
Abstract
Keywords
Introduction
Diabetes mellitus is increasing in prevalence both in urban and rural population in India.1 -3 The main consequences, in the long term, of uncontrolled diabetes are microvascular (nephropathy, retinopathy, and neuropathy) and macrovascular (coronary artery disease, cerebrovascular, and peripheral vascular disease) complications. 4 The latter has resulted in diabetes being proclaimed as vascular disease and it is the leading cause of cardiovascular death worldwide. 5 The clinical management of the patient with diabetes includes not only addressing hyperglycemia but also screening for the angiopathic complications and assessing the other risk factors. 6
The burden of diabetic complications is high in India because of the large number of people with diabetes. 7 Studies from India reported a prevalence of 5% to 37% of macrovascular and microvascular complications among diabetes patients.8,9 Patients with diabetes and associated microvascular complications are at higher risk of accelerated atherosclerosis which ultimately culminates in cerebrovascular and cardiovascular events and premature death. 6 A multicentric study in India reported a high prevalence of microvascular complications like diabetic neuropathy (26.1%) and nephropathy (26.9%). 10 The prevalence of undetected complications is more in rural area when compared to urban area, due to poor control of diabetes, lack of awareness, and limited access to health care.1,11
Population data on diabetes complications are available in urban India. 11 Data on the burden of vascular complications of diabetes, its prevalence and severity are scarce from the rural setting in India.12,13 This may be due to lack of expertise in rural clinics, non-availability of tools that may be required for screening as well as cost of the tests. 14 India being a developing country and with majority of the population being in rural area, comprehensive assessment of diabetic patients and identifying the complications becomes the need of the hour. Screening for both macro and microvascular complications in type 2 diabetes patients will help in understanding the burden of the problem. In this background, we proposed to assess the prevalence of vascular complications in type 2 diabetes patients with clinical examination and simple easily available tools in a rural health center.
Methodology
Study Setting and Population
This hospital based cross sectional study was conducted in Rural Health and Training Centre (RHTC) of Department of Community Medicine of medical college located at Vayallanullur, Tamil Nadu from Jan 2017 to Aug 2017. Based on study done by Agarwal et al, on vascular complication of diabetes (prevalence of neuropathy—32.5%), the minimum sample size was calculated to be 324 subjects at 95% confidence level and 5% of allowable error. 8 RHTC caters to 800 diabetic and hypertensive patients who are registered with the center. Of them, 300 were diagnosed with only hypertension and another 100 were not regular in their visits for treatment and so they were excluded from this study.
Data Collection and Quality Control Measures
Information on background demographic characteristics like age, gender, education, occupation, etc. was collected using a pretested structured questionnaire. Details of co-morbidities were obtained from their records as well as from history. The content validity of the questionnaire was examined by an expert team of 3 endocrinologists. The questionnaire was then translated to Tamil and then back translated to English by language experts. Data collection was done by the principal and co-investigators of the study.
Anthropometric assessment of study population was done using standard procedures. 15 The cut off for waist circumference was taken to be 90 cm for male and 85 cm for female. 16 Blood pressure was measured and patients with blood pressure of either systolic >140 or diastolic > 90 mm Hg were considered to be hypertensive. 17
Complete foot examination was done to look for signs of skin discoloration, absent hair, dystrophic nails, fissured skin, ulceration, gangrene, absence of toes, past healed/unhealed ulcers, deformity, absent peripheral pulses (dorsalis pedis, posterior tibial). Touch (prick) sensation in lower limbs was assessed using 10 g monofilament. The monofilament was held perpendicular to the skin and pressure was applied until the filament just bends with a contact time of 2 seconds. Vibration and touch were tested at 5 areas—plantar surface of distal hallux, heads of first metatarsal, fifth metatarsal, heel, dorsal surface of the foot. In addition, presence or absence of ankle reflex was checked using percussion hammer.
