
Abstract
The prevalence of childhood obesity continues to rise despite decades of clinical and public health efforts. Early identification of children at risk of developing obesity is essential using newer electronic health systems, which move beyond traditional growth charts to provide a wealth of information about body mass index and other relevant parameters such as social determinants of health and comorbid conditions. For children who already have obesity, there are several evidence-based strategies health care providers can use as they work with patients and families to mitigate the effects. First and foremost, providers should address the issue; unfortunately, weight is often not discussed in clinical practice. In addressing the issue, providers should support families through effective, positive relationships. Providers must be aware of their biases; their language should be appropriate and nonstigmatizing. Helpful interventions should focus on behavior, not weight, health, or appearance. Motivational interviewing may be used to promote healthful behaviors: supportive parenting, regular exercise, healthful food choices, minimal screen time, and optimal sleep. There is limited evidence for the efficacy of specific weight loss diets. Both medication and bariatric surgery are indicated for select adolescents who have severe disease unresponsive to behavioral management.
Introduction
Currently, there are 13.7 (around 17% of US population) million children and adolescents with obesity. Children with obesity face a lifetime of physical and psychological complications, yet this condition is often ignored and under addressed at most office visits.1,2 Many reasons have been proposed for this gap in care services, including lack of effectiveness of any currently available interventions, lack of engagement, availability, or affordability of the recommended intensive interventions, and provider discomfort. Nonetheless, these children and families need optimal clinical care to mitigate the effects of obesity. Accordingly, this future guideline development for primary care providers identifies those components of family-centered advice and support that are supported by evidence. The framework to effectively deliver family-centered care should include screening and early detection for obesity and associated risk factors and comorbid conditions; supporting children with obesity and their caregivers while mitigating bias and stigma; and focus on behavior change as the primary intervention.
Screening and Early Identification for Obesity and Associated Risk Factors and Comorbid Conditions
A systematic approach where growth parameters, medical and psychological issues, and diet and activity habits are routinely assessed in all children is recommended (Figure 1). 3 No single measure clearly distinguishes health from disease, but routine assessment of the relation of height and weight is useful to create awareness and prompt further assessment and discussion. There is moderate evidence that routine body mass index (BMI) screening results in meaningful weight loss or improved outcomes.4,5 Electronic medical records automatically produce weight for length plots for children younger than 2 years 3 and BMI for children older than 2 years. 3 Physicians should routinely review these displays in addition to standard length and weight charts. Since BMI changes with age, percentiles specific for age and sex are used rather than absolute BMI. For children with a BMI above the 95th percentile, displays which stratify BMI as a percentage of the 95th percentile are also available. Class I obesity is defined as BMI greater or equal to 95th percentile but less than 120% of the 95th percentile. Class II obesity is BMI greater or equal to 120% to less than 140% of the 95th percentile. Class III obesity is defined as greater than 140% of the 95th percentile.6,7

Staged approach to treating children with obesity or overweight.
In addition to diet, physical activity, and genetic factors, there are a number of increasingly recognized early childhood risk factors for childhood obesity. Significant maternal weight gain during pregnancy can increase a child’s risk for obesity.8,9 There is evidence that increases in BMI percentile level or BMI trajectory in children during the first 3 years of life is predictive of obesity. 10 Infants can develop obesity due to being overfed (such as for comfort) and other feeding practices like bottle feeding in infancy. 11 Bottle feeding formula can contribute to obesity in children due to the way the formula is prepared, the nutrient composition, and how it is provided to infants. 12 In addition, social determinants of health, including adverse childhood experiences can increase the risk of adolescent obesity. 13 These early childhood risk factors can be mitigated by nutrition counseling and parent support groups 14 and home visiting 15 for expectant mothers or mothers of high-risk infants.
