
Abstract
Introduction:
Minority communities have had limited access to advances in genomic medicine. Mayo Clinic and Mountain Park Health Center, a Federally Qualified Health Center in Phoenix, Arizona, partnered to assess the feasibility of offering genomic screening to Latino patients receiving care at a community-based health center. We examined primary care provider (PCP) experiences reporting genomic screening results and integrating those results into patient care.
Methods:
We conducted open-ended, semi-structured interviews with PCPs and other members of the health care team charged with supporting patients who received positive genomic screening results. Interviews were recorded, transcribed, and analyzed thematically.
Results:
Of the 500 patients who pursued genomic screening, 10 received results indicating a genetic variant that warranted clinical management. PCPs felt genomic screening was valuable to patients and their families, and that genomic research should strive to include underrepresented minorities. Providers identified multiple challenges integrating genomic sequencing into patient care, including difficulties maintaining patient contact over time; arranging follow-up medical care; and managing results in an environment with limited genetics expertise. Providers also reflected on the ethics of offering genomic sequencing to patients who may not be able to pursue diagnostic testing or follow-up care due to financial constraints.
Conclusions:
Our results highlight the potential benefits and challenges of bringing advances in precision medicine to community-based health centers serving under-resourced populations. By proactively considering patient support needs, and identifying financial assistance programs and patient-referral mechanisms to support patients who may need specialized medical care, PCPs and other health care providers can help to ensure that precision medicine lives up to its full potential as a tool for improving patient care.
Keywords
Introduction
There has been significant interest in precision medicine as a tool to understand disease and optimize patient care at an individual level. 1 To date, however, the majority of precision medicine initiatives have been positioned in academic medical centers and large healthcare systems.2,3 As a result, the potential health benefits of integrating new forms of precision medicine into community-based health centers that provide primary care services to more diverse communities are unclear.4,5
Integrating genomic medicine into community-based health centers presents several challenges. Many primary care providers (PCPs) report a lack of familiarity with genetic testing and genomic screening.6-8 Absent genetic counseling resources, PCPs working in community-based health centers may find it difficult to educate patients about genetic testing options, establish clinical management plans informed by genetic test results, or obtain insurance coverage for their patients.9,10 Additionally, patients from lower-resource communities, and the physicians who care for them, are concerned about the affordability of genomic medicine and its potential to widen existing health disparities.11-13
To better understand the potential value and challenges of integrating genomic medicine into community-based health centers, we established a partnership between Mayo Clinic and Mountain Park Health Center (MPHC), a Federally Qualified Health Center in Phoenix, Arizona that provides primary care and behavioral health services to financially disadvantaged patients. We offered genomic screening to interested patients, incorporated those results into patients’ electronic health record (EHR), and assessed the impact of genomic screening on patients and healthcare providers.14,15
We describe this partnership in greater detail, focusing on the experiences of PCPs and clinical staff who supported this genomic screening initiative and counseled patients who received positive genomic screening results. Examining both the potential benefits and burdens of integrating genomic screening into community-based health centers that provide care to lower-income patients can help to ensure that precision medicine lives up to its full potential as a tool for improving patient care.
Methods
We invited 1621 patients at MPHC to undergo genomic screening. These patients self-identified as Latino and all had previously provided a blood sample to the Sangre Por Salud Biobank. 15 Of those invited, 500 patients agreed to participate after attending an in-person genetics education session and informed consent discussion, which was conducted in either Spanish or English depending on participant preference. Participants agreed to have their biobank sample analyzed, receive genomic screening results, and have those results placed in their EHR. 16
Genomic analysis included the sequencing of 68 genes known to be associated with disease and screening for 14 actionable single nucleotide variants. 14 After genomic analysis was completed, we contacted participants whose results revealed a pathogenic or likely pathogenic (P/LP) genetic variant by certified mail or telephone and asked them to schedule an in-person appointment. At this appointment, a medical geneticist who was a member of the research team disclosed the patient’s genomic screening results and discussed their potential health implications. An interpreter participated in these discussions when needed. Following this appointment, genomic screening results were placed in the patient’s EHR and an alert was sent to the patient’s PCP. Participants whose results indicated no P/LP variants were notified about their results by mail, with subsequent confirmation of receipt by a study staff member and optional in-person support available by request.
