
Abstract
Objectives:
To estimate racial/ethnic differences in the extent to which mental health treatment is obtained from mental health providers, primary care physicians (PCPs), or both and to examine the effects of provider type on change in mental component scores (MCS) of the SF-12 on different race/ethnic groups.
Methods:
Secondary data analysis of 2008 to 2015 Medical Expenditure Panel Survey (MEPS). Non-institutionalized civilian US population, aged 18 to 64 (N = 62 558). Based on counts of all mental health visits in a calendar year, we identified patients who obtained care from PCPs, mental health provider, PCP and mental health providers and other providers and examined changes in MCS by type of care.
Results:
9.9% of Non-Hispanic Whites obtained mental health treatment, compared to 5.0% for Hispanics, 5.3% for Blacks and 5.5% for Other Races (P < .001). Non-Hispanic Blacks and non-Hispanic “Other” were more likely than other groups to obtain care from mental health providers only (P = .017). All obtaining care solely from PCP had better mental health (mean (se)) MCS: 43.2(0.28)) than those obtaining care solely from mental health provider (39.8 (0.48)), which in turn was higher than for those obtaining care from both PC and MH providers (38.5 (0.31), (P < .001).
Conclusion:
Even when diagnosed with a mental health disorder, Hispanics and Blacks were less likely to seek mental health treatment than Whites, highlighting the continuing disparity. Future research should focus on understanding how and what aspects of integrated care models and other mental health delivery models that reduce disparities and provide greater accessibility.
Introduction
Major depressive disorders are a major cause of disability-adjusted life years (DALYs) lost in the U.S. 1 Additionally, depression will be 1 of the 3 leading causes of disability in the developed world by 2030. 2 In 2017, the U.S. spent $183 billion on mental and substance use disorders, a figure likely to rise with continued population growth and aging. 3 However, the greatest costs often cannot be directly measured, and include lost productivity/economic output, decreased quality of life, increased need for social support services, increased housing instability, and increased burden on caregivers. 4 The World Economic Forum study has estimated global cost in lost economic output could reach $16 trillion in the next 20 years. Despite this, treatment rates remain low, with large disparities in treatment access and utilization especially in racial/ethnic minorities. 5
Research suggests that little has changed since the 2001 Surgeon General’s report highlighting cultural and racial disparities in U.S. mental health care.6-9 Recent literature shows that while Blacks and Hispanics have poorer mental health, they are less likely to obtain mental health treatment. Racial and ethnic differences persist in the receipt of mental health services among young adults. Blacks are less likely to have received mental health services than non-Hispanic Whites, and even when minorities seek mental health services, they are more likely to seek services within a general healthcare setting or inpatient setting, and less likely to receive guideline-conforming care.10-13
There are a variety of barriers to receiving mental health treatment, such as cost, stigma about mental health, biases of providers, poor health literacy, poor insight, geographic inaccessibility, and linguistic/cultural barriers.14,15 Behavioral health integration in primary care, the largest healthcare delivery platform in the U.S., is increasingly recognized as essential to effective and cost-efficient care for populations and individuals.16-18 Evidence highlights the utility of integrated models in ameliorating disparities in mental health treatment.19,20
However, while disparities in receipt of mental health treatment among minority groups have been well documented, less is known about which providers minorities seek out or the quality of the care they receive. As health systems and communities increasingly transition toward an integrated model of care, knowing where individuals from at-risk, minority groups are seeking and receiving care will help to better address these mental health care gaps and better structure collaborative programs. In our research, we aim to estimate racial/ethnic differences in the extent to which mental health treatment is obtained from mental health (MH) providers only, primary care physicians (PCPs) only, or a combination of primary care (PC) and MH providers (eg, psychiatrists, psychologists, and/or social workers). We will also examine the effect of type of provider on changes in mental health. Based on previous research, we hypothesize that individuals who are Black and Hispanic will more often receive mental health treatment from primary care doctors rather than from mental health specialists. Further, we hypothesize that non-White individuals will experience poorer outcomes when accessing mental health care.