Blood was examined for plasma glucose (fasting and postprandial), HbA1c, and serum creatinine. Urine was examined for glucose, albumin, pus cells, and RBCs. A 12-lead electrocardiogram resting ECG was taken. Nephropathy was assessed using estimated glomerular filtration rate (eGFR) which was calculated by the abbreviated MDRD equation (Modification of Diet in Renal Disease). 18 Based on the patient’s history, physical examination and laboratory findings, vascular complications of diabetes were diagnosed by an endocrinologist (SM).
Operational Definition of Vascular Complications Macrovascular Complications
Coronary artery disease (CAD): History of angina or myocardial infarction or/and documented in medical records or abnormal ECG findings indicating the presence of ischemia or infarction indicating coronary artery disease. 19
Cerebrovascular disease (CVD): History of stroke or transient ischemic attack/hemiplegia or/and documented in medical records. 20
Peripheral vascular disease (PVD): Definitive history of intermittent claudication or if one or more peripheral pulses absent in any one foot. 21
Microvascular Complications
Peripheral neuropathy: Ankle reflex absent or 10 g monofilament for touch is
<3/5 or 128 Hz vibration sense is <3/5 in any 1 foot. 22
Nephropathy: Estimated Glomerular filtration rate less than 60 mL/min/1.73 m2. 23
Diabetic foot: Presence of ulcer/old healed ulcer/ gangrene/ deformity/amputation in either foot. 24
Ethics
Ethical approval was obtained from Institutional Ethics Committee prior to the commencement of the study (IEC-NI/16/NOV/56/81). Written informed consent was obtained from all participants before data collection after giving the details of the study.
Data Processing and Analysis
Data entry and analysis of the variables was done using Statistical Package for Social Sciences (SPSS) version 16 (IBM Corporation, Somers, New York, USA) software after checking for completeness. Qualitative variables such as socio-demographic characteristics were expressed as frequency and percentages. The prevalence of vascular complications of diabetes was calculated as percentages and 95% Confidence Interval. Univariate and multiple logistic regression analysis was done to identify various factors associated with complications of diabetes among study subjects. “Two sided” P value of <.05 was considered to be statistically significant.
Missingness was observed in certain background variables such as education (0.2%), waist circumference (3.5%), and duration of diabetes (2.8%). About 1.5% of blood parameters like FBS and PPBS were missing due to errors in processing of blood sample.
Results
Out of the 400 diabetic patients who attended the diabetic clinic at the rural health center, 10 patients refused to give consent. The remaining 390 patients were included in the study. The socio-demographic characteristics of the study subjects are given in Table 1. The mean (SD) age of study population was 56.3 ± 10.1 years. About three fourth of the study population were females. About 65% of study population were educated less than primary school level. The mean (SD) BMI was 26.9 ± 11.4 kg/m2 and more than 50% of the study population were overweight/obese. The mean (SD) duration of diabetes was 6.3 ± 6.1 years. Based on the HbA1c value about 55.4% of study population had their diabetes under control (HbA1c < 7%).
Socio Demographic Characteristics of Study Subjects (n = 390).