PCPs were encouraged to discuss their patient’s genomic screening results with the medical geneticist who had met with these patients. All PCPs who received an alert about a patient with a positive screening result elected to consult with the medical geneticist in-person. During these one-on-one consultations, PCPs received individualized genomic education focused on the specific results reported to their patient(s). These consultations provided PCPs with an opportunity to discuss the mechanism of disease pathology, the penetrance of the genetic mutation, the need for medical surveillance, and potential clinical management options. The medical geneticist also informed each of the PCPs about diagnostic criteria and clinical practice guidelines relevant to their patients’ results.
To assess provider experiences caring for patients with P/LP results, we conducted semi-structured interviews. These interviews were conducted in-person or by telephone, depending on provider availability, approximately 3 months after their consultation with the medical geneticist and subsequent interactions with their patients. To provide a comprehensive assessment of these experiences, we interviewed PCPs, the medical geneticist, and the primary clinical research coordinator at MPHC who coordinated the reporting of genomic results and supported clinical staff involved in the care of patients who received a P/LP result. The medical geneticist (N.M.L.) and research coordinator (V.H.) were members of the study team and are co-authors of this report. We included them as participants in this study given their critical roles in patient care and provider support, and to capture their insights into potential operational challenges associated with providing genomic screening in a community-based health center.
Interviews were conducted by 2 experienced qualitative researchers (R.R.S., E.J.S.), who asked providers to comment on their experiences caring for recipients of P/LP results. Interviewees were also asked to reflect more broadly on their perceptions of the potential benefits and challenges of integrating precision medicine into their clinical practice. All interviews were audio-recorded and transcribed verbatim by a professional transcription service. Two members of the research team (T.S., E.J.S.) read the transcripts and conducted a descriptive, thematic analysis. The first author wrote detailed thematic memos, which were reviewed and revised iteratively by the analytic team (T.S., E.J.S., R.R.S.).
Results
Genomic screening was provided to 500 patients at MPHC. Of these individuals, ten were found to have a P/LP result. 17 Table 1 highlights the diversity of clinical management scenarios associated with reporting medically actionable genomic screening results and provides a summary of select patient health histories, genomic results, clinical management options, and recommended follow-up care. These cases illustrate the types of care-coordination challenges that PCPs may encounter when genomic screening is offered at a community-based health care center like MPHC.
Illustrative Cases of Genomic Screening Results and Their Management at a Community Health Center.

Petrucelli N, Daly MB, Pal T. BRCA1- and BRCA2-Associated Hereditary Breast and Ovarian Cancer. 1998 Sep 4 [Updated 2016 Dec 15]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020.
National Comprehensive Cancer Network. Genetic/Familial High-Risk Assessment: Breast and Ovarian (Version 3.2019). https://www2.tri-kobe.org/nccn/guideline/gynecological/english/genetic_familial.pdf. Accessed April 27, 2020.
Dietz H. Marfan Syndrome. 2001 Apr 18 [Updated 2017 Oct 12]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020.
Antoniou AC, Casadei S, Heikinnen T, et al. Breast-Cancer Risk in Families with Mutations in PALB2. NEJM. 2014 Aug 7; 371: 497-506.
National Comprehensive Cancer Network. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic (Version 1.2020). https://jnccn.org/view/journals/jnccn/18/4/article-p380.xml. Accessed April 27, 2020.
National Comprehensive Cancer Network. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic (Version 1.2020). https://jnccn.org/view/journals/jnccn/18/4/article-p380.xml. Accessed April 27, 2020.
Schneider K, Zelley K, Nichols KE, et al. Li-Fraumeni Syndrome. 1999 Jan 19 [Updated 2019 Nov 21]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020.
Wilde AAM, Amin AS. Clinical Spectrum of SCN5A Mutations. JACC: Clinical Electrophysiology. 2018 May; 4(5): 569-579.
Brugada R, Campuzano O, Sarquella-Brugada G, et al. Brugada Syndrome. 2005 Mar 31 [Updated 2016 Nov 17]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020.
Alders M, Bikker H, Christiaans I. Long QT Syndrome. 2003 Feb 20 [Updated 2018 Feb 8]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle, WA: University of Washington, Seattle; 1993-2020.
