
Abstract
Objectives:
Poor Food security (FS) is associated with risk of diet-related diseases and rising healthcare costs. Produce Prescription Interventions (PRx) are emerging clinical tools to improve FS and diet quality, but their impact in families with children is not well established. This study evaluates the impact of a pediatric PRx on FS and nutrition-related behaviors.
Methods:
Adult caregivers of children (0-18) were enrolled within a 6-month produce delivery and nutrition education intervention. A validated food security survey was administered pre/post intervention to determine FS scores and “Food Secure” status. Statistical analyses tested pre-post differences in FS scores and proportion of scores within the “Food Secure” range. Semi-structured interviews were performed post-intervention to explore families’ experiences with low FS and healthy behaviors and were thematically analyzed.
Results:
Between October 2021 and December 2022, 82 families were enrolled, 65 completed FS survey at baseline and 54 completed it at post-intervention. FS scores improved post-intervention (P < .05) and a greater proportion of household- and child-level scores fell within the “Food Secure” range post-intervention (P < .05). Twenty-eight interviews were analyzed. Three salient themes were identified: (1) value of healthcare-based screening and intervention, (2) food and education motivate behavior change, and (3) perceptions of post-intervention lifestyle sustainability.
Conclusions:
Participation in the PRx was associated with improvements in FS and nutrition-related attitudes and behaviors. PRx can be implemented by health systems to improve FS and health behaviors associated with risk for diet-related diseases. Longer-term support may be needed to maintain healthy behavior changes associated with PRx participation.
Keywords
Introduction
A diet high in fruits and vegetables (F&V) is correlated with lower disease burden 1 and lower healthcare costs in adults.2,3 However, <10% of the United States (US) consumes adequate F&Vs.4,5 Low food security (FS), or limited access to nutritionally adequate and safe foods, 6 poses a significant barrier to this optimal dietary pattern resulting, in lower quality diet,7 -9 increased risk of diet-related chronic diseases,10,11 and worse health, development, and educational outcomes in children.12,13 Factors contributing to the association between poor diet and low FS include the cost of and access to healthful foods compared to ultra processed food, taste preferences, and limited nutrition self-efficacy.14-16
In 2022, 17.3% of households with children experienced food insecurity, which was a significant increase from 2021 and 2020, likely reflecting an exacerbation of food insecurity resulting from the COVID-19 pandemic and associated inflation, economic challenges, and the end of pandemic era federal programs.17,18 “Food as Medicine” (FAM) interventions are a series of tools delivered in the healthcare setting to provide greater access to healthful food and nutrition education. Evidence suggests FAM interventions positively influence FS and dietary habits and reduce diet-related chronic disease in adults. 19 Pediatric-based FAM interventions include federal nutrition programs, medically tailored meals/groceries, and produce prescription interventions (PRx).19-22 Many PRx to date have focused on adults, 23 however, pediatric PRx may also improve household FS and produce intake in children. 24 Data regarding implementation of PRxs on households with children experiencing low FS is needed to understand their potential impact.
The Family Lifestyle Program’s Produce Prescription Initiative (FLiPRx) launched a pilot (FLiPRx 1.0) in 2020 to increase access to healthful foods and provide nutrition education for families with children. 25 Program evaluation was designed to understand the impact of a PRx on FS and perceived access to health food as well as healthy behaviors related to food purchasing and consumption. An updated version, FLiPRx 2.0, was launched in 2021 and incorporated lessons learned from the pilot and the theoretical framework established from that work. Table 1 describes FLiPRx 1.0 and 2.0. This theoretical framework establishes the link between FS and long-term health in 5 steps. First, low FS is associated with poor diet quality. Second, the healthcare setting is a critical venue to screen for and address FS. Third, PRx programs provide clinicians and families with a tool to address FS and diet quality. Fourth, enrollment in PRxs leads to experimentation and diet diversification. Finally, these dietary changes lead to improved longitudinal behavioral changes and chronic disease prevention. This paper describes the impact of FLiPRx 2.0 on household, adult, and child FS and subjective experiences around nutrition-related behavior change in families.