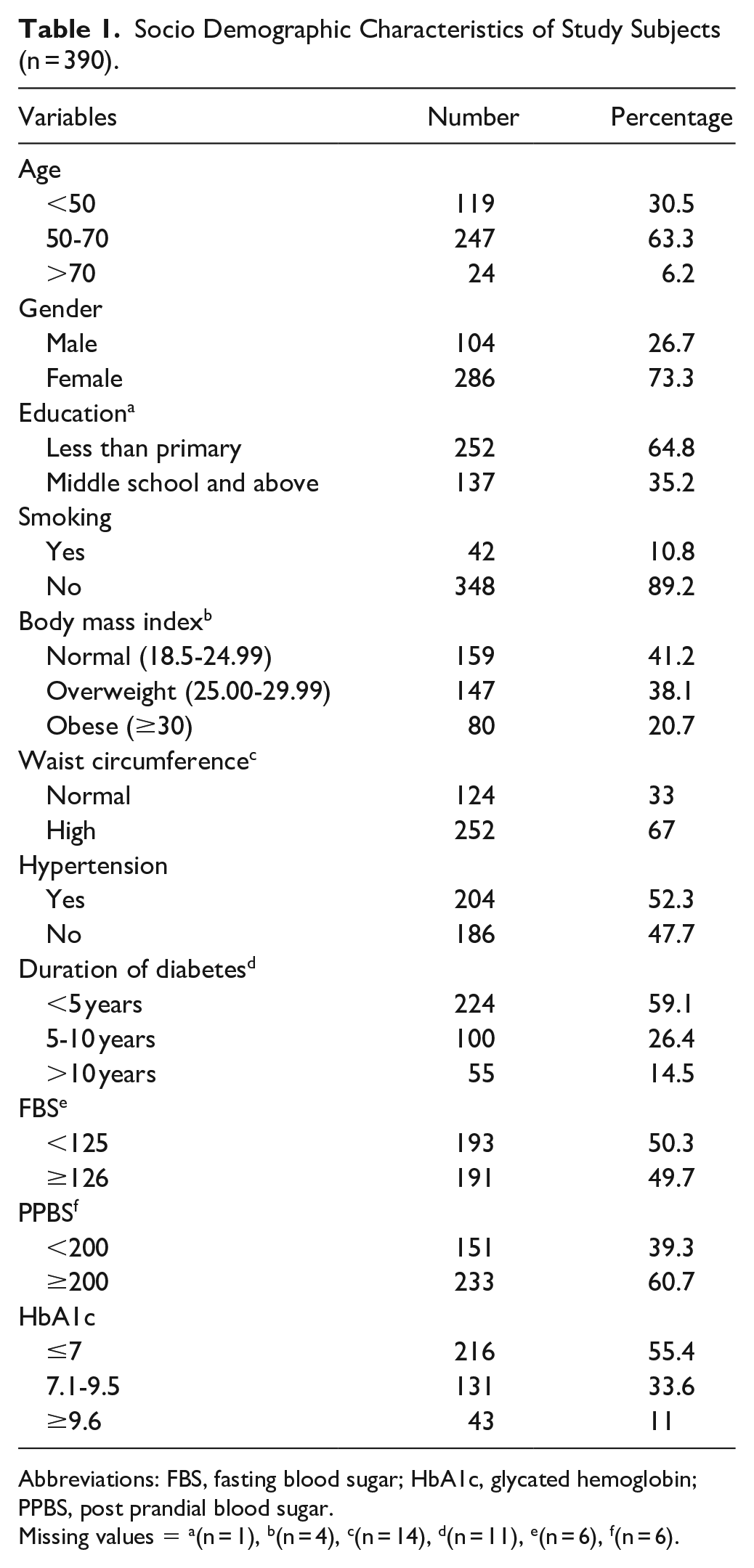
Abbreviations: FBS, fasting blood sugar; HbA1c, glycated hemoglobin; PPBS, post prandial blood sugar.
Missing values = a(n = 1), b(n = 4), c(n = 14), d(n = 11), e(n = 6), f(n = 6).
The overall prevalence of macrovascular and microvascular complications in our study population was 29.7% and 52.1%, respectively. About 19.7% of study subjects had both macro and microvascular complications (Figure 1). Figures 2 and 3 describes the various signs and symptoms of complications of diabetes. About 12.3% of study subjects presented with abnormal ECG findings. History of CAD and CVD was observed in 4.4% and 1.5% of study subjects respectively. About 3.3% and 12.3% of study subjects presented with history of intermittent claudication and absent peripheral pulses. Among the symptoms of peripheral neuropathy, diminished touch sensation (30.3%) was most prevalent followed by absent ankle reflex (23.1) and diminished vibration (17.3). About 10% of study subjects had abnormal urine albumin and serum creatinine. The findings of diabetic foot among the study participants were presence of ulcer (3.6%), healed ulcer (4.3%), gangrene (0.8%), and deformity (6.2%).

