
Abstract
Keywords
Introduction
Atherosclerotic diseases, including acute myocardial infarction, are pathologies of great impact for health systems and generate a significant morbidity and mortality burden. It is estimated that in the year 2012, 17.5 million people died as a result of cardiovascular disease, and it is expected that by the year 2030, this figure will reach almost 24 million people. 1 In Colombia, cardiovascular disease represented the main cause of death in the period of 2005 to 2013, being responsible for 30% of deaths and 16% of all years of potential life lost, mainly related to the occurrence of acute coronary syndromes. 2
Many outcomes caused by coronary disease could be prevented if an effective intervention with nonpharmacological and pharmacological measures is applied, depending on the risk factors of each person. This may involve the use of statins and aspirin, the control of blood pressure with antihypertensive medications, and even the proper management of diabetes mellitus and any other related conditions. 3
Despite the benefits shown by some of the medications, it is estimated that many patients are not receiving them as part of their cardiovascular risk management. Furthermore, these drugs have usually been used in patients who already had major cardiovascular outcomes, losing the opportunity to use them as primary prevention strategies.4,5
The objective of the present study was to determine, in patients who suffered a first acute coronary syndrome, the use profile of statins and aspirin before such event (as a strategy for primary cardiovascular prevention).
Methods
A cross-sectional study was carried out. We identified patients affiliated with one healthcare insurer within the contributory (paid) scheme of the Colombian Health System, of any sex and >18 years, with a diagnosis of a first episode of acute coronary syndrome that occurred during the period of 2015 to 2016. The prescription of statins and aspirin before said event was reviewed, considering the recommendations of the Colombian dyslipidemia guidelines 6 and the United States Preventive Services Task Force (USPSTF) guide for aspirin in primary prevention. 7 The information was obtained from the clinical records provided by the insurer and the medication claim data from the company Audifarma SA (largest drug dispensing company in the country).
From a population of 1 405 800 patients affiliated with the insurer, we identified a total of 1894 adult patients who suffered a first episode of acute coronary syndrome between January 2015 and December 2016. From these patients, and in order to review individual clinical records, a representative simple random sample of 322 cases was selected, using 5% as an acceptable margin of error and a confidence level of 95%. Patients without a clinical history prior to the coronary event were excluded from the study.
Based on information from clinical and drug dispensing records, a database was designed with the following variables: 1) Sociodemographic and anthropometric: sex, age, education level, and body mass index (BMI). Obesity was defined as patients with a BMI ≥30 kg/m2. 2) Comorbidities: hypertension, type 2 diabetes mellitus, chronic kidney disease, hypothyroidism, peripheral arterial disease, smoking, and chronic obstructive pulmonary disease. 3) Clinical and laboratory data: whether or not recommendations were received about healthy lifestyles or exercise, or having had a consultation with a nutrition professional before the coronary event. The values of systolic blood pressure (SBP, in mmHg), glycated hemoglobin (HbA1c) and cholesterol (total, high-density lipoprotein [HDL] and low-density lipoprotein [LDL] cholesterol, in mg/dL) were collected. For the review of the lipid profile, recommendations on lifestyles and healthy diet, and nutritionist evaluation, the reports up to 1 year before the coronary event were considered. 4 ) Pharmacological: use of statins, aspirin, antihypertensives, antidiabetics and their respective doses (mg/day), and use of comedications, including bronchodilators, psychotropic drugs, non-steroidal anti-inflammatory drugs, anti-ulcer drugs, and levothyroxine. 5 ) Cardiovascular risk: the corrected Framingham cardiovascular risk score for Colombia, 8 the cardiovascular risk score according to the American Heart Association (AHA) protocol 9 and the need for use (yes/no) of statins and aspirin in primary prevention.
For the definition of the requirements for the use of statins in primary prevention, the recommendations classified as “strong in favor” were taken into account, from the Colombian dyslipidemia guidelines. 6 For people in need of statins at a high intensity dose, the following was included: having LDL cholesterol >190 mg/dL (>4.9 mmol/L); having a diagnosis of diabetes mellitus, age over 40 years, an associated cardiovascular risk factor and LDL cholesterol >70 mg/dL (>1.8 mmol/L); or having an estimated cardiovascular risk >10% at 10 years, according to the adjusted Framingham score for Colombia. The need for moderate intensity statins included people with diabetes mellitus, age older than 40 years, with LDL cholesterol >70 mg/dL and without criteria for intensive therapy.