Program Design Differences between the Family Lifestyle Program’s Produce Prescription Initiative (FLiPRx) 1.0 Versus FLiPRx 2.0.

Methods
FLiPRx is delivered by a major academic medical center in collaboration with community organizations, including the Young Men’s Christian Association who helped co-create and deliver the monthly nutrition and culinary classes and 4P Foods, a local food hub working with local farmers to deliver the food,26,27 serving families living in historically and economically marginalized, majority African American neighborhoods within and adjacent to Wards 7 and 8 in Washington, DC. Residents in these neighborhoods experience disproportionately high rates of chronic disease, poverty, low FS, and lack adequate access to full-service grocery stores.18,28-30
From October 2021 to December 2022, pediatric patients (0-18 years old) and their adult caregivers who had poor FS via the Hunger Vital Sign™ screening questions 31 were recruited from 2 primary care clinics located in Ward 8. Detailed inclusion criteria have previously been described. 25 FLiPRx 1.0 participants were ineligible. Caregivers gave their written informed consent. This work was approved by the Children’s National Hospital Institutional Review Board (Pro00014391).
This family-based intervention has been described in detail elsewhere. 24 Briefly, home-delivery of 8-pounds of pre-selected F&Vs was provided every 2 weeks for 6 months along with virtual evidence-based nutrition education. The curriculum was guided by Social Cognitive Theory and the Transtheoretical Model. 32
This was a longitudinal interventional cohort study, using a convergent mixed-methods design through pre-post adult self-report surveys and post-intervention semi-structured interviews. Post-intervention surveys were conducted within 1 month of program completion. Primary quantitative outcomes were changes in household-, adult-, and child-level FS. Using thematic analysis, qualitative information explored post-intervention self-perceived food access and nutrition-related attitudes, knowledge, and behaviors. 33 Additionally, baseline demographics and programmatic outcomes were collected. Race and ethnicity information was classified based on participant self-identified data. While race and ethnicity are social constructs, participant self-identified race/ethnicity data were included in this study for 2 reasons. First, it is critical to acknowledge that the community within which the intervention took place is predominantly African American and historically disenfranchised.29,30 Second, both local and national studies have shown that Black families are disproportionately impacted by low FS, therefore highlighting the importance of developing FS interventions which address racial disparities.17,18
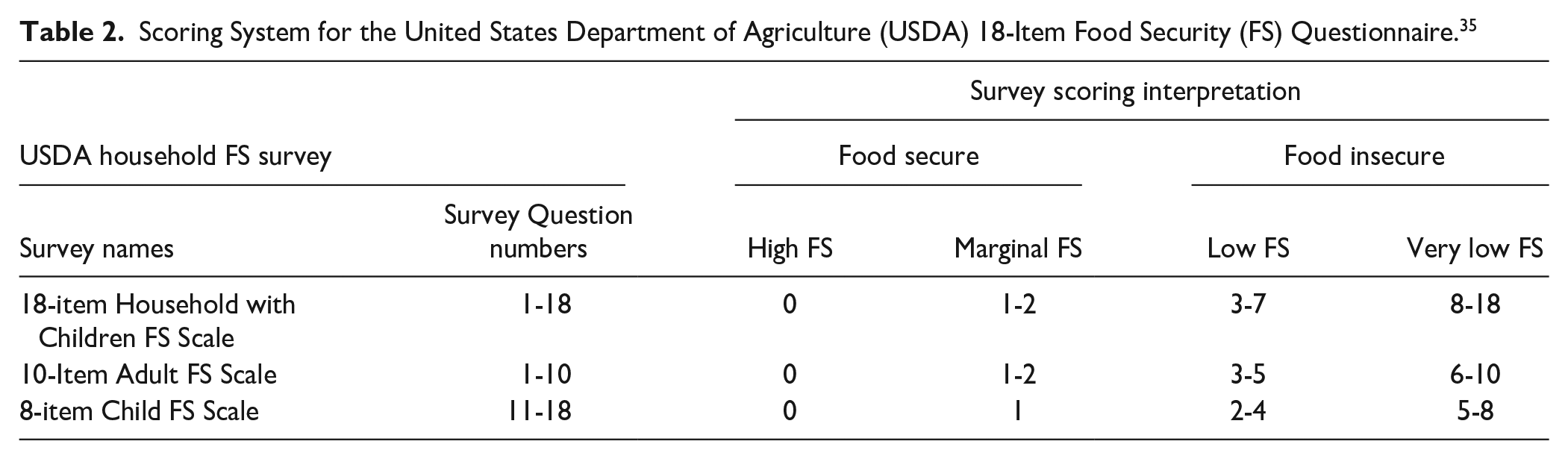
Survey data were obtained using Research Electronic Data Capture (REDCap). 34 FS was measured using the validated 18-item USDA Household Food Security Survey. 35 Initially, FS was measured through the 6-item FS questionnaire but the 18-item FS questionnaire was implemented several months into participant enrollment because we wanted to collect data at the level of the child. The quantitative analysis included in this manuscript is of the participants who completed the 18-item FS questionnaire to capture more detailed food security data for households with children. The sum of affirmative responses to questions (q), was used to calculate the degree of FS for the household (q1-18), adult (q1-10) and child (q11-18). FS scores were converted into corresponding FS categories “Food Secure” or “Food Insecure.” Table 2 summarizes the scoring system. 