Prevalence of both macro and microvascular complications among type 2 diabetes patients in a Rural Health Centre (n = 390).

Prevalence of signs and symptoms of macrovascular complications among study subjects (n = 390).

Prevalence of signs and symptoms of microvascular complications among study subjects (n = 390).
Table 2 describes the prevalence of macrovascular complications and univariate analysis of various background variables with macrovascular complications. The prevalence of coronary artery disease (CAD), peripheral vascular disease (PVD) and cerebrovascular Disease (CVD) in our study population were 15.1%, 15.1%, and 1.5% respectively. Univariate analysis showed that increasing age, lower education, hypertension was significantly associated with increased risk of coronary artery disease. Hypertension and increased duration of diabetes were associated with increased risk of cerebrovascular disease.
Prevalence and Association of Various Background Characteristics with the Macrovascular Complications Among Study Subjects.

Abbreviations: FBS, fasting blood sugar; HbA1c, glycated hemoglobin; PPBS, post prandial blood sugar.
Indicates unadjusted odds ratio (95% CI) of age 50-70 years versus <50 years for macrovascular complications, CAD, PVD respectively and a1,c1,e1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of age >70 years versus <50 years for macrovascular complications, CAD, PVD respectively and b1,d1,f1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of duration of diabetes 5-10 years versus <5 years for macrovascular complications, CAD, PVD respectively and g1,i1,k1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of duration of diabetes >10 years versus <5 years for macrovascular complications, CAD, PVD respectively and h1,j1,l1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of HbA1c (7.1%-9.5%) versus HbA1c (
Indicates unadjusted odds ratio (95% CI) of HbA1c (>9.6) versus HbA1c (
P < .05.
Unadjusted odds ratio.
Table 3 describes the prevalence of microvascular complications and its association with various background variables. Peripheral neuropathy (44.9%) had the highest prevalence followed by nephropathy (12.1%) and diabetic foot (7.2%). Univariate analysis showed that factors such as increasing age, lower education, increased duration of diabetes, higher fasting blood sugar, postprandial blood sugar and HbA1c (≥9.6%) were significantly associated with peripheral neuropathy(P < .05). Hypertension was significantly associated with nephropathy (P < .05) whereas higher glycemic parameters such as fasting, postprandial blood sugars, and HbA1c were significantly associated with diabetic foot (P < .05).
Prevalence and Association of Various Background Characteristics With the Microvascular Complications Among Study Subjects.

Abbreviations: FBS, fasting blood sugar; HbA1c, glycated hemoglobin; PPBS, post prandial blood sugar.
Indicates unadjusted odds ratio (95% CI) of age 50 to 70 years versus <50 years for microvascular complications, neuropathy, nephropathy respectively and a1,c1,e1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of age >70 years versus <50 years for microvascular complications, neuropathy, nephropathy respectively and b1,d1,f1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of duration of diabetes 5 to 10 years versus <5 years for microvascular complications, neuropathy, nephropathy, diabetic foot respectively and g1, i1,k1,m1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of duration of diabetes >10 years versus <5 years for microvascular complications, neuropathy, nephropathy, diabetic foot respectively and h1,j1,l1,n1indicates the corresponding P values.
Indicates unadjusted odds ratio (95% CI) of HbA1c (7.1%-9.5%) versus HbA1c (
Indicates unadjusted odds ratio (95% CI) of HbA1c (>9.6) versus HbA1c (
P < .05.
Unadjusted odds ratio.
