
Abstract
Introduction
Diabetes mellitus contributes greatly to the global health burden of this century. The prevalence of type 2 diabetes mellitus (T2DM) has been escalating in the developing countries. 1 Diabetes, which was initially an entity in developed countries and in the urban area, has now percolated deeply in developing countries and into the periurban and rural areas. 2 Ten-year trend in the prevalence of T2DM shows that the rise in prevalence of diabetes in towns and periurban villages is significantly more than the rise of prevalence in the urban areas. 3
Despite the availability of effective antidiabetic drugs and regimens, achieving glycemic goals remains a great challenge. Individualized therapy and comprehensive disease management strategies are recommended to slow the progression of T2DM and to achieve glycemic targets.4,5 As indicated in the DCCT 6 study and the UKPDS 7 study, it is essential to maintain tight glycemic control during the treatment of T2DM in order to prevent complications. These studies aim at achieving a target HbA1c (glycated hemoglobin) of ≤7% while treating T2DM. However, there are many barriers to maintain such glycemic targets. One of the main barriers is hypoglycemia. Randomized controlled trials namely ADVANCE, 8 VADT, 9 ACCORD, 10 revealed a 3-fold increased risk of hypoglycemic episodes while trying to maintain glycemic goals. Such episodes of hypoglycemia are associated with increased incidence of cardiovascular events and mortalities. 10 The American Diabetes Association (ADA) recommends that plasma glucose-level maintenance need not be too strictly followed especially while treating long-term diabetic patients and the elderly individuals with comorbidities and that it is essential to treat patients in such a way as to minimize the risk of developing hypoglycemia. 11
ADA and European Association for the Study of Diabetes (EASD) guidelines recommend hypoglycemia risk to be considered while treatingT2DM patients. 12 It is established that the primary cause of hypoglycemia among T2DM patients is medications, namely sulfonylureas and insulin in 90% of the diabetic patients.13–16 However, hypoglycemia may occur due to other causes apart from medications, which needs to be explored. Patient’s well-being can get affected directly due to hypoglycemic symptoms and indirectly due to fear of subsequent hypoglycemic episodes. 17 Even mild symptoms of hypoglycemia can affect the treatment of T2DM if patient’s fear of hypoglycemia overtakes the willingness to take medications. 16 Recurrent hypoglycemic episodes can lead to poor quality of life, 17 increased anxiety, depression, and mood swings. 18 ADA Work Group on T2DM has coined a term, “Probable Symptomatic Hypoglycemia” where the exact value of the glucose levels need not be measured. Reporting details of such episodes is required in achieving better control of plasma glucose levels. 19 Hence, identifying self-reported symptoms of hypoglycemia is a practical approach to estimate the prevalence.
India, which ranks second in terms of diabetic population in the world, 20 with more than 72 million people living with T2DM in 2017, 21 the problem of hypoglycemia, appears to be a neglected entity. In affluent states of India like Tamil Nadu, 2 where there is established spread of T2DM to the economically weaker sections of the society, there is need for research about hypoglycemia. Although there are various studies to indicate hypoglycemia as a complication in treatment of T2DM, data regarding the prevalence of such episodes is lacking in Indian rural setting. Thus, in our study, we intend to estimate prevalence of hypoglycemia among T2DM patients, who receive treatment from a rural health center in Tamil Nadu, India. The study outcome will definitely benefit all the primary care physicians, as they are the first contact physicians of the rural community and play a major role in identifying and treating patients with hypoglycemia. This will also guide them to provide patient education regarding the symptoms of hypoglycemia and its management.
Objectives
To study the self-reported prevalence of hypoglycemia among patients with T2DM.
Materials and Methods
Study Setting
The study was conducted from January 2017 to March 2017 at the Rural Health and Training Centre (RHTC), Vayalanallur of Poonamallee block, Tamil Nadu, India. The center is directly under Department of Community Medicine of Sri Ramachandra Institute of Higher Education and Research (SRIHER), Chennai, Tamil Nadu, India.