36 Rate of enrollment was the number of baseline surveys completed divided by the number of eligible referrals. Retention was the number of completed post-intervention surveys divided by the number of enrolled participants. Individual participant attendance was recorded at each class by program staff and the individual rate of attendance was the percent of classes attended. Utilization was self-reported by monthly surveys (on a scale of 0%-100%). Participants received monetary compensation for completing surveys and interviews. There were no specific study disenrollment criteria. The Strengthening the reporting of observational studies in epidemiology (STROBE, Supplemental checklist) cohort reporting guidelines were utilized to report the methods and findings of the study. 37
Scoring System for the United States Department of Agriculture (USDA) 18-Item Food Security (FS) Questionnaire. 35
Univariate analysis was used to describe baseline demographics, programmatic outcomes, and quantitative FS outcomes. The changes in the degree of FS were analyzed using the non-parametric Wilcoxon Signed Rank Tests because the data were not normally distributed. McNemar’s Test was used to evaluate the change in the proportion of “Food Secure” participants from baseline to post-intervention. Differences in demographics and FS scores in interviewees versus non-interviewees was explored through Wilcoxon Rank Sums Test. Significance level was set at p < .05. Statistical analysis was conducted with SAS software version 9.4. 38
All FLiPRx 2.0 participants who completed the program were invited to take part in a semi-structured interview with the aim to interview all participants until data saturation was reached. Interviews were then administered via Zoom within 2 months of program completion. Three team members were trained and conducted interviews. Two of the interviewers were known to the participants from their role in research coordination activities including the initial consent process, reminder phone calls and texts, and presence at monthly cooking classes for technical assistance. Interview questions were designed to elicit feedback on the program delivery and perceived impact of the program on access to healthy food and produce utilization. Interviews were recorded, transcribed, and analyzed using Dedoose Version 9.0.17. 39 Codes were developed, and preliminary themes were created using the content thematic analysis approach. 40 Four team members completed an initial reading of all transcripts and created a codebook. All of the research team members who conducted interviews also participated in the study analysis. Each transcript was coded independently by 2 coders. Thematic analysis of interviews concluded after reaching data saturation. After the data was fully coded, themes and subthemes were defined through an iterative group consensus process.
Results
Between October 2021 and December 2022, 82 child/adult pairs were enrolled on a rolling basis. Table 3 provides demographics of enrolled participants and the sub-group of interviewees (n = 28). Interviewees did not significantly differ from the non-interviewees in demographics or baseline FS. Rate of enrollment was 64.5% (82/127), retention was 65.8% (54/82). The average rate of individual attendance was 43.5% (±27.9%) and 51.2% attended ≥50% of monthly classes. Average monthly produce utilization was 72.3% (±18.5%).