Multiple logistic regression analysis was done on 376 subjects due to missingness observed. Regression analysis for macrovascular complications (Table 4) showed that subjects with primary schooling and less (Adjusted odds ratio (aOR) = 2.1[1.1-4.5]), being hypertensive (aOR = 2.0[1.1-3.8]) had increased risk of associated CAD than those with higher education and normotensives. Study subjects with abdominal obesity had 2.2 [1.1-4.5] times increased risk of associated PVD than those with normal waist measurements (P = .031).
Logistic Regression Analysis of Various Background Characteristics With the Macrovascular Complications Among Study Subjects (n = 376).

Abbreviations: FBS, fasting blood sugar; PPBS, post prandial blood sugar.
Adjusted for age, gender, education, smoking, waist circumference, hypertension, duration of diabetes, FBS, PPBS, HbA1c.
P < .05.
Multiple logistic regression analysis (Table 5) for microvascular complications showed the less than primary schooling (aOR = 2.8[1.7-4.8]), duration of diabetes > 5 years (aOR = 1.8[1.1-3.2]), postprandial blood sugar (≥200 mg/dl) (aOR = 1.7[1.1-2.9]) and HbA1c (≥9.6%) (aOR = 2.6[1.2-5.9]) had increased risk of associated neuropathy than the others. Females (aOR = 0.3[0.1-0.9]) had lower risk of associated diabetic foot than males. Subjects with HbA1c (7.1%-9.5%) value had 4.1 [1.4-11.3] times increased risk of associated diabetic foot than those with HbA1c of (≤7%).
Logistic Regression Analysis of Various Background Characteristics with the Microvascular Complications among Study Subjects (n = 376).
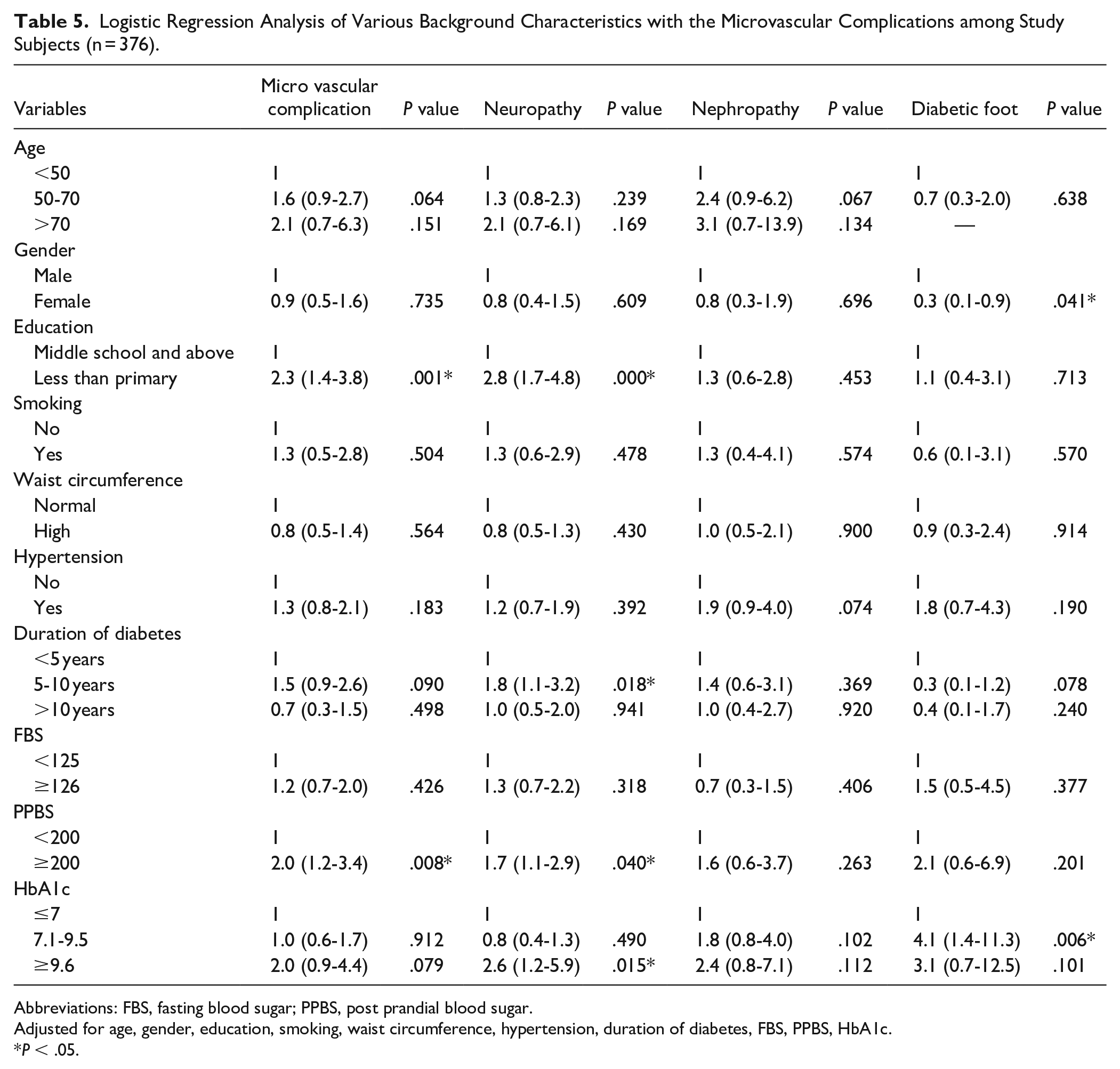
Abbreviations: FBS, fasting blood sugar; PPBS, post prandial blood sugar.
Adjusted for age, gender, education, smoking, waist circumference, hypertension, duration of diabetes, FBS, PPBS, HbA1c.
P < .05.
Discussion
In this study, simple, easily available screening tools were used to assess the prevalence of vascular complications of diabetes in a rural setting. It revealed high prevalence of both micro and macrovascular complications in the population. The implications of the study findings are: (1) burden of vascular complications is quite high in our rural population also, (2) simple tools of assessment may suffice in periodic evaluation of these patients.