The medical geneticist returned genomic screening results to 9 of the 10 patients with P/LP results (One participant was scheduled to receive screening results, but presented for their appointment in severe psychological distress due to unrelated personal circumstances. Given these circumstances, the health care team decided that the disclosure of genomic screening results should be postponed. However, subsequent attempts to return those results have not been successful). Immediately following their appointment with the medical geneticist, patients met with a behavioral health provider to assess their psychosocial needs and support. At that time, an appointment was scheduled with a PCP to discuss clinical management and follow-up care. Seven of the nine patients who received P/LP results attended their appointment with a PCP.
At the time we scheduled interviews to discuss provider experiences, one of the MPHC PCPs had retired and another had left MPHC. We were able to interview all of the remaining five PCPs, the medical geneticist, and the primary clinical research coordinator for a total of seven participants. Interviews ranged in length from 15 to 120 minutes.
Benefits of Genomic Screening
All interviewees felt that implementing genomic sequencing at MPHC had benefited patients, providers, and the community at large. They emphasized the value of genomic screening to identify unknown risk factors. Several providers also mentioned that screening for familial susceptibility to cancer or heart conditions can raise awareness of the importance of regular medical monitoring and engagement with healthcare providers. Providers noted that by implementing screening for younger, asymptomatic patients, providers might be able to contextualize patients’ health behaviors in terms of personalized risk. They also noted that those screened might influence the behavior of their at-risk family members and others in the community. Providers often remarked that genomic screening was closely aligned with the goals of primary care, which include proactive health monitoring and the cultivation of positive health behaviors: “[The patients], they wanna take a proactive measure and know, ‘Hey, do I have a predisposition to some kind of genetic disorder, and could my family benefit from knowing this information?’” (ID5)
Other benefits noted by interviewees included the perception that genomic screening could serve as an educational tool to empower individual patients and their families to learn more about disease risks. Specifically, interviewees felt genomic screening could be useful in discussing family health histories and addressing knowledge gaps regarding disease histories: “People don’t actually know their family history beyond their first-degree relatives for the most part. They may have died of cancer in Mexico, but Lord knows what it was. You can’t get records” (ID7). Several providers also remarked that genomic screening could help improve health literacy for patients and their families. Interviewees felt that patients who pursued genomic screening might be better positioned to engage with clinical information and understand the interplay of genetic and lifestyle factors on their health outcomes: “[Even] if they do nothing, no action, they at least know a little bit more about genetics” (ID6).
The perceived benefits of genomic screening were not limited to patients and their families. Some providers expressed a personal desire to remain at the cutting-edge of primary care medicine and viewed their involvement in translational research as critical to that end: “If you don’t get involved with research, you kind of get left behind” (ID7). Other providers viewed learning more about precision medicine as critical to their practice: “That’s where medicine is going if we like it or not” (ID4).
Given the breadth of genomic screening, and the diversity of potential patient management scenarios, PCPs greatly appreciated the tailored genomics education they received for their patients from the medical geneticist supporting the genomic screening initiative. Several providers acknowledged a lack of familiarity with genomic screening methods and the genes evaluated in the study: “I wasn’t really aware of how far or how, um, advanced some of these tests and interpretations has gotten, really” (ID1). They described the clinical decision support that the medical geneticist provided as invaluable, particularly in relation to advice on clinical management and medical monitoring plans.
Challenges Encountered in Offering Genomic Screening
Providers described several struggles and frustrations that they encountered, particularly related to reporting genomic results and coordinating follow-up care. A common challenge was difficulty contacting patients and conveying a sense of urgency to come into clinic to discuss their results and arrange for follow-up care: “She never answered the phone. She never responded to the letter” (ID6). Providers reported similar challenges contacting at-risk family members and encouraging them to come in to discuss genetic testing options.
Several providers voiced concerns about their patients’ capacity to pursue recommended follow-up care due to financial constraints. This was noted as a source of considerable personal distress to the PCPs. Since many patients who receive care at MPHC are underinsured, providers worried that patients with P/LP variants would not have sufficient insurance to cover the costs of follow-up care. As a result, those patients might be left with a difficult decision to either pay out-of-pocket expenses or forego recommended diagnostic evaluations or procedures: “Most of these patients can hardly afford their blood pressure medicine so I don’t expect them to afford expensive procedures” (ID4). Providers described inadequate patient health insurance and a lack of subsidized government alternatives as significant barriers to patients accessing the care they need, as defined by clinical practice guidelines for the management of P/LP results.