There is not complete consensus on optimal screening in children with obesity. 16 The United States Preventive Service Taskforce (USPSTF) and American Academy of Family Physicians (AAFP) recommends against screening for hyperlipidemia due to insufficient data and no prospective evidence 17 ; whereas the American Academy of Pediatrics (AAP) and National Heart, Lung and Blood Institute do advise a fasting lipid profile in children aged 2 to 11 years with BMI ≥95th percentile and adolescents ≥12 years with BMI ≥85th percentile. 18
Testing for type 2 diabetes is recommended by the Pediatric Endocrine Society; when children have BMI percentile ≥95th percentile, a family history in first- or second-degree relative, high-risk race or ethnicity, and maternal history of diabetes or gestational diabetes during pregnancy. 16 Children should be screened for diabetes by obtaining a fasting glucose or 2-hour plasma glucose test after age 10 years or at onset of puberty, whichever happens first. 19 Hemoglobin A1c alone is not as reliable in children to diagnose diabetes. 20
It is important to identify comorbidities in obese children that are developing or have already developed—psychological (bullying, self-esteem, depression), decreased mobility, orthopedic, dermatologic, elevated blood pressure, cardiovascular disease, elevated lipids, and type 2 diabetes. 21 When childhood obesity continues into adulthood, it is associated with cardiovascular disease and type 2 diabetes. 3
Supporting Children With Obesity and Their Caregivers While Mitigating Bias and Stigma
Primary care providers must routinely convey that they are willing and continually available to discuss weight-related concerns in a nonjudgmental way and ensure that they are viewed as trusted partners who are present and supportive for these families over the long term. Many primary care providers do not feel that they have adequate time, knowledge, or tools to address obesity.22,23 Additionally, primary care providers must be aware of biases toward persons with obesity and avoiding stigmatizing them. Although evolving societal norms may be making obesity and overweight status somewhat more acceptable, body weight discussions nonetheless provoke emotional reactions in most people and conversations about weight may have unintended consequences. 24
Society in general and primary care providers in particular are often highly biased toward people with obesity. 24 A study with obese children aged 9 to 11 years found implicit bias to be around 5%. 25 Rather than ignoring or denying bias, primary care providers must instead develop the self-awareness to recognize and manage it, realize that it may be unconscious, and guard against providing different or suboptimal care. 24 Bias often results in the stigmatizing belief that obesity is in the control of the individual and that this chronic illness is a personal choice. 24
Stigmatization of patients with obesity by primary care providers in turn may lead to psychological distress, exercise avoidance, reduced preventive visits, and overall avoidance of care. 24 Stigmatizing children or their parents is ineffective as motivation for change and is more likely to be counterproductive, often resulting in unhealthy dieting or eating behaviors, or even eating disorders. 5 Adults who have experienced stigma or bias often avoid or delay medical care, and children who are overweight or obese are more likely to receive routine care in an emergency department rather than a physician’s office compared with normal weight controls.5,26
There is evidence regarding the “people first” terminology is preferred by patients. Terms that convey the sense of a person with a condition, such as “your child is above their ideal body weight” or “let’s try to help your child achieve healthier weight” are preferred over terms such as “fat,” “obese,” “morbidly obese,” or “chubby,” which imply that the person is defined by their condition (Table 1). 27 However, no matter what terms are used, body weight discussions provoke emotional reactions in most people. Primary care providers should ask permission to discuss weight with families and also ask what terms they prefer to be used when discussing abnormal weight. 28

Based on survey of 1064 adults (60% female, mean age 45 years) in 2010.
“No weight-based term was perceived to be completely free of stigma or blame; body weight may not be a neutral subject for most people, and that regardless of the language used. . .there may be an emotional reaction.” 27
Focus on Behavior Change
Most physicians recognize that addressing the obesity epidemic will require broad public health and societal changes. Families need advice about proper nutrition and physical activity, not necessarily for the child to lose substantial weight but to promote optimal physical and mental health, as well as to temper effects of obesity and slow the rate of weight gain. Even relatively small amounts of weight loss of just a few pounds; have been shown to improve various metabolic and laboratory parameters. 29 Unfortunately, most individuals who lose weight regain it after 12 to 24 months, and it is not known if this temporary change is helpful or even harmful over a lifetime.
Motivational Interviewing
Physicians who utilize motivational interviewing techniques are more successful in helping patients change behaviors than those relying on a more direct approach. 30 Patients are often ambivalent about change and are more likely to be successful if they are able to consider and articulate their own reasons and goals for addressing behavior change and are asked nondirective questions like “What concerns, if any, do you have about your child’s weight?” 3 When approaching patients on their terms, the physician develops rapport and helps patients develop strategies to identify concerns and overcome barriers to healthier lifestyles. 31
Weight Loss Programs
There are freely available tools and resources that can help primary care providers promote behavior change including Choose My Plate, Let’s Move and Let’s Go 5-2-1-0.32,33 Let’s Go 5-2-1-0 recommends that children eat 5 or more fruits and vegetables, watch 2 hours or less of recreational screen time, participate in 1 hour or more of physical activity and ingest 0 sugary drinks each day. 34 This tool has been demonstrated to improve healthy habits35,36 In children with obesity, especially those with associated comorbid conditions and who do not respond to initial primary care interventions, referral to more intensive programs should be considered. Comprehensive, lifestyle-based behavioral interventions of approximately 26 or more total contact hours have been found effective for weight loss in children and adolescents after 6 to 12 months duration in program. 4 Typical interventions include multispecialty teams with physicians, physical therapists, dieticians, psychologists, and social workers.