Among the macrovascular complications, the prevalence of CAD and PVD was high (15.1%) followed by CVD (1.5%). Studies done in rural India observed the prevalence of Ischemic heart disease and stroke to be 7.8% to 11.4% and 0.5% respectively.13,25 Study done by Agarwal et al observed that the prevalence of PVD by both clinical examination and doppler to be 18.1% which was close to our study findings. 26 Presence of claudication (likelihood ratio LR—3.30) and any pulse abnormality (LR, 3.10) are the most useful clinical findings in diagnosis of PVD. PVD is one of the dangerous complications of diabetes, a simple history of intermittent claudication and examination of peripheral pulses will help in early detection of PVD and patients can be referred to higher centers for further diagnosis and treatment. 27
Among the microvascular complication, peripheral neuropathy (44.9%) had the highest prevalence followed by nephropathy (12.1%) and diabetic foot (7.2%). Studies have shown the prevalence of peripheral neuropathy in South India to range from 10.5% to 60.4%.28 -30 The prevalence was higher in urban areas when compared to rural area.31 -33 The high prevalence in rural areas could be due to delay in diagnosis, poor self-care, poor health-seeking behavior. In the current study, medical officers in the rural center were trained to use these simple tools like monofilament and VibraTip for early detection of peripheral neuropathy which can be implemented country wide. Awareness program on foot care was conducted with special training to patients diagnosed with peripheral neuropathy.
A multicentric study done in India to screen diabetic patients for presence of diabetic foot revealed 8.7% of study population suffered from foot ulcers and blisters which was close to our study findings (7.2%). 34 In our study comprehensive assessment of foot along with peripheral vascular disease and peripheral neuropathy was done which helped in identifying at -risk foot too. Medical officers in rural center were trained to educate the patients on simple self-foot examination which is a very effective preventive strategy to reduce this grave complication.
