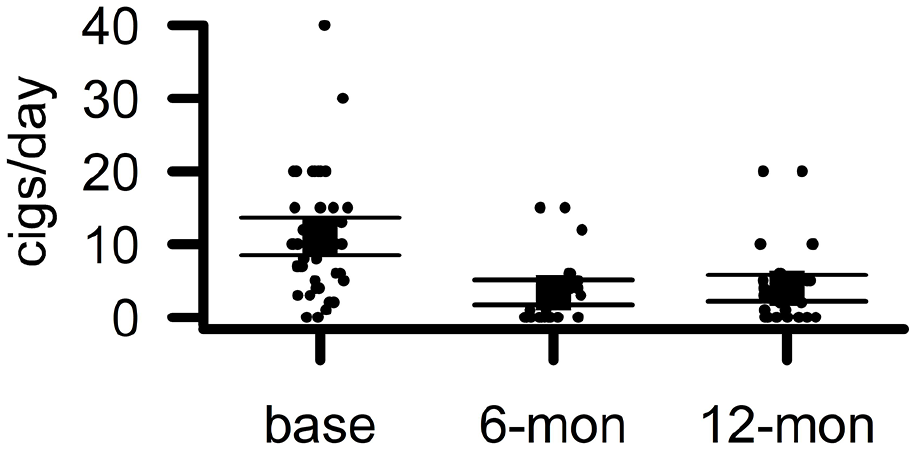
Patients reduced the number of cigarettes they smoked per day. The y-axis displays the number of cigarettes that patients reported smoking per day (cigs/day). The x-axis displays the time at which measurements were taken (base = baseline, 6-mon = follow up at 6 months, 12-mon = follow up at 12 months). Points indicate individual patients. Boxes indicate group means. Error bars indicate 95% confidence intervals.

Carbon monoxide in patients’ breath reduced. (A) The y-axis displays the concentration of carbon monoxide in parts per million (CO (ppm)). The x-axis displays the time at which measurements were taken (base = baseline, 12m = follow up at 12 months). Dashed lines link the measurements for individual patients. (B) The y-axis displays the difference scores for CO ppm with negative numbers indicating a reduction in CO ppm and positive numbers indicating an increase. The 12m—base abbreviation stands for follow up at 12 months minus baseline. Dots indicate individual patients. In both panels, boxes indicate group means and error bars indicate 95% confidence intervals.
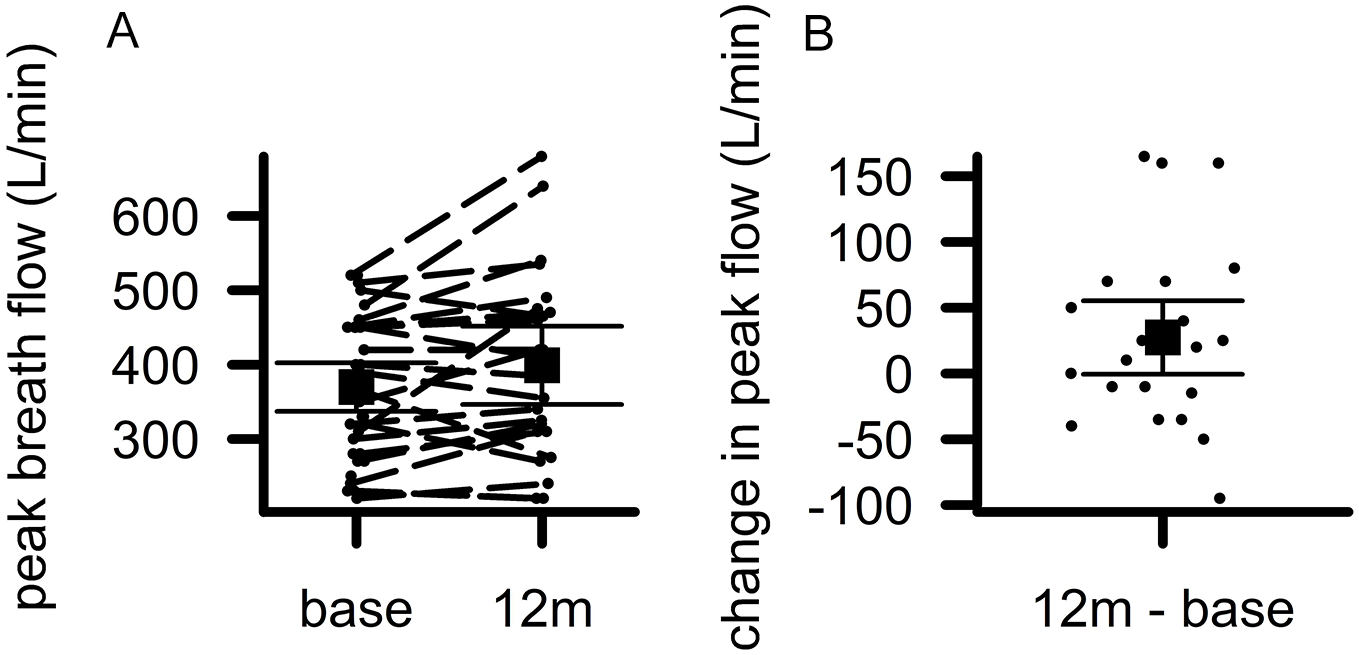
Patients’ lung capacity increased. (A) The y-axis displays patients’ lung capacity measured as the peak flow measured during exhalation in units of liters per minute (peak breath flow (L/min)). The x-axis displays the time at which measurements were taken (base = baseline, 12m = follow up at 12 months). Dashed lines link the measurements for individual patients. (B) The y-axis displays the difference scores for peak breath flow L/min with positive numbers indicating increased lung capacity and negative numbers indicating reduced lung capacity. The 12m—base abbreviation stands for follow up at 12 months minus baseline. Dots indicate individual patients. In both panels, boxes indicate group means and error bars indicate 95% confidence intervals.