Study Design and Population
This was an institute-based cross-sectional study. All T2DM patients with more than 6 months duration, who had their follow-up visit from January 1, 2017 to March 31, 2017, were included in the study. Patients with T1DM, gestational diabetes, and newly diagnosed within the past 6 months were excluded.
Study Variables and Measurements
Prevalence of hypoglycemia was assessed based on a pretested structured questionnaire in which all the possible symptoms of hypoglycemia were included.21-24
Whipple’s triad is a collection of 3 criteria termed as Whipple’s criteria, which suggests that a patient’s symptoms result from hypoglycemia. The essential conditions include the following:
Symptoms known or likely to be caused by hypoglycemia especially after fasting or heavy exercise
Low level of plasma glucose at the time of the occurrence of the symptoms
Relief of the symptoms once the glucose levels become normal
The common symptoms of hypoglycemia were enlisted. The patients were asked if they had ever experienced any one of the listed symptoms in the past 2 to 3 months. If the answer was yes, then they were enquired about the frequency of the above said symptoms. If they answered that they had experienced the symptoms at least 2 to 3 times in a month and the symptoms relieved on consuming food/sugar/juice, and so on, were considered to have had a hypoglycemic episode. As the patients are from rural areas, they do not have the facility of checking their plasma glucose with glucometer; only patient’s clinical history and symptomatic relief were taken into consideration for the estimation of prevalence of hypoglycemia. Hence, if the first and third criteria were met, the patients were identified to have had hypoglycemic episode. A hypoglycemic event which required assistance of another person or which required medical assistance in a hospital for corrective measures were documented as a severe episode of hypoglycemia. 11
Data Collection and Quality Control Measures
Approval by the Institutional Ethics Committee was obtained prior to the commencement of the study (reference number IEC-NI/16/NOV/56/81). Written informed consent was obtained from all the patients who were included in the study. The questionnaire included the sociodemographic variables of the patients, details of their disease condition and comorbidities, and details of hypoglycemic