This concern about patients’ inability to act on medical recommendations based on genomic results prompted several PCPs to question whether genomic screening should be offered to individuals who do not have the financial capacity to pursue follow-up care in the event of a positive result: “I have to be realistic. I mean, if we’re not gonna pay for it, we shouldn’t be ordering it” (ID3). This tension was experienced as a form of moral distress for some providers, exacerbated in instances when a patient or an at-risk family member did not appear for their follow-up clinical visit: “I wonder what my legal responsibility is if she hasn’t come back. I’d probably need to look her up and send her a certified letter to make sure she comes in. I was worried about her” (ID1).
Suggestions for Future Genomic Screening Initiatives
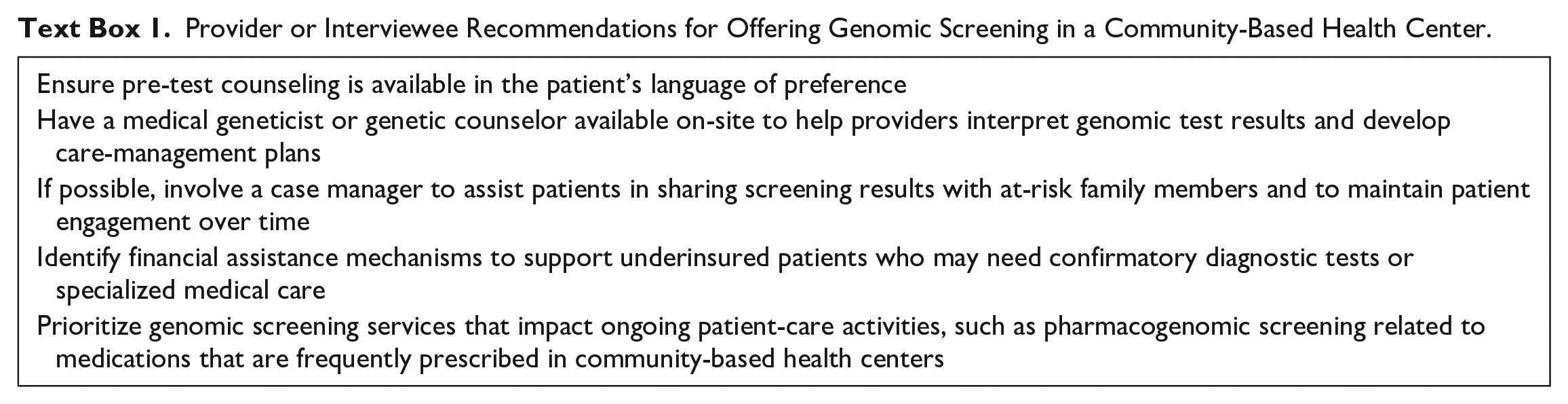
While opinions about the clinical impact of precision medicine varied among PCPs, with some voicing excitement and others apprehension, all of the providers we interviewed expected that their patients would have more questions related to genetic testing and genomic screening in the future. As providers reflected on their experiences counseling patients about genomic results, they had several suggestions to support future efforts to bring genomic screening to community-based health centers. Text Box 1 describes these recommendations, many of which were related to anticipating patient-support needs, including financial costs associated with additional diagnostic tests, and coordinating specialized medical care that might require referral to another healthcare facility.
Provider or Interviewee Recommendations for Offering Genomic Screening in a Community-Based Health Center.
Discussion
Our findings highlight tensions in bringing precision medicine to community-based health centers. On the one hand, PCPs wanted to ensure that individuals from lower-resource communities are part of the research driving the future of medicine, in part to ensure that their patients are able to benefit from those advances. On the other hand, financial constraints contributed to a number of clinical management challenges, resulting in moral distress and prompting some providers to ask whether it was ethical to offer genomic services in lower-resource settings.
Although providers noted the potential of genomic screening to provide their patients with clinical and preventive health benefits, they found it difficult to get patients and their family members to come in for primary care consultations and follow-up appointments. Additionally, many of the patients seen in the clinic lacked adequate health insurance coverage and the financial resources to pursue advanced diagnostic evaluations and specialized care available at referral facilities. These challenges are often faced by PCPs and other clinicians who practice in community-based health centers serving low-income populations, contributing to physician burnout and dissatisfaction.18-20 These and other burdens on providers are important to consider as new forms of precision medicine are integrated into primary-care clinics.