Methods
MEPS collects detailed information on demographics, medical conditions, diagnostic codes, medications, employment, income, insurance, medical expenditure, and health status. MEPS includes information collected from the Self-Administered Questionnaire (SAQ), which is available in both English and Spanish. The SAQ includes the Short Form Health Survey 12 version (2) (r) (SF-12), which consists of 12 questions regarding mental and physical health. Results are summarized into Physical Component (PCS) and Mental Component Scores (MCS) based on a standard algorithm. 22 Respondents were recruited and interviewed 5 times in a 2-year period in the MEPS. Each year, AHRQ releases data consisting of overlapping data from 2 panels. We examined full-year consolidated files and office-based medical event files. For health status, we used SF-12 MCS scores as baseline mental health measures and change in mental health measurement at the round II and IV interviews, respectively.
Study Sample
We pooled 2008 to 2015 MEPS data (N = 284 296) restricted to respondents who completed the SAQ (176 061) and who had 2 years of data to examine the change in MCS from rounds II to IV (N = 62 558). As we conducted secondary data analysis of publicly available de-identified data, this study was exempted from human participants review by the Institutional Review Board.
Exposure Measures
Data on mental health visits were obtained from office-based visits when respondents indicated that the provider addressed their mental health concern(s) during the visit. We used the AHRQ Clinical Classification Codes to classify reported mental health conditions into the following: depression, anxiety (“neurotic”) disorder, schizophrenic disorder, affective disorder, acute stress, and adjustment reaction. 23 For each office visit, respondents were asked to identify type and specialty of provider seen. For each respondent, we counted total number of mental health visits over our observation period as well as counts to each type of provider, from rounds II through IV. This period is approximately 1 year, with considerable variation (mean = 358.3 days, SD = 54.6). Based on this, we created 4 groups:
(1) Primary Care Only (n = 1770): All office-based care in the past 12 months received from PCP (ie, internal medicine, family medicine, general practice).
(2) Mental Health Only (n = 699): All office-based care in the past 12 months received from MH professionals (ie, psychologists, social workers, psychiatrists).
(3) Both mental health and primary care (n = 1519): Office-based care/treatment obtained from both PC and MH professionals.
(4) Treatment from other providers (n = 385): Care obtained exclusively from other providers (eg, specialists, chiropractors, technicians, nurse practitioners/nurses, physician assistants).
Outcome Measures
MEPS uses the SF-12 from the SAQ to assess functional health and wellbeing, which results in the MCS, a composite mental health score that is standardized, with a mean of 50 and standard deviation of 10. Lower scores correspond to poorer mental health status. Research demonstrates that individuals with moderate mental health illnesses scored between 30 and 39, and those with severe mental health issues had scores below 30.24,25 We calculated the difference in MCS (N = 62 558) from rounds II to IV to determine change in mental health.
Covariates
Our selection of covariates was based on the Anderson Behavioral Model of health service use, which has been used extensively in analyses relating to health service use and access.26,27 We used marital status and employment from the second interview and gender, age, education, insurance status, and income measured in the first year as covariates in our multivariate analyses. We recoded age into 3 groups (18-29, 30-44, 45-64). Education was recoded into 3 categories—(1) less than high school degree, (2) high school degree, and (3) higher than high school. Respondents were classified into 4 racial/ethnic groups—(1) Non-Hispanic Whites, (2) Non-Hispanic Blacks, (3) Non-Hispanic Other, and (4) Hispanic. The 4 census regions were: (1) South, (2) Northeast, (3) Midwest, and (4) West. We categorized employment status into 2 categories—(1) Employed and (2) Non-employed. We treated respondents’ missing data on employment as a third group (n = 165) to ensure no significant differences among those who had valid employment data and those who were missing employment data.