episodes. The content validity of the questionnaire was examined by an expert team of 3 endocrinologists under the guidance of the Head of Department of Endocrinology, SRIHER. The questionnaire was then translated to Tamil and then back-translated to English by language experts. Medical officers at RHTC, Department of Community Medicine, SRIHER did data collection after being briefed by the principal investigator. Each patient was interviewed for 30 minutes to obtain all the relevant information. All patients were clinically examined, and their blood was collected for estimation of HbA1c levels.
Data Processing and Analysis
Data entry and analysis of the variables was done using Statistical Package for Social Sciences (SPSS) version 16 software after checking for completeness. Descriptive statistics was used to analyze the background variables and using chi square, the associations of risk factors were analyzed. The odds ratios (ORs) and their 95% confidence intervals (CIs) were computed. A P value of <.05 was considered to be statistically significant.
Results
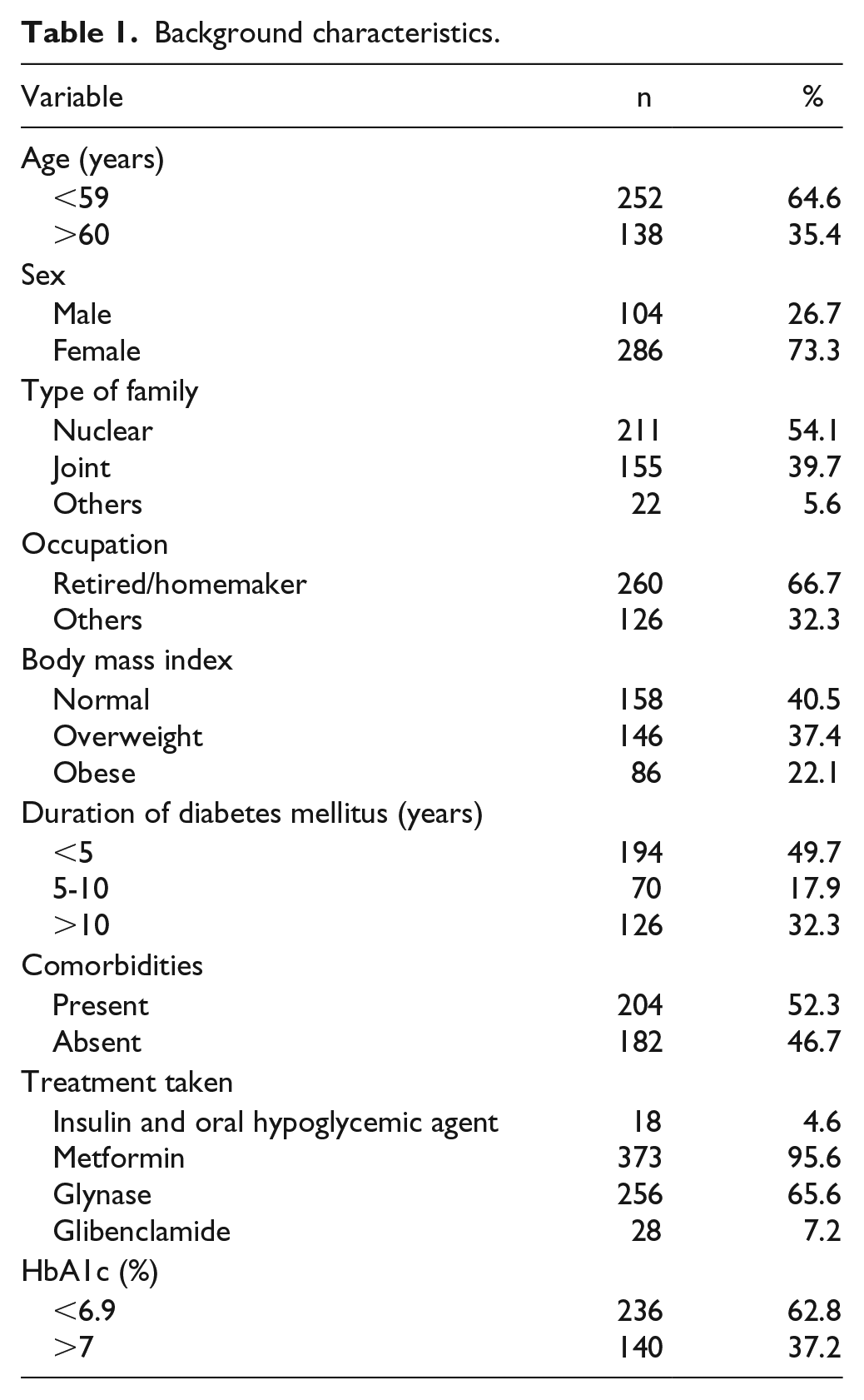
A total of 390 patients with T2DM were interviewed. The median age was 56 years. Most of the patients were female (73.3%). The family type was nuclear in 54.1% and majority of them were either retired or homemakers (66.7%). Among them, 34.6% of the patients were illiterate, 30% of them had completed only primary school, 30.8% had middle school education, 3.6% had high school education, and only 0.8% were graduates/postgraduates. The mean (SD) per capita income of the patients was INR2849 (INR3668) (USD1 ≈ INR70). Among the patients, 32.3% had diabetes for more than 10 years. Mean duration of diabetes was 6.83 years. Body mass index (BMI) of >25 kg/m2 was found in 57.9% of the patients. The mean (SD) of the BMI was 26.9 (11.45) kg/m2. The mean (SD) of HbA1c level was 7.27% (1.72%) and the maximum documented level was 13%. HbA1c levels were more than 6.5% in 56.4% of the study population. All patients were either on metformin or on combination of metformin with glibenclamide/glynase. Only 18 (4.6%) of them were on insulin along with oral drug combinations. Among the diabetic patients, 52.3% had some comorbidities like hypertension (41.8%), cardiovascular complications (4.4%), or renal problems (0.5%). The background variables are given in Table 1.
Background characteristics.