Qualitative Results
The characteristics of participants in the focus group discussions are presented in Table 3. Qualitative analysis of conversation transcripts revealed 3 main categories of information with several subthemes in each category. The following highlights some of the general opinions that came up repeatedly in these discussions as well as specific quotes emphasizing main points.
Characteristics of Participants in Focus Group Discussions.
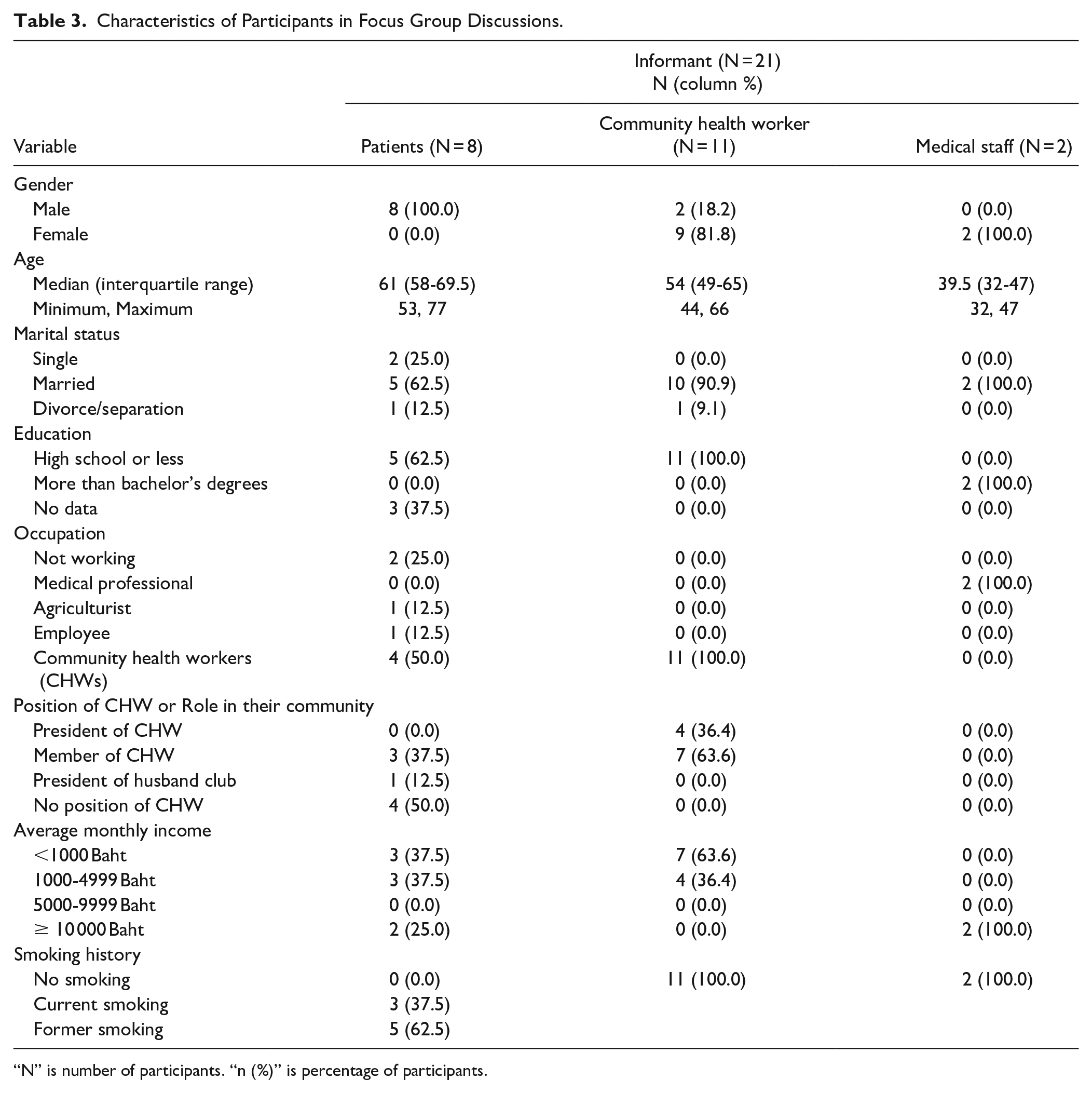
“N” is number of participants. “n (%)” is percentage of participants.
Knowledge
After participating in the program, CHWs reported more knowledge of the health effects of smoking, laws regulating sale and access to cigarettes, and various techniques that have been found effective for helping people quit smoking. They also reported feeling more confidence in their actions to help people quit smoking.
N “I have this technique from the (program) teacher. I knew before that sourness can reduce craving to smoke but I didn’t know how to use that. The teacher taught me that to use a lemon you have to slice both the rind and the flesh, slice them into bite sized, thin pieces and then put them in a bag. When using, chew slowly in your mouth. . .Keep doing this until the lemon is completely dissolved. . .It helps smokers reduced cravings to smoke better than just putting it in the mouth.”
C “After listening to the teacher saying that cigarettes contain a lot of toxic substances. The smell of cigarette smoke also gets stuck on clothes. Now, my neighbors are raising a child the same age as mine. I want to ask him to quit smoking. But he still does not want to quit now. So I went to talk with his wife to inform his wife that cigarette smoke can track in on smokers’ clothing and skin. Then spread to children. . .Therefore, after smoking you should wash your hands, take