A “misuse of statins” was considered for patients who needed their prescription and were not receiving it before the coronary event, according to the Colombian guidelines. To define the need for the use of aspirin, the updated USPSTF grade B recommendation was considered: use of aspirin at low doses in patients between 50 and 59 years old with a risk of 10% or more of developing a cardiovascular event in 10 years (according to the risk score of the AHA 2013 [pooled cohort equations]). 7 In addition, patients with the need for aspirin who were between 60 and 69 years of age were identified (grade C).
A patient with hypertension was considered under control if the blood pressure values before the coronary event were less than 140/90 mmHg. In patients with diabetes mellitus and chronic kidney disease, levels under 130/80 mmHg were considered to be under control. Regarding diabetes mellitus, a patient was considered controlled if the glycated hemoglobin level prior to the coronary event was ≤7.0%.
The protocol was endorsed by the Bioethics Committee of the Universidad Tecnológica de Pereira and was classified in the category of “risk-free research” according to national laws. Personal data of the patients were not used, and their identity was safeguarded following the principles established by the Declaration of Helsinki. Code: CBE-SYR-162016.
Data Analysis
Descriptive statistics were used for the analysis of the data, using the statistical package SPSS version 24.0 (IBM, USA) for Windows. Bivariate tests were also performed for the comparison of quantitative variables; X 2 test was used for the categorical variables. We performed a non-parsimonious, exploratory binary logistic regression model, using as a dependent variable the misuse of statins (yes/no). The covariates in these models included age, sex and those that were significantly associated with the dependent variable in the bivariate analysis. The level of statistical significance was P < .05.
Results
We included 322 patients who met the inclusion criteria. The mean age was 61.9 ± 10.8 years and 77.3% (n = 249) were men. There were 125 patients (38.8%) aged 65 years or older, and only seven patients were of African descent (2.2%). None of the events analyzed presented a fatal outcome. Table 1 describes the main characteristics of the study population.
Sociodemographic, Anthropometric and Comorbidity Characteristics of Patients with a First Coronary Event for One Insurer in Colombia, 2015 to 2016.

Abbreviations: BMI: body mass index - kg/m2; COPD: Chronic Obstructive Pulmonary Disease; IQR: interquartile range; PAD: peripheral arterial disease; SD: standard deviation.
There were 287 patients (89.1%) with some of the comorbidities examined, especially dyslipidemia, hypertension and type 2 diabetes mellitus. In addition, it was identified that one third of the population were smokers (Table 1). The median systolic blood pressure was 120 mmHg (interquartile range [IQR]: 110-130 mmHg), without significant differences according to sex or the age group of 65 years or more.