Hypoglycemic episodes were reported in 224 of the 390 diabetic patients. The prevalence of hypoglycemia was estimated to be 57.44% (95% CI 52.48-62.25) Among the 224 patients with hypoglycemia, 77.7% were female. Severe hypoglycemia requiring help from other persons or medical assistance for plasma glucose correction was prevalent among 24 (10.7%) patients who had hypoglycemia. Of those patients with severe episodes, hospital admission and plasma glucose correction were required for 7 (29.17%). A total of 11.6% of the hypoglycemic patients had symptoms daily; 21.9% of them had 2 to 3 episodes in a week, and almost half (48.2%) had 2 to 3 episodes a month, while it was rare among 18.3%. The details of the symptoms of hypoglycemia are in Table 2. The other symptoms were epigastric pain, nausea, and sleep (0.4%) each. The first symptom of hypoglycemia was dizziness, which was reported in 72.3% of the individuals. This was followed by sweating in 44.2% of them (Table 2). The most common self-reported etiological factor for the hypoglycemic episode was missing food or delayed food intake, which was seen in 200 patients (90%; Figure 1). The majority of them (56.7%) ate the missed-out meal and were relieved of the symptoms (Figure 2).
Most Common Symptoms of Hypoglycemia.

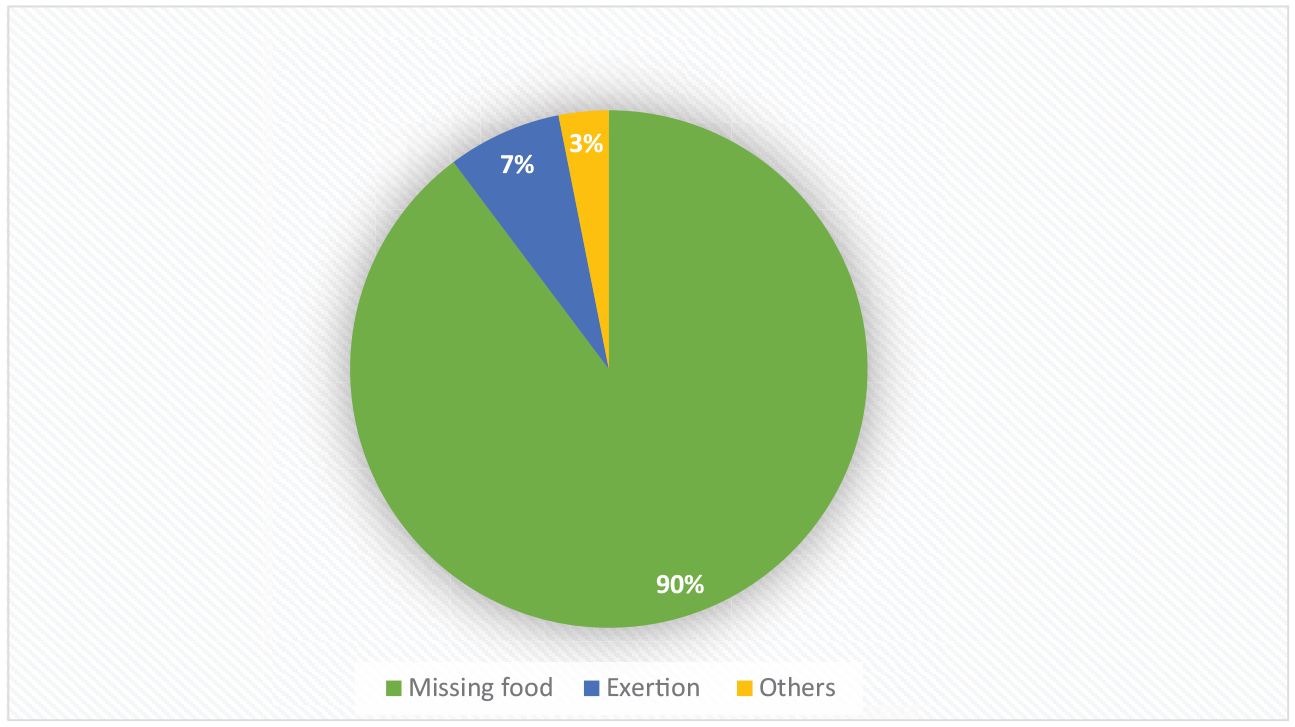
Self-reported etiological factors for hypoglycemia.

Action taken for hypoglycemia.