a shower and change your clothes before hugging or kissing [your children]. I used to invite smokers to quit smoking. He said, gradually he would reduce the amount of smoke, because he has been smoking for a long time since he was a teen. . ..So I told him to gradually reduce it from 6 cigarettes, it was reduced to be 3 or 2.”
Attitude
CHWs only advised people to quit smoking, but they did not care if people quit or not. CHWs often developed negative attitudes toward patients who failed to quit smoking. After the attitude adjustment process, CHWs had positive attitudes towards patients. They wanted to help people to quit smoking and reduce the impact of secondhand smoke. Patients became aware of the goodwill of the volunteers.
N “After joining the program, they (CHWs) have a more positive attitude. Before this, they never cared about people who smoke. Now, when I told them to follow up with patients. They were delighted and always asked me, how to talk with patients that they want to help to quit.”
C “I asked patients to quit smoking because I pity them, especially because of how secondhand smoke affects their family. Although they may not listen, but I would like to make them quit. I wanted to help them.”
Practice
The CHWs were more confident persuading people to quit smoking. They became more persistent. In addition, they were able to extend healthcare coverage directly to the patients in their local communities. They provided knowledge about the harms of smoking and encouraged people to participate in smoking cessation services. In some cases, volunteers also helped by driving people to SHPH for pharmacy consulting. CHWs compiled lists of people who smoke and gave them advice in the community. They tailored their approach to the economic, family, and health of each patient. In addition, volunteers who smoked tried to quit smoking themselves to be a role model.