During the pre-infarct visits, a total of 252 patients (87.8%) received recommendations for healthy lifestyles. In the year prior to the date of the coronary event, 108 patients (33.5%) were assessed by a nutritionist, especially those with obesity (OR: 1.89, 95% confidence interval [95%CI]: 1.10-3.24).
Only 197 patients (61.2%) had complete reports for total, LDL and HDL cholesterol before the coronary event. Among these, the mean total cholesterol was 202.4 ± 54.2 mg/dL, mean LDL cholesterol was 125.9 ± 46.6 mg/dL and mean HDL cholesterol was 40.0 ± 9.3 mg/dL (median of 39.0 mg/dL, IQR: 34.0-46.0 mg/dL).
Calculation of Cardiovascular Risk and Use of Drugs for Primary Prevention
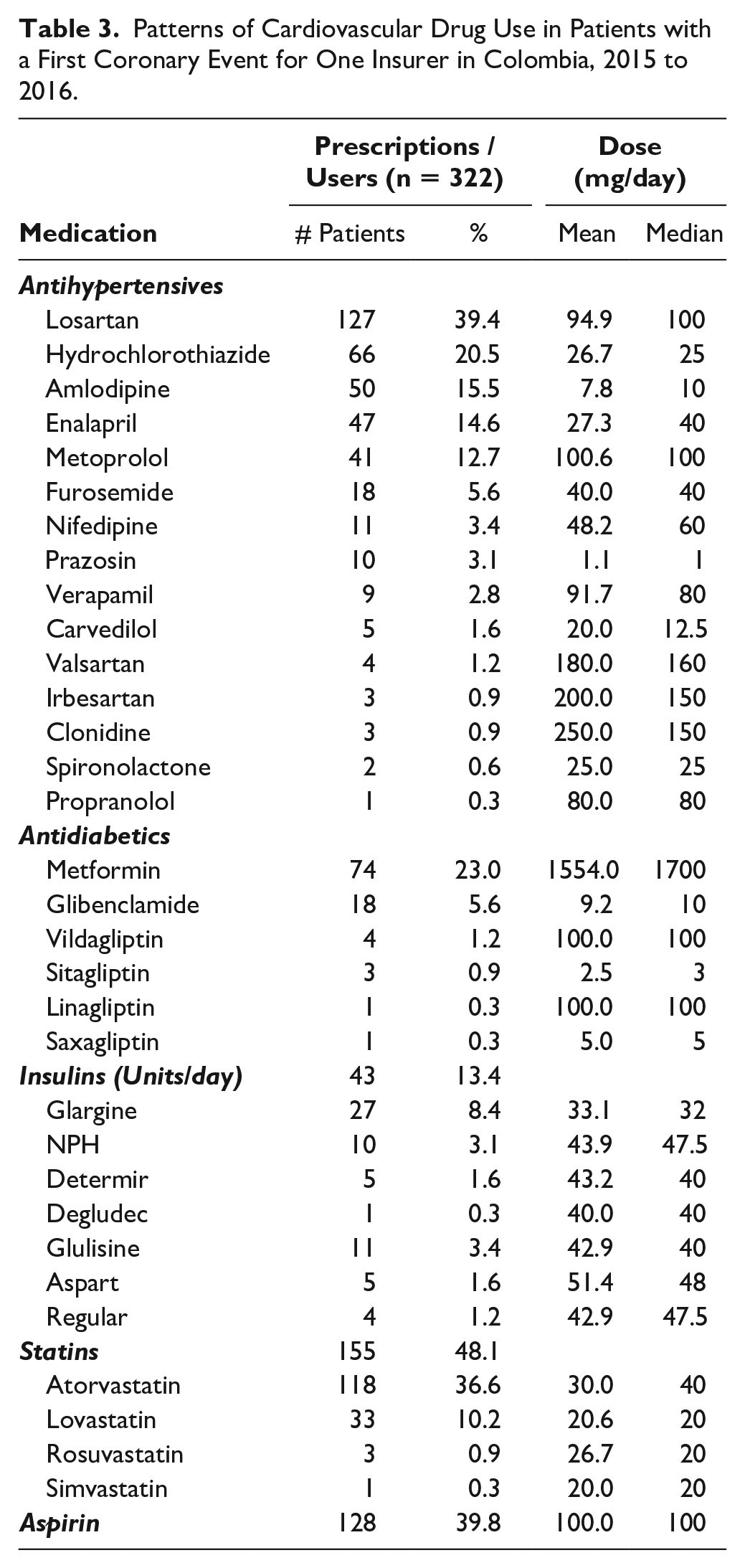
The cardiovascular risk score was calculated in 211 patients (65.5%) who had the necessary variables complete. The median Framingham risk score adjusted for Colombia was 21.4% (IQR: 11.7%-22.5%), while the median cardiovascular risk according to the AHA scale was 16.3% (IQR: 9.1%-28.6%). According to the recommendations of the Colombian guidelines, 179 patients (84.8%) needed a statin in primary cardiovascular prevention. It was found that 155 patients (48.1% of the total number of participants studied) were receiving statins before the coronary event, of which 63 (40.6% of those with statins) received high intensity doses. However, according to the cardiovascular risk results and the recommendations of the Colombian guidelines, 175 cases (97.8% of those requiring statins) with a calculable cardiovascular risk score should have been receiving high intensity statins, and 56 patients (31.3% of those who needed them) were not receiving the statin, which was considered a misuse of this group of medication (Table 2). On the other hand, 48 patients (27.4%) were adequately receiving high intensity statins (Figure 1). Atorvastatin was the most used statin, followed by lovastatin (Table 3).
Comparison Between Users of Statins and the Need for Use According to the Recommendations of Clinical Guidelines in Patients with a First Coronary Event for One Insurer in Colombia, 2015 to 2016.

Abbreviation: AHA: American Heart Association.

Consumption proportion of the different medications useful in the management of cardiovascular risk and in primary prevention based on the need for use according to the guidelines evaluated, in patients with a first coronary event for one insurer in Colombia, 2015 to 2016.
Patterns of Cardiovascular Drug Use in Patients with a First Coronary Event for One Insurer in Colombia, 2015 to 2016.
In the exploratory binary logistic regression model, it was found that patients diagnosed with dyslipidemia were more likely to adequately receive a statin (Hosmer-Lemeshow test P = .735, Nagelkerke’s R squared .294) (Figure 2).