Diabetic nephropathy is the leading cause of end-stage renal disease world-wide. 35 A study done in rural India reported that the prevalence of diabetic nephropathy was 13.6% close to our study findings (12.1%). 36 Nephropathy was assessed by eGFR (MDRD equation) which requires age, gender, serum creatinine value of patients. Using this simple method yearly once screening of patients for nephropathy is highly recommended to diagnose early and prevent further progression of the disease.
Lower education status, hypertension were independent and commonly encountered risk factors for CAD. Educational status influences the awareness about diabetes, compliance to drugs and the health seeking behavior of an individual. Studies have observed that lower the education higher is the risk of CAD.37,38 The risk of PVD in diabetic patients increased 2.2 times in those with high waist circumference which is a measure of abdominal obesity. Study done by Rao et al observed that abdominal obesity measured by waist-hip ratio and waist circumference were independent and significant risk factor of PVD similar to our study findings. 39
Lower education, increased duration of diabetes, high postprandial blood sugar and high HbA1c values were significantly associated with peripheral neuropathy (P < .05). A meta-analysis on diabetic neuropathy observed that duration of diabetes, HbA1c are significantly associated with increased risks of DPN among diabetic patients. 40 Studies done in India observed that poor glycemic control and increased duration of diabetes were significantly associated with diabetic neuropathy which was similar to our study findings.41,42 Males have higher risk of developing diabetic foot than females. Agriculture is the major occupation in rural India and men are more prone to foot injuries during work than women and this could be reason for this difference. Study done by Dinh et al also observed similar results. 43 Poor glycemic control was also associated with occurrence of diabetic foot. Study done by Arambewela et al observed that risk of diabetic foot increased with increase in HbA1c value similar to our study results. 44 Good glycemic control and proper self-care of foot has proven to dramatically decrease the prevalence of diabetic foot. 45
Limitations of Study
Few limitations of the study were because of cross sectional nature of the study, temporality of association between factors studied and risk of complications among diabetes patients could not be established. As the study was conducted in a rural health center, dilation and examination of eyes for diabetic retinopathy was not feasible and lipid profile was not taken due to lack of facilities. Majority of our study population were women as it was center based study done during daytime.
Strength of Study
Simple, easily available tools for assessment of diabetes complications were used in this study making it highly relevant for resource constrained settings in both urban and rural settings in our country.
Conclusion
High prevalence of vascular complications was observed in this study from rural center. Simple, effective, and easily available tools may suffice to screen for the complications facilitating early diagnosis and referral. Factors such as education, hypertension, HbA1c, and postprandial blood sugar were strongly associated with increase in vascular complications of diabetes.
Footnotes
Authors’ Note
Place where research was conducted: Rural Health and Training Centre, Vayalanallur, Department of Community Medicine, Sri Ramachandra Medical College and Research Institute, Sri Ramachandra Institute of Higher Education and Research
Author Contributions
AGV: concepts; design; definition of intellectual content; literature search; data acquisition; data analysis; statistical analysis; manuscript preparation; manuscript editing; manuscript review; guarantor. AJ: definition of intellectual content; literature search; data acquisition; data analysis; manuscript preparation; manuscript editing; manuscript review; guarantor. SV: definition of intellectual content; literature search; data acquisition; data analysis; manuscript preparation; manuscript editing; manuscript review; guarantor. VS: concepts; design; definition of intellectual content; literature search; data acquisition; data analysis; statistical analysis; manuscript preparation; manuscript editing; manuscript review; guarantor. ARM: data acquisition; manuscript editing; guarantor. VD: concepts; design; data acquisition; guarantor. GT: data analysis; statistical analysis; guarantor. SM: concepts; design; definition of intellectual content; manuscript preparation; manuscript editing; manuscript review; guarantor. The manuscript has been read and approved by all the authors, the requirements for authorship have been met and each author believes that the manuscript represents honest work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.