C “For me, at first I asked them to quit and they didn’t quit. I thought, let they smoke until death. Because I don’t know how to invite. After I get knowledge from the teacher, I known the techniques to persuade and encourage smokers to quit. I persuaded him by using the cardiovascular disease of his family as his motivation for quitting. In the end, he agreed to come out and smoke outside the house to reduce secondhand smoke. I also raised money issue as his motivation.”
C “My process was different from others because my house is close to the smoker’s house, and he does not want to go by himself. I always pick him up to go to the SHPH for smoking cessation clinic. I intended to help him quit smoking. I pity him and his family. Though, he refused our service before, I still invite and persuade him.”
C “He is a CHW, if he wants to invite others to quit smoking, he should be a role model to others. The CHWs are a leader in health. It will not look good, if he smokes.”
C “In case the smoker does not want to quit, I always say that his wife and all family members will be impacted from his smoking. There is 1 person who won’t quit. I invited many times, he did not give up. However, I don’t get discouraged until he agrees to quit smoking.”
P “After I followed up with patients, I found some had no mobile phones. I couldn’t contact these patients. So, I followed up through CHWs. (talked with smoker via CHW’s mobile phone and/or if I cannot contact directly then CHWs would follow up with patients, then report data to pharmacist). The CHWs reported results of cessation performance by themselves.”
Discussion
This study demonstrated that a smoking cessation program using CHWs was successful at helping patients quit smoking. The number of cigarettes smoked per day was reduced by an average of 7.2 cigarettes across all patients, and 29% of patients were completely cigarette free at a 1-year follow-up. This value was calculated with the conservative assumption that all patients lost to follow up were still smoking. Without this assumption, if our quit rate were calculated based only on patients who were available for follow up then it would be 35% (12/34). Patients also exhibited a marginal decrease in exhalation CO levels and a marginal increase in lung capacity, providing verification of patients’ cigarette smoking self-reports. The rate of smoking cessation observed in our sample was much higher than has been observed for unassisted smoking cessation,4,17 and was also better than has been observed in many random controlled trials of various smoking cessation interventions. 18 The present study dramatically outperformed the 2% to 3% success rate expected in the WHO Toolkit for delivering the 5A’s and 5R’s brief tobacco interventions in primary care. 13 The present result also compares favorably with comparable approaches involving pharmacists but not CHWs. 19 Our results replicate those found for a CHW-based program carried out in Vietnam where smoking cessation at a 6-month follow-up was 26% for patients who received support from CHWs. 12
In focus group discussions, across the categories of knowledge, attitude, and practice, a common theme was that CHWs were empowered by the program to become more confident and effective. They felt they gained a good understanding of health risks associated with smoking and common methods to help quit. Their attitude towards people dealing with smoking addiction was changed to allow them to become more sympathetic and caring, and they became persistent in their efforts to convince people to stop smoking. This empowerment led to many unique solutions that were tailored to individual patients. For example, a CHW persuaded a patient to quit smoking by reminding him of his individual family history of cardiovascular disease. Another CHW found out that a patient lacked transportation and began driving him to his appointments.
A major success factor in this study was the well-developed role of CHWs in Thailand. In Thailand, CHWs, known as village health volunteers, was a person who has been selected by the villagers in each group of houses and has been trained according to the curriculum prescribed by the Ministry of Public Health. They play an important role as a leader in health behavior change, health promotion surveillance and disease prevention, first aid and treatment, referral of patients to rehabilitation services, and consumer protection for health. They get remuneration about 1000 baht per month from the Ministry of Public Health. 20 CHWs have been effective in many past public health initiatives.21-23 CHWs currently provide coverage to over 12 million households throughout Thailand. 24 Because of this track record of success, CHWs are recognized as respected leaders in their local communities. Their position gives them knowledge of potential patients that can be critical in bringing care into the community. This is particularly important in programs where potential patients may not consider themselves to be patients. For example, in the current study, only 7% of our patients were actively attempting to quit smoking at baseline.