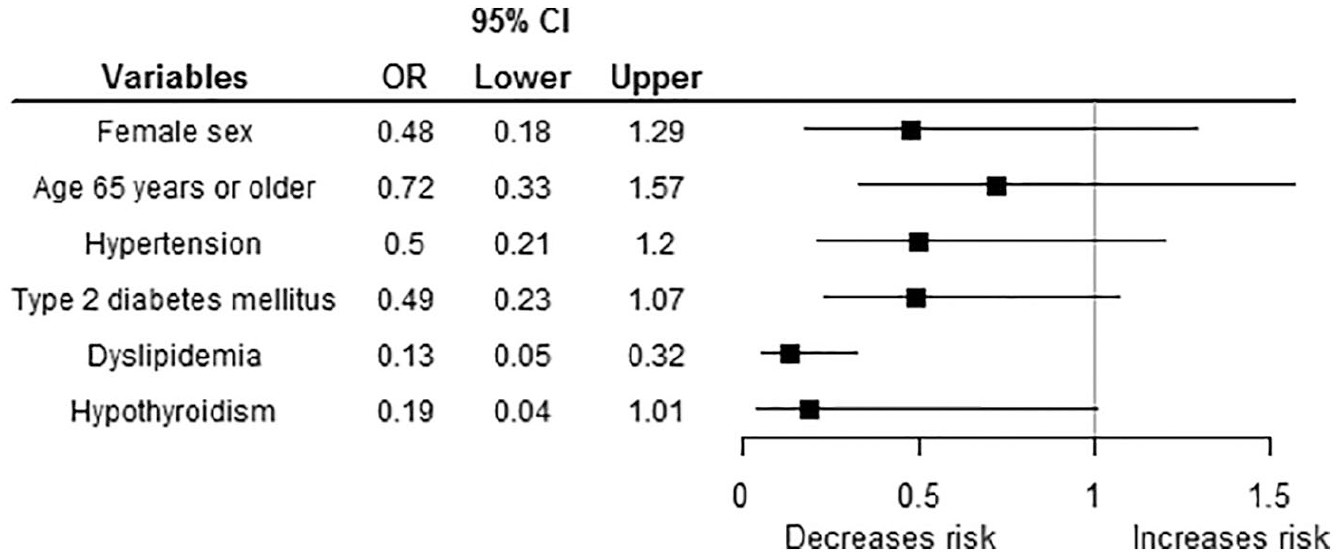
Variables related to the misuse of statins in the binary logistic regression model for patients with a first coronary event for one insurer in Colombia, 2015 to 2016.
Regarding the use of aspirin, it was found that 128 patients (39.8% of the total population) were receiving aspirin, all of them at a dose of 100 mg/day. Of the 211 patients with a calculable cardiovascular risk, 88 (27.3%) should have received aspirin in primary prevention according to USPSTF recommendation; it was found that 38 patients of the 88 (43.2%) with an indication for aspirin use were not receiving it (Figure 1). Conversely, 61 patients (28.9% of the 211 with calculable risk) were prescribed aspirin without indication.
Comorbidities
Of the 202 patients diagnosed with hypertension, 195 (96.5%) were receiving at least one antihypertensive medication, the most frequently prescribed being losartan, followed by hydrochlorothiazide, amlodipine, and enalapril (Table 3). Of the hypertensive patients, 142 (70.3%) presented blood pressure values within the goals.
A total of 91 of the 97 patients (93.8%) with type 2 diabetes mellitus were receiving some antidiabetic medication, with an average of 1.5 ± 0.7 drugs per patient. There were 45 patients (46.4%) who used a single antidiabetic, 39 (40.2%) who used two and seven who received three (7.2%). The most frequently prescribed medication was metformin, followed by insulin and glibenclamide (Table 3).
The HbA1c registry was missing for 10 of the patients (10.3%) with diabetes mellitus. In the remaining 87, the median HbA1c was 7.5% (IQR: 6.5-9.4), and only 35 of the cases (36.1%) were within the treatment goals. Table 3 shows the use patterns of medications related to cardiovascular disease that were being used in the study patients.
The most frequently prescribed comedications were proton pump inhibitors in 76 patients (23.6%), followed by acetaminophen (n = 69, 21.4%) and nonsteroidal anti-inflammatory drugs (n = 57, 17.7%).
Discussion
Main Finding of this Study
Given the significant burden of morbidity and death that acute myocardial infarction represents worldwide, the identification of patients who, due to their cardiovascular risk, required specific medications to prevent the coronary event but were not receiving them becomes a relevant issue for any public health system. In this case, it could be established that a third of the patients who needed statins and 40% of those who may have required aspirin did not receive them before the acute coronary event.
The characteristics of the patients included in this study are similar to the results reported nationally and globally, such as mean age, sex, BMI, and associated comorbidities that get involved in cardiovascular outcomes. It was found that the most frequently associated comorbidity was dyslipidemia, followed by arterial hypertension. Recently, Álvarez-Ceballos et al found that in a group of Colombian patients seen in primary care, 76% had high blood pressure, highlighting the frequency of this pathology in our population, while diabetes mellitus was found in 22% of their study population 10 as well as ours.