It was found that only 21.9% of the patients reported such symptoms to the medical practitioner. Moreover, only 23% of the diabetic patients carried glucose with them when they went out. Most of the patients (89.3%) who received treatment at the rural center checked their plasma glucose levels every 3 months. A total of 5.4% of them checked even more frequently and 5.4% of the patients did not check their levels regularly. None of them could afford a glucometer for self-monitoring their glucose levels. The present study showed that female patients were at a higher risk of developing hypoglycemia compared with the male patients (OR 1.2, 95% CI 1.04-1.3, P < .05). Patients with higher fasting blood sugar levels had an increased risk of hypoglycemic episodes; it was not statistically significant (Table 3).
Factors Associated With Self-Reported Hypoglycemia.
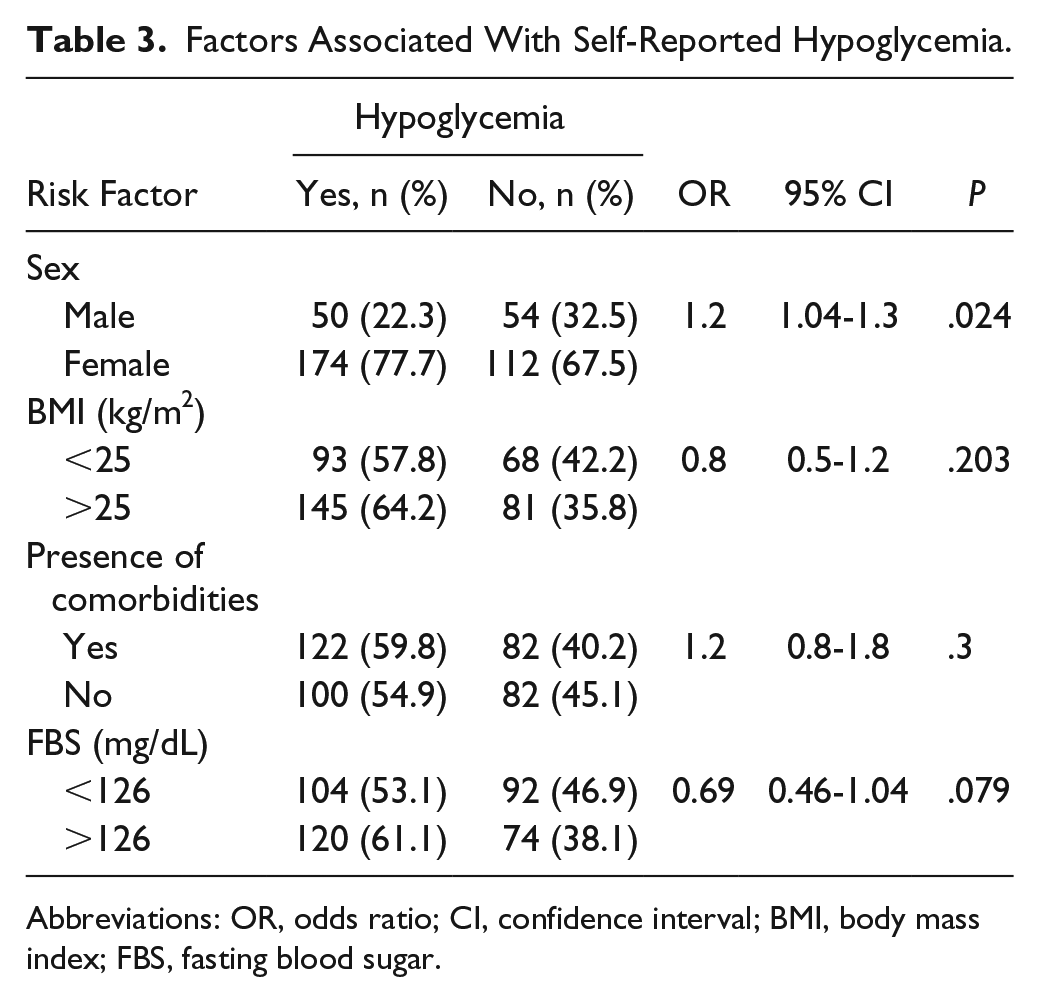
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; FBS, fasting blood sugar.