Characteristics of Adult Caregiver Participants in FLiPRx 2.0.

DM, diabetes mellitus; HTN, hypertension; SD, standard deviation; SNAP, supplemental nutrition assistance program; SSI, social security income; TANF, temporary assistance to needy families; WIC, special supplemental program for women, infants, and children.
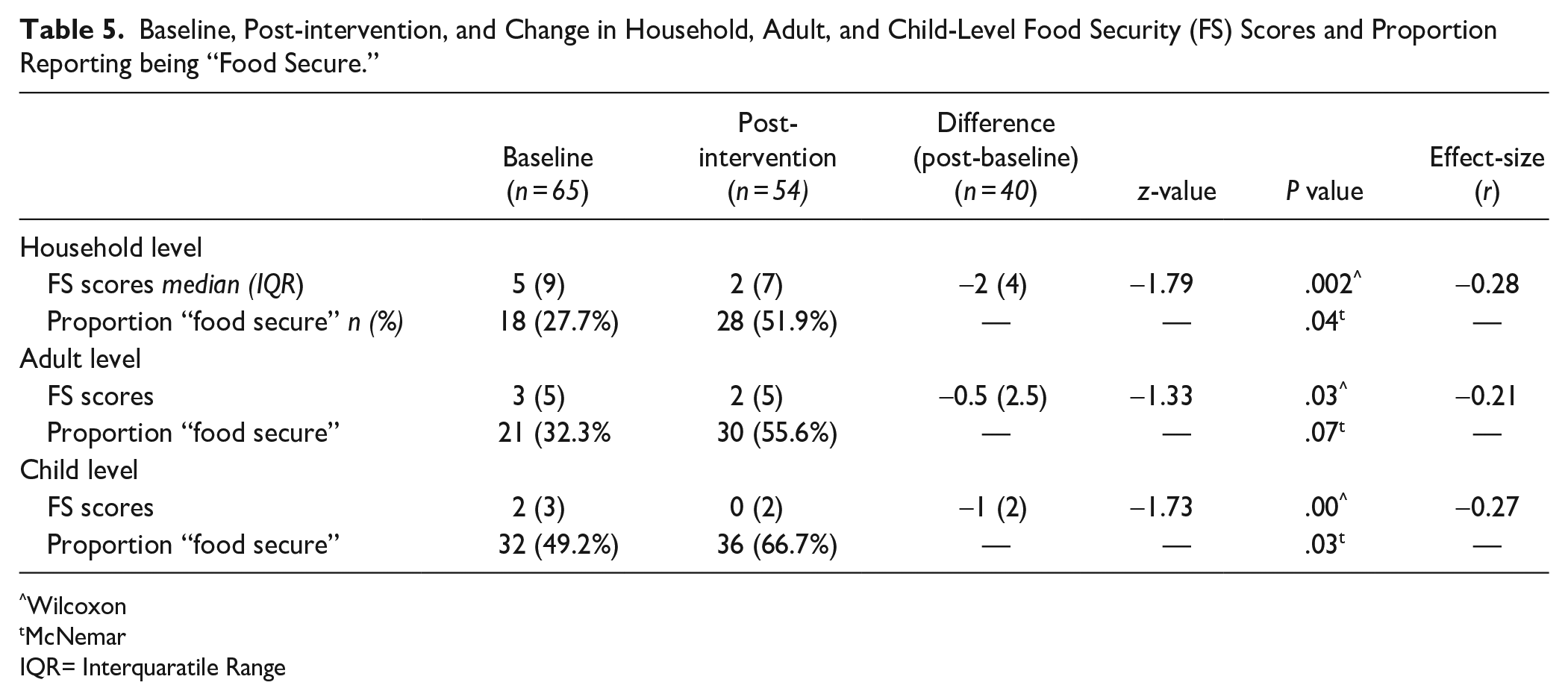
Sixty-five participants completed the 18-item FS questionnaire at baseline and 54 completed it post-intervention. Forty participants had complete pre-post FS data. The rate of affirmative responses to individual survey questions was generally lower post-intervention compared to baseline (Table 4). Median household FS scores were significantly lower (p = .002) at post-intervention (2.0) with interquartile range (IQR) of 7) versus baseline (5 IQR=9). The effect size (r=-0.28) indicates a near-medium effect. Median adult FS scores were significantly lower (p = .04) at post-intervention (2 IQR=5) versus baseline (3 IQR=5). The effect size (r=-0.27) indicates a near-medium effect. Median child FS scores were significantly lower (p = .001) at post-intervention (0 IQR=2) versus baseline (2 IQR=3). The effect size (r=-0.21) indicates a small effect. The median baseline household, adult, and child FS score were in the “Low” category and the median post-intervention scores was in the “High” category, indicating overall improvement in FS. (Table 5). The proportion of families who scored in the “Food Secure” range increased from baseline to post-intervention at the household, adult, and child levels (Table 5). This pre-post difference was statistically significant at the household (p = .04) and child (p = .03) levels.
Rates of Affirmative Answers to the USDA 18-item FS Questionnaire.

Baseline, Post-intervention, and Change in Household, Adult, and Child-Level Food Security (FS) Scores and Proportion Reporting being “Food Secure.”
Wilcoxon
McNemar
IQR= Interquaratile Range
From June 2022 to March 2023, 28 participants completed post-intervention interviews before saturation was reached. Table 6 summarizes themes, sub-themes, and representative quotes.
Results of the Thematic Analysis.

Theme #1: Value of Food Insecurity Screening and Intervention Within the Medical Home
Subtheme: 1.1 Referral from trusted healthcare provider to address health conditions
Caregivers often joined the program because they wanted to make lifestyle changes. They were concerned about their child’s health and risk of diet-related diseases and sought advice from healthcare providers who introduced them to FLiPRx during the clinic visit: “I was actually referred to the program because of my daughter. She’s on the overweight side, and we had to find ways for her to start eating without gaining [weight], and because she was at risk of diabetes.” Participant (P)132
Another participant mentioned: “At the time, I had a fifteen-year-old [son who] was kind of overweight. So I was looking for a way to get his weight under control.” (P70)
Subtheme 1.2: Tangible resource to address pressing health-related social need
Caregivers faced barriers to implementing lifestyle changes to self-identified and medically diagnosed health concerns on their own. Barriers included time constraints, transportation challenges, and limited local healthy food options: “Where I live, we don’t have that many grocery stores and the fruits and vegetables that you get are sometimes not good.” (P124)