Even with the additional personnel and specialist support available through the collaboration with Mayo Clinic, PCPs experienced moral distress caring for patients who received medically actionable genomic screening results. The concept of moral distress has garnered considerable interest in the medical community, resulting in a growing body of scholarship examining moral distress resulting from the care of uninsured patients whose healthcare needs are not being adequately met.21-25 In our study, providers highlighted the challenge of getting uninsured and underinsured patients at high risk of disease the medical care they felt was necessary given their genomic results and cited concerns about the lack of state or federal funding to assist patients with insufficient financial resources to pay for recommended medical care. These challenges, combined with difficulties getting patients and family members to attend follow-up care appointments, were noted as significant contributors to providers’ moral distress.
Consistent with our findings, prior studies have underscored the difficulty of arranging financial coverage for cascade genetic testing (testing of at-risk family members of the proband after initial return of a P/LP variant).26,27 Addressing these and other health inequities in genetic medicine requires that we consider how best to make the potential benefits of precision medicine available to under-resourced communities.11,28,29 This sentiment was evident in our interactions with PCPs, all of whom expressed a strong interest in advancing community-based health by promoting genomic research, despite limited evidence of clinical utility in comparable settings and full awareness of the many challenges associated with the clinical management of patients who received a medically actionable result. A consistent sentiment among PCPs was enthusiasm for this research in genomic screening to learn more and consider how precision medicine might benefit their patients in the future.
Our findings also underscore a need for system-wide provider education and clinical decision support as a key element of integrating genomic screening into community-based health centers. Even when the medical implications of genetic test results are reviewed directly with patients (as they were in our study), future providers will have access to this information via the electronic health record and will need to be prepared to integrate those genetic test results into ongoing patient care activities. All of the PCPs we interviewed expressed a lack of familiarity with clinical genetic testing and the management of positive genomic screening results prior to this study, which is consistent with the broader literature.6-8 Similarly, other genetic implementation studies in primary care settings have demonstrated a clear need for ancillary physician education, often through partnerships with academic medical centers.30-32 These academic partnerships can also help to address infrastructure limitations, for example, by providing referral options for complex patients who would benefit from additional evaluation.33-35 While productive, this reliance on outside academic institutions raises questions about the long-term sustainability of genomic screening as a service provided by community-based health centers. Empowering on-site PCPs through genomic education and clinical decision support integrated into the EHR may provide more stable long-term support for the integration of precision medicine into community-based health centers.35,36
Lastly, our findings suggest that precision medicine may not integrate seamlessly into community-based health centers that support medically under-resourced communities. As advocates of precision medicine seek to expand its reach to include underrepresented populations in biomedical research, it will be critical that they evaluate experiences at community-based health centers. While there are many potential benefits of incorporating genomic screening into primary care, the burdens on patients and their PCPs may be considerable in lower-resource settings. 37
It is important to note the limitations of our results. This study examined the experiences of PCPs caring for Latino patients at a single community-based health center serving a primarily low-income patient population. Although we interviewed all of the available PCPs at MPHC who cared for a patient with an actionable genomic screening result, the experiences of these providers may not be typical of PCPs at other facilities or in other communities. Additionally, since 2 of the 9 patients had limited healthcare interactions after receiving their genomic results, the experiences of their PCPs may not be typical of other providers caring for patients with medically actionable screening results.
Despite these limitations, our findings help to address a significant gap in available scholarship by describing provider perspectives on the integration of genomic screening into community-based health centers, a setting in which patients are rarely offered new forms of precision medicine despite the potential for genomic screening to improve their health through the identification of unknown, but medically manageable risk factors.
Conclusion
Avoiding potential inequities that might result from advances in precision medicine will require creative approaches to delivering genomic services. By examining the potential benefits and challenges of offering genomic screening in community-based health centers, particularly health centers that support lower-income patients from diverse racial and ethnic backgrounds, we can transform what might otherwise be a highly disruptive and potentially discriminatory technology into a useful, positive influence on patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Institutes of Health, USA (U01 HG006379) and by the Mayo Clinic Center for Individualized Medicine.