Analysis
We analyzed data using Stata 14.2 statistical software. 28 We calculated descriptive statistics and reported number and percentages for categorical variables and means and standard errors for continuous variables. We used a Chi-squared test for categorical variables to identify statistically significant differences in demographics, and ANOVA for MCS across the 4 races/ethnicities. We used multiple linear regression models to measure associations between provider type and change in MCS (Supplemental Table 1). Sampling weights with survey design variables were used to account for oversampling, stratification, and complex MEPS survey design to obtain a nationally representative sample. 22
Results
We restricted our analysis to respondents aged 18 to 64 years with valid data on the MCS and covariates, which yielded a final sample of 62 558 (Table 1). Consistent with previous studies, we found substantial differences across race and ethnicity in regards to demographic characteristics. The proportion of women was higher among Blacks than the other racial/ethnic groups (55%, P < .001). A lower percentage of Hispanics were older than 45 when compared to other race/ethnicity groups, with 30.9% of Hispanics age 45 to 64, as compared to 47.1% of Whites, and 39.7% of Blacks (P < .001). Non-Hispanic Whites were more likely to be married, employed, privately insured, and higher income than other racial/ethnic groups (P < .001). The percentage of those having some college or college degree was higher among Non-Hispanic “Other” compared to all other racial/ethnic groups (69.8%, <.001).
Distribution of Demographic Characteristics by Race/Ethnicity (N = 62 558).

Source: 2008-2015 medical expenditure panel survey (N = 62 558). df = 3.
Chi-squared test of significance across race/ethnicity categories.
Of the adults in the 2008 to 2015 pooled data, 4372 had a mental health diagnosis (Table 2). This includes 9.9% of Non-Hispanic Whites, compared to 5.0% for Hispanics, 5.3% for Blacks and 5.5% for Other Races (P < .001). Non-Hispanic Blacks and Non-Hispanic Others were more likely than other groups to receive care from Mental Health providers only and less likely to receive care from a PCP alone (Table 2).
Distribution of Respondents with Mental Health Diagnosis/Treatment by Race and Provider Type.
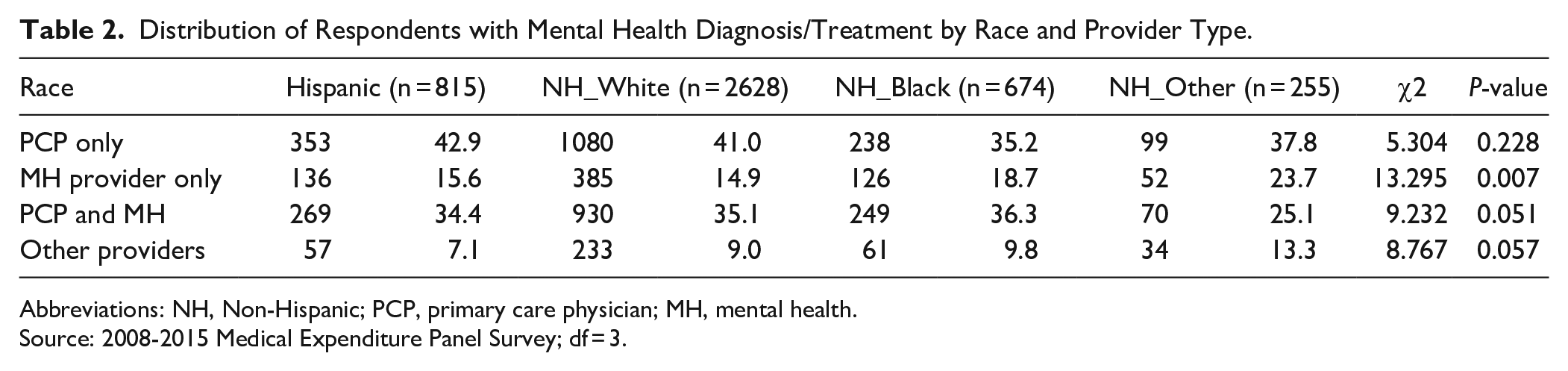
Abbreviations: NH, Non-Hispanic; PCP, primary care physician; MH, mental health.
Source: 2008-2015 Medical Expenditure Panel Survey; df = 3.