Providing free home-delivered produce helped reduce financial and accessibility barriers: “My cars got messed up, so having it dropped off at my door was super convenient.” (P24) Another participant added “My youngest doesn’t get lunch at school so [the free produce] helps me take care of my boys.” (P55)
Theme #2: Produce Delivery and Concomitant Nutrition Education as Catalysts for Caregiver Driven Behavioral Changes in Children
Subtheme 2.1: Exposure to assorted produce influenced family eating habits
Participants reported that exposure to free produce led to their discovery of new foods and recipes and willingness to experiment with novel F&V: “There were some green tomatoes, and I never tried them and after trying one, that was really good, and we was excited about that.” (P136) [With the produce deliveries] we’ll try some different things a little bit more often. We tried a Japanese curry. . . a recipe that uses some of the vegetables that we had and that’s a new house favorite. (P132)
Caregivers reported that their children were excited to explore the F&V delivered and found ways to get their kids to consume F&Vs: “[When the delivery came] we open it up and go through describing what was there, and [it was enjoyable to] be able to put your hand on the actual items.” (P84)
Subtheme 2.2: Engaging and supportive nutritional education influenced family eating and purchasing habits
Caregivers reported that the nutrition education facilitated produce utilization: “I love the book that you guys sent with the produce where it showed what this is, and this is how you store this." (P132)
The group classes fostered a sense of peer-learning: “One lady [discussed] things that she would implement because of the cooking classes that helped [her son] and I would think, ‘well, maybe I can help [my son] in the same manner.” (P26)
Participants learned practical shopping and nutrition label reading skills that enabled more informed purchasing decisions: “[Before] my vegetables would go bad. . . [now] I buy weekly vegetables with a plan.” (P45) Another mentioned: “I’m reading labels more now. . .looking for high sodium and high sugar, and if it’s high, I don’t buy it.’” (P70)
Theme 3: Family Perceptions of Post-Intervention Lifestyle Sustainability
Subtheme 3.1. Barriers to ongoing family behavior changes post-intervention
Participants expressed low levels of confidence in sustaining healthy eating habits due to ongoing barriers that will persist once F&V deliveries conclude, including limited local access, financial constraints, and lack of time: “I just have to keep looking [for produce] . . .I just have to go outside of DC. Sometimes. . .to Maryland. . .which is hard to get a ride.” (P115)
Caregivers expressed the potential need to reduce produce and healthful food consumption: “I would love to have resources to continue to have access as I don’t qualify for SNAP benefits. This kind of leaves me in the lurch of going to unhealthier options because they are cheaper.” (P84)
Participants were concerned about the financial consequences of food waste: “I love to spend money on things that my family is going to use, but it hurts to spend money on things that just sit there.” (P113)