Discussion
The current study was a part of the project undertaken in a rural health center in Tamil Nadu with the objective to find the prevalence of self-reported hypoglycemia and its associated risk factors among all the patients with T2DM who were registered at the center. All patients with T2DM who were undergoing regular treatment at the center who consented were included in the study. The study results can be generalized to any primary health center or a diabetic clinic where patients are receiving treatment. This study was done in a primary health care setting, which is a common setting in the Indian population as it is where first contact of the patient happens with the physician. It was found that 224 patients (57.43%, 95% CI 52.48-62.25) had hypoglycemic episodes. The narrow confidence interval indicates that the study has good internal validity and sufficient sample size. Marrett et al 25 reported that 63 % of patients with T2DM had symptoms of hypoglycemic episodes of which 46% were mild, 37% moderate, 13% severe, and 4% very severe. Study by Shriraam et al 26 found the prevalence of any one symptom of hypoglycemia as 78.1% who fit in the operational definition of relief of symptom on intake of glucose. The study setting was in a tertiary care hospital where severe hypoglycemia was reported among 19% of the patients. However, in the present study, severe hypoglycemic episodes were less (10%). In another survey done by the American Association of Clinical Endocrinologists, 27 20% of the diabetic patients required assistance for hypoglycemic episodes and 6% required hospitalization for the same. The first symptom of hypoglycemia was dizziness followed by sweating in the present study. Similar first symptom of dizziness was reported in another study 26 in a tertiary care hospital.
Miller et al 28 conducted a retrospective interview among patients with T2DM and reported a prevalence of 16% hypoglycemia among patients on oral hypoglycemic agents compared with 30% prevalence among those on insulin therapy. In the rural setting, very few people (4.6%) were on insulin, hence the association of hypoglycemia with insulin therapy could not be established.
The most common situation where hypoglycemia developed was a missed meal, which was observed in 89.3% of the patients. Similar findings were observed in another study, 27 where 87% of the patients reported a missed meal as the etiological factor. This indicates the importance of education to the patients about consuming meals at the right time that would prevent episodes of hypoglycemia.
Women were at a higher risk of developing hypoglycemia. The reason for this could be that in Indian culture, women in general consume meals only after their spouses completes their meal. It is important to educate patients as well as the family members regarding timely meals in diabetic elderly women, which would help in preventing hypoglycemia.
Limitations
As the patients belonged to a lower socioeconomic status in a rural, low-resource setting, there was no possibility of measuring plasma glucose concentration at the time of the hypoglycemic episode. Therefore, the exact prevalence of these episodes is a challenge to measure. The accuracy of the prevalence of self-reported hypoglycemia may have been affected by patient recall especially when the event has been mild. 29 It could also be affected by the individual’s ability to identify the episode as a hypoglycemic event, as it is essential for the patient to differentiate hypoglycemic symptoms and other nonrelated symptoms. There is a possibility of underestimate of the exact prevalence.
As the most common cause of these episodes is a delayed or a missed meal, there is a possibility of this occurring in normal individuals also. These symptoms are more frequent and much exaggerated in diabetic patients, which require proper preventive measures.
Strengths
This is the first study done to estimate the prevalence of hypoglycemia in a rural health center where the resources are limited. This study throws light on the high prevalence of hypoglycemic episodes in the rural population. Even in the near future, it is impossible to document hypoglycemia by glucose measurement in India especially in a rural setting. This is the best way possible to document hypoglycemia.
Conclusion
Hypoglycemia is highly prevalent among the diabetic patients treated in the rural health center. It is to be noted that 10% of them had severe episodes of hypoglycemia. Only a fifth of the patients reported symptoms to the medical practitioner. This implies that it is essential for the primary care physicians to enquire about the symptoms of hypoglycemia to all the patients at every visit. It is highly essential to educate the diabetic patients about symptoms of hypoglycemia and the importance of reporting such episodes to the doctor. The patients should be emphasized about the importance of carrying glucose in hand to tackle hypoglycemic episodes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.