There were relatively small differences by race in baseline (round II) MCS scores among all non-elderly adults (with and without a mental health diagnosis), with scores ranging from 50.5 for Non-Hispanic whites to 51.7 for the “Other” category (Table 3). Between the second and fourth interviews, these scores improved by about 0.4 points, with minor variation across groups. Across the different care options, we found a gradient in baseline MCS scores across provider types (Table 3)—which in turn was higher than for those obtaining care from both PC and MH providers (38.5 (0.31), (P < .001). Individuals obtaining care from all MH providers had the lowest baseline MCS scores (34.6 (1.12)). By contrast, there were substantial differences across provider types in the number of MH visits, with fewer for patients obtaining care solely from PCPs.
Baseline MCS Scores, Change in MCS Scores and Number of MH Visits, for Full Sample and by Type of Care.
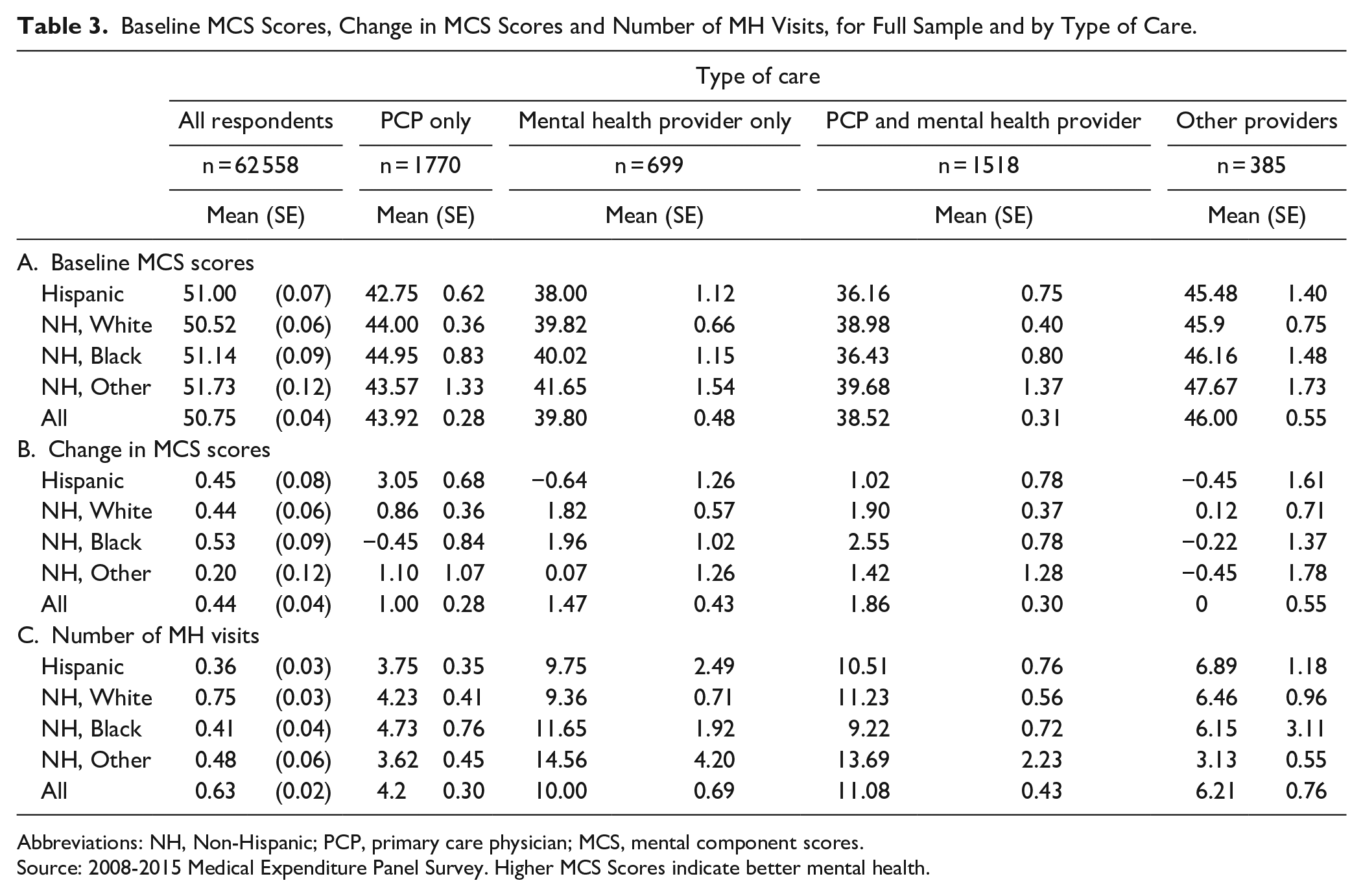
Abbreviations: NH, Non-Hispanic; PCP, primary care physician; MCS, mental component scores.