Some expressed their desire for the program to continue beyond 6 months: “The only thing that will help me probably is, if I can continue to get the [deliveries] because that really came in handy because. . . I’m able to get other stuff that are needed in the household.” (P94)
Subtheme 3.2. Facilitators for ongoing family behavior changes post-intervention
Despite these barriers, participants identified lessons from FLiPRx that would support maintenance of healthy habits, including changes in attitudes and enhanced culinary skills, nutrition knowledge, and shopping strategies.
Families were motivated to continue to purchase, prepare, and consume F&Vs as well independently learn more about nutrition and cooking: “I’m gonna continue to make some of the recipes that you all had. And I want to continue trying new and different types of vegetables and stuff when I go into the store.” (P94)
Caregivers expressed a newfound positive attitude toward produce consumption: “I want to definitely incorporate more vegetables. . . I want to make the change because if I can do it for myself it will help my kids. Eating fruits and vegetables makes me feel more alive.” (P39)
Some mentioned strategies to reduce cost while buying healthful foods: “I’m talking about teaming up with my mom [getting] the big bulkier foods, and we’ll just break it down and share.” (P24) Another mentioned: “Now, I’m like, ‘okay so there’s $2, do I want to get a bag of chips or do I want to get these two apples’. This bag of chips will last [my son] for two minutes. [But] with these two apples I can make two different desserts.” (P56)
Discussion
This study evaluated the impact of a 6-month PRx on FS and explored the lived experience of families. Post-intervention FS scores were significantly lower and a larger proportion of household- and child-level scores were categorized as “Food Secure” compared to baseline. These findings support the hypothesis that PRx participation improves FS. Qualitative data from post-program interviews provide context on factors that contributed to improvement in FS and describe barriers and facilitators to food access and healthy eating habits.
Similar FS improvements have been reported in other PRx studies.41-43 One study using the FS Survey Module for Youth identified a significant improvement in child-reported FS to a similar degree as our parent-reported results. 42 Other PRx studies measured FS using short form screeners without assessing severity of FI,44,45 and also reported improvements in FS. Our results expand on these studies by using the USDA 18-item FS questionnaire in a PRx and demonstrating that PRx participation is associated with significant improvement in FS at household and child levels.
We found a larger increase in child FS than adult or household FS. FLiPRx was designed to address pediatric health concerns, thus adult caregivers may have been motivated to address their childs’ food needs before their own. Previous research has also shown that adults often attempt to shield children from feeling the impact of low FS. 8 For example, of the 17.3% of households with children that were food insecure in 2022, only around half reported FI at the child-level. 17 Thus, improvement in child FS may be attributable to parents’ tendency to prioritize their children’s FS. This suggests that increasing produce delivery size could further improve FS at the household and adult level.