Medications
In treating childhood obesity, medications should only be used as part of a comprehensive weight management program; they have only been studied in conjunction with supervised diet and exercise interventions and have no role as a stand-alone or first-line treatment. The Food and Drug Administration has approved Orlistat for children older than 12 years. Metformin is helpful in children with impaired glucose tolerance or polycystic ovary syndrome, and often promotes weight loss. This medicine can usually be used in children as young as 6 years. Unfortunately, any weight lost is usually regained after stopping the medication. The use of medication for childhood obesity is also limited by side effects, cost, and uncertainty about their long-term safety.3,37
Bariatric Surgery
Bariatric surgery is effective in selected adolescents with severe obesity who fit the criteria in Table 2 38 and was recently endorsed by a policy statement from the American Academy of Pediatrics. 39
Pediatric Bariatric Surgery Candidate Requirements. 38
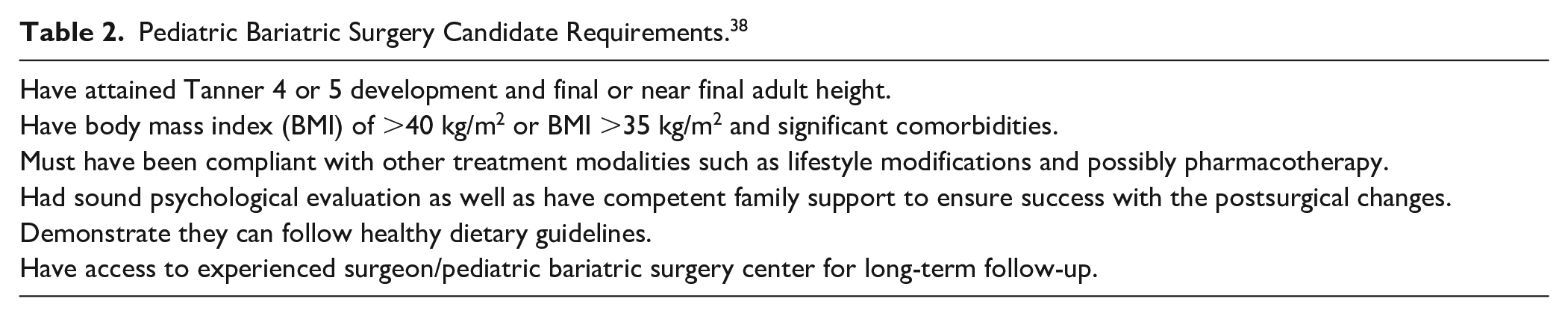
Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy both resulted in slightly more than 25% weight loss after 3 years. 40 Children treated with bariatric surgery also showed remission of type 2 diabetes, prediabetes, abnormal kidney function, elevated blood pressure, and dyslipidemia after 3 years. 40 Primary care providers should be aware of this new evidence of the efficacy of bariatric surgery for severe childhood obesity and refer appropriate candidates to appropriate pediatric tertiary care centers.
Limitations of This Work
This future practice guideline was limited by the fact that there are different recommendations from different professional societies on management of children with obesity. Primary care providers, though, need to understand these differences to inform them how to deliver family-centered care. Additionally, there is a paucity of knowledge currently regarding medical provider stigma and bias toward children with obesity and most of the recommendations in this practice guideline were extrapolated from adult studies. It is important that primary care providers recognize that stigma and bias can occur toward children with obesity and their families. Future research needs to investigate educational and practice-based approaches to mitigating stigma and bias in the care for children with obesity.
Conclusion
It is imperative that primary care providers provide a family-centered advice and support for children with obesity and their caregivers. The primary care provider is ideally suited, through long-term trusting relationships with families, to screen for obesity and associated risk factors and co-morbid conditions and to offer sensitive, respectful advice that mitigates the negative impact stigma and bias. Primary care providers should focus their childhood obesity intervention efforts on incremental, family-focused behavior changes which can mitigate or delay comorbidities or complications. Future childhood obesity research should evaluate the best methods for educating primary care providers in providing family-centered care and the optimal approaches to delivering this care.
Footnotes
Acknowledgements
The authors would like to thank Dr Tom D. Thacher, Mayo Clinic Department of Family Medicine Research Chair, for support of our work.
Author Contributions
Dr Tara K. Kaufman was first author who designed the work, performed the literature review, and was drafter of the manuscript. Dr Brian A. Lynch and Dr. John M. Wilkinson contributed equally to work on paper by critically reviewing literature and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.