Having pre-established CHW programs may be of central importance. In a previous meta-analysis of smoking cessation programs with and without CHWs, only 1 study out of 5 demonstrated a large effect of CHWs. 10 That study had CHWs who were already established in the community when the smoking cessation program was implemented. 12 In general, survey results indicate that factors such as prestige and respect are among those that determine the success of CHWs, and these factors likely take time to build. 25
Thus, a key issue for future projects will be how to develop effective CHW programs. Replicating the CHW program in Thailand will require large-scale government action. In Thailand, CHWs are chosen by their neighbors, giving them immediate local legitimacy. In addition, CHWs generally reflect the spiritual and socioeconomic norms of their areas, which may contribute to the trust they enjoy in their communities. Interestingly, we observed that in our study CHWs tended to be female, but patients tended to be male. In our hands, this did not seem to matter, but future research may benefit from more careful consideration of concordance/discordance between CHWs and the patients they serve. They were trained in a program developed by the Ministry of Public Health, providing baseline medical knowledge to help improve public health. They are paid 1000 baht per month, which in many parts of Thailand amounts to 10% to 20% of typical full-time earnings. 20
This study also has some limitations. First, due to the self-selection of patients, it is likely that motivation to quit was higher in our patients than in the general population. Future studies should consider an active control condition with patients drawn randomly from a single self-selected pool. Second, our patients tended to be older than is typically reported in surveys of smoking prevalence in our region. 26 We believe this was because older patients had more free time to devote to participate in our program. Future studies could provide more flexible schedule options to help address this recruitment bias. Third, 19% of patients were lost to final follow-up. Although this is lower than has sometimes been observed (eg, 40% follow-up loss in) 27 future studies should examine more critically why attrition rates are often high in smoking cessation studies. Fourth, future studies could improve causal inference through the use of a cluster randomized design. Fifth, the impact of CHWs in our study depended on personal connections. Although this was likely a great strength of the program, it is also a source of variability, making interpretation more difficult.
Conclusions
A smoking cessation program combining CHWs and pharmacists was effective. Key factors were empowering CHWs to bring patient-specific care direct to the patients, and recruiting respected, established CHWs within the communities where they worked. We suggest that organizing community-specific teams including CHWs to help with smoking cessation will lead to lower rates of smoking and better public health.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211048363 – Supplemental material for Community Health Workers Improve Smoking Cessation When They Recruit Patients in Their Home Villages
Supplemental material, sj-docx-1-jpc-10.1177_21501327211048363 for Community Health Workers Improve Smoking Cessation When They Recruit Patients in Their Home Villages by Adinat Umnuaypornlert, Adam J. O. Dede and Sudarat Pangtri in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
Special thanks to Thailand Health Promotion Smoke Free Pharmacy Network in Community Pharmacy Foundation and Thai Health Promotion Foundation for the grant. Special thanks to Suraphin Chanapit, Maytheewat Tuntichaisrikul, Sarun Kiriya, Waranya Senawiset, and, Thitiphorn Nonkasem for help in facilitating programs at SHPH. And the reviewers for their insightful comments.
Implications
It is unclear what factors influence the success or failure of community health worker (CHW) based programs. We implemented a successful CHW-based smoking cessation program and followed up with a series of focus group discussions to assess which factors were most important to the program’s success. The key factors were: having CHWs that are respected and established in their communities, using CHWs who know their patients and can provide individually tailored solutions, and empowering CHWs with intensive training.
Author Contributions
Conceptualization: Adinat; Methodology: Adinat, Sudarat; Formal analysis and investigation: Adinat, Adam, Sudarat; Writing - original draft preparation: Adinat; Writing - review and editing: Adinat, Adam; Funding acquisition: Adinat; Resources: Adinat, Sudarat, Supervision: Adinat
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Thailand Health Promotion Smoke Free Pharmacy Network in Community Pharmacy Foundation, Thai Health Promotion Foundation. The funding source had no role in the study design, the collection, analysis, and interpretation of the data.
Ethics Approval
All methods were approved by the Institutional Review Board (IRB) at the University of Phayao. Number 2/053/62.
Supplemental Material
Supplemental material for this article is available online.
Consent to Participate
All subjects gave informed written consent to participate in accordance with IRB protocols. Original documents in Thai are available upon reasonable request to the corresponding author.
Consent for Publication
Informed consent documents included specific consent for de-identified quotes to be shared and utilized in publication.
Availability of Data and Material
Original data are available upon reasonable request to the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.