Source: 2008-2015 Medical Expenditure Panel Survey. Higher MCS Scores indicate better mental health.
The multivariate results in Table 4 show that overall change in MCS scores for those with mental health diagnoses improved least for persons obtaining care from MH providers only (β = −1.17, 95% CI: −2.17 to −0.18) or from both PCPs and MH providers (β = −1.37, 95% CI: −2.22 to −0.51) when compared to those obtaining care only from PCPs (who, as noted above, had healthier baselines). These results are statistically significant yet modest in magnitude (for perspective, a 2-point decline in MCS scores is about 0.2 standard deviations).
Linear Regression Showing Change in MCS by all Provider Types and Race/Ethnicity Among Adults with a Mental Health Diagnosis.

Abbreviations: NH, Non-Hispanic; CI, confidence interval; PCP, primary care physician.
Source: 2008-2015 Medical Expenditure Panel Survey. Regression models adjusted for age, gender, education, census region, income, marital status, MCS and insurance coverage.
P < .001, **P < .05, *P < .10.
These patterns varied by race/ethnicity, especially for Hispanics. In the second panel, Hispanics who obtained care from PCPs had substantially better improvement in MCS scores compared to all other care combinations, except for “other providers.” MCS change scores for Hispanics who obtained care only from MH providers were about 5.5 points smaller (ie, less improvement) than those who obtained care only from PCPs ((β = −5.49, 95% CI: −8.72 to −2.27).
Discussion
Although much research has focused on disparities in receipt of mental health treatment among minority groups, less is known about which type of providers they seek out or how provider type affects outcomes. This study aimed to quantify from which type of providers minorities currently receive mental health care. Consistent with prior literature, non-Hispanic Whites were more likely to obtain mental health treatment than minorities.29,30 However, our findings that Blacks were more likely to receive care from MH providers is inconsistent with previous findings.12,13 This interesting and unexpected finding may reflect differences in baseline access to care—ie, that Black respondents were less likely to have a primary doctor at baseline and thus did not seek mental health services from a PCP. More research, including qualitative studies, would help elucidate the reason for this observation. The large majority of individuals obtaining mental health treatment received care either solely from PCPs or from MH and PC providers jointly, underscoring the importance of primary care in access to mental health treatment.
Whites and Hispanics were more likely to obtain care solely from PCPs, while Blacks were more likely to receive treatment from MH providers. Outcomes varied depending on provider. Individuals receiving treatment by PCP only experienced the greatest magnitude of improvement compared to those receiving treatment by a MH provider. It is important to note that individuals receiving treatment from a MH provider or MH and PCP began treatment with lower baseline MCS scores, indicating poorer mental health status. Individuals experiencing higher levels of mental distress may obtain care from specialized mental health professionals, while individuals experiencing milder forms of distress more often obtain care from PCPs. Outcomes also varied by race/ethnicity, particularly for Hispanics. These outcomes mirror previous outcomes and suggest that Hispanics who received mental health treatment from PCPs experienced greater improvement in MCS scores. Again, those with a mental health condition who seek care from PCPs may have less severe/persistent mental health disorders at baseline, and therefore have greater changes in MCS scores. It is reasonable to expect those patients who seek care from a psychiatrist to have a greater change in MCS but in this study, they do not. This may be because they severe/persistent mental illness to begin with, resulting in smaller change in MCS pre- and post-treatment. Note that absolute changes in MCS score are shown in Table 3, but score changes in Table 4 are represented relative to a reference group (receipt of care by PCP only), and do not represent MCS changes in a negative direction.