More than 70% of the patients with arterial hypertension had blood pressure values within the goals, compared with previous studies of cardiovascular disease in Colombia that showed a control rate of 82%. 11 In the case of diabetes mellitus, only 36% were within HbA1c goals, a lower proportion than the 57% in the study conducted by Machado-Duque et al in patients treated by the same insurer. 12 This should highlight the importance of achieving adequate control of these pathologies given that, in the group of patients with a coronary event included in the study, both pathologies presented lower proportion of control than those of previous analyses. Additionally, it should be noted that the control measures of other determinants, such as obesity, were apparently insufficient, as only one third of the patients attended a nutrition evaluation in the year before the coronary event.
Many of the patients who were evaluated did not have enough data to be able to determine the risk score, which, more than a study limitation, suggests the importance of its periodic measurement, especially when the mean age exceeds 60 years.
It was also found that of the patients who were receiving statins, the most prescribed was atorvastatin, which is similar to the results reported by studies in the United States and Taiwan.13,14 A study conducted by Rosselli et al showed that the most cost-effective strategy for Colombia is achieved with the prescription of atorvastatin compared with the other statins, so its preference as found in the present work seems to be appropriate. 15
The limited prescription of cardiovascular therapies in the context of secondary prevention has been widely described. For example, Bennett et al found in an Irish population that only 37% of patients with diabetes and coronary heart disease were receiving statins. 16 Yusuf et al also found that this low prevalence of use occurs more frequently in low and middle income countries, such as Colombia. 17 However, in the field of primary prevention, studies are scarce.
A study conducted in the United States found that only 20% of patients with a 10-year cardiovascular risk score greater than 20% were receiving the necessary drugs to address the risk. 4 Kulenovic et al described that in Denmark, the use of statins in primary prevention before the development of acute myocardial infarction was infrequent; however, the use of statins was much lower than that identified in the present work (approximately 12% vs 69%), which can be explained by the risk scale used and the inclusion criteria of that study, which collected only patients without a history of any cardiovascular disease (including diabetes). 18
The use of aspirin in primary prevention is still controversial. In this study we included the recommendations given by the USPSTF. Recent trials have found divergent results on the effect of aspirin for primary prevention, that varies according to baseline cardiovascular risks factors, specially the presence of diabetes mellitus.19,20 Thus, the use of aspirin in this setting should be still assessed carefully in the clinical context of each patient, considering its preferences and potentials risks, as stated in the recent clinical practice guidelines, 21 which limits the potential patients eligible for aspirin. On the contrary, in this study we found patients using aspirin without any indication, which should also be reviewed to avoid unnecessary bleeding risk.
The current study presents several limitations for the generalizability of its results. Only patients from one insurer in the country were included, so the results can be applied to populations with similar demographic and health care characteristics. A third of the analyzed cases did not have all the necessary variables to perform the calculation of cardiovascular risk scores, which can be seen as an important finding that indicates shortcomings in the approach toward patients in follow-up consultations and morbidity management (ie, high blood pressure, diabetes mellitus, and dyslipidemia). As a strength, the individualized review of each patient’s clinical records should be highlighted, allowing to identify in general all the other variables under study, including the doctor’s recommendations regarding changes in lifestyle.
Conclusion
With the above findings, it can be concluded that only approximately two thirds of the population who had a first acute coronary event had sufficient information in their clinical records to qualify their 10-year cardiovascular risk. Of these, their median cardiovascular risk scores measured with different scores were high; 85% required the use of a statin for primary prevention, but only two thirds actually received it, and at insufficient doses in most cases. In addition, a high proportion of patients that may have required a platelet antiaggregant for the same purpose were not receiving it, which, added to the insufficient results in the control of diabetes mellitus and arterial hypertension, can explain the outcome of the cases included. Based on these results, it is essential to implement measures that encourage primary care physicians to measure the cardiovascular risk levels of their patients and prescribe the appropriate medications to reduce the probability of an acute coronary event.
Footnotes
Author Contributions
AGV participated in the drafting, data collection, data analysis, description of results, discussion, critical revision of the article, and evaluation of the final version of the manuscript. JAZC participated in the drafting, data collection, data analysis, description of results, discussion. AARB participated in the drafting, data collection, data analysis, description of results, discussion. CLBP participated in the drafting, discussion, and critical revision of the article. JEMA participated in the drafting, data analysis, description of results, discussion, critical revision of the article, and evaluation of the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received support from the Fundación Universitaria del Área Andina and Audifarma SA.