Integrated care including both primary care and mental health services has proven to be an effective delivery modality for patients with both chronic disease and mental health issues. 22 Integrated care was proposed as a solution in the President’s New Freedom Commission on Mental Health in 2003 and in many subsequent studies.16,19,31 There are many potential barriers to racial/ethnic minorities accessing specialized or integrated mental health services. 32 Understanding these barriers is the next step to achieving effective mental health treatment. Geographic as well as financial accessibility may be 2 such barriers. Other barriers may include cultural/linguistic barriers. Attitudes toward mental health treatment (eg, perceived treatment efficacy, willingness to seek help, or comfort talking to professionals) vary among racial/ethnic groups and becoming aware of and addressing these attitudes will affect treatment receipt differentially.33,34
This current study has some limitations. The use of secondary data and retrospective study design is limit its ability to infer causality, and create potential sampling bias present in the original survey. Many household surveys result in a failure to include some segments of the U.S. population in research studies. 6 The prevalence of a mental health disorder in this study’s sample was 6%, while current U.S. prevalence estimates are approximately 18% among adults. 35 This discrepancy may suggest that this sample is not representative of the broader U.S. population, limiting generalizability of its findings. However, given restrictions of this study’s analysis to office visits where a mental health diagnosis was made, it is likely that the actual prevalence within the sample is higher.
This study compared patients in 4 broadly defined racial/ethnic groups, each composed of a heterogeneous mix of individuals. Thus, this study cannot differentiate the needs of more specific subgroups. In addition, there were differences in baseline demographics. For example, more Blacks were female, more Hispanics were under age 45, and more Blacks reported better general health. Although many covariates were controlled for, there may be other cofounding variables that were overlooked, such as managed care plans that may be variable in their restrictions on access to specialty services.
Lastly, this study compared outcomes for 4 types of providers/groupings but did not include an explicitly defined “integrated care” model. The cohort who received mental health care from both MH and PC providers were not necessarily presenting to integrated care settings. Given the potential of integrated care to address the needs of underserved populations, it would be useful to include an integrated care setting, as this would contribute to the growing literature on the effectiveness of the integrated care model for minorities’ mental health treatment. Additionally, care provided in non-traditional settings are also prudent to addressing gaps in mental healthcare access by race and ethnicity. These include outreach-based care, such as Assertive Community Treatment and intensive case management. These also include community interventions, such as mental health partnerships with churches and other trusted community venues, multi-sector partnerships, and care provided by trusted community members such as community health workers and/or peer support programs. 36
Conclusion
In our population-based study of mental health care receipt, non-Hispanic Whites were almost twice as likely as Hispanics and non-Hispanic Blacks to receive care for a mental health diagnosis. Among those with mental health diagnoses, Blacks were more likely to receive care from mental health specialists rather than PCPs. Across race/ethnic distinctions, mental health scores improved most when care was given by PCPs, although this group of patients also had higher mental health scores at baseline. Future research is needed to clarify how these dimensions of access and receipt of care affect outcomes for individuals from minority populations.
Supplemental Material
Supplemental_Table_1 – Supplemental material for Taking a Closer Look at Mental Health Treatment Differences: Effectiveness of Mental Health Treatment by Provider Type in Racial and Ethnic Minorities
Supplemental material, Supplemental_Table_1 for Taking a Closer Look at Mental Health Treatment Differences: Effectiveness of Mental Health Treatment by Provider Type in Racial and Ethnic Minorities by Tracey L. Henry, Anuradha Jetty, Stephen Petterson, Helaina Jaffree, Allie Ramsay, Erica Heiman and Andrew Bazemore in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.