Our previous pilot study reported a statistically non-significant improvement in FS. 25 This difference may be from differences in data collection methods, participant engagement, intervention design, or other unmeasured factors. For example, FLiPRx 1.0 utilized the 6-item FS survey, was statistically underpowered, and had much lower nutrition education attendance compared to 2.0. 25 In 2.0, attendance and produce utilization were correlated (not reported), so further investigation of the relationship between program engagement, produce utilization, and FS is warranted. Additionally, FLiPRx 1.0 was a 12-month intervention while 2.0 was 6 months. While this change was made based on participant feedback that 1 year commitment was challenging, it may have also impacted the results of the FS outcomes. The positive results at 6 months suggest that FLiPRx 2.0 could potentially have made an even larger impact if extended to a year. Further research directly comparing FS status based on length of participation is needed to understand the impact of duration on FS outcomes.
Our reported utilization rate (73%) is comparable 46 or exceeds43,47 reported redemption rates. Most pediatric PRx currently offer vouchers and redemption rates vary widely, many below 70%. 48 Our qualitative data suggests delivery reduced transportation and access barriers, so home delivery may have advantages compared to vouchers and might be a more effective PRx implementation strategy in patient communities similar to this setting.
FLiPRx provided pre-selected produce, to which participants reported perceived improvements in the quality, quantity, and variety of produce available and consumed. Household produce availability is correlated with F&V consumption, 49 so increasing household availability of produce may increase F&V intake. Participants reported free produce alleviated concerns for potential financial loss from unused food. Research suggests fresh produce items are among the most wasted foods, 50 so offering families with limited resources free produce might mitigate their likelihood to limit buying produce due to the risk of financial loss.
Qualitative results suggest a healthcare-based referral encouraged participation in FLiPRx. Participants accepted the referral because it came from a trusted health professional and addressed their child’s diet-related disease risk and household FS. Existing literature supports that referrals from trusted healthcare providers increase participation in community programs, 51 families are interested in discussing diet-related health conditions with their child’s pediatrician 52 and prefer a multidisciplinary approach to dietary interventions. 53 There are also health related benefits to providing a social needs intervention within the primary care setting.54–56 This suggests an opportunity to leverage medical visits as a particularly important time to capitalize on motivation for healthy lifestyle change.
FLiPRx’s nutrition education helped participants utilize produce by providing practical knowledge around food preparation, storage, and nutrition literacy. Interacting with other families in virtual classes created a community to share and learn from. Thus, providing practical, group nutrition education may increase the variety and quantity of produce used by families. Other PRx have also reported positive qualitative outcomes of nutrition education.41,44,57 Nutrition education within other forms of FAM have yielded positive results in dietary quality. 58 Quantitative analysis on the impact of nutrition education in PRx on F&V intake is needed.
Participants raised concerns about navigating barriers to sustaining behavioral changes once the program concluded. Such concerns are a major theme in other PRx studies.25,45,59 In this study, families who completed the 6-month program were asked if they would like additional food resources and were provided information about resources specific to their neighborhood. The nature of entrenched social needs may necessitate embedding PRx within the structure of health systems serving marginalized communities. Medicaid managed care programs and private healthcare payers have begun pilot programs that offer PRx as part of their coverage.46,60 Data from these pilots will guide future decisions around payment for healthcare-embedded FAM interventions.
Based on participant feedback, potential improvements to PRx interventions include offering more than one live educational option per month to accommodate busy schedules, offering staple cooking ingredients and tools (spices and measuring cups) as an “onboarding kit” to facilitate use of the delivered produce and to follow along with class recipes, delivering an amount of produce proportional to family size, and incorporating self-select items in addition to pre-selected produce items.
This study has limitations. The 18-item FS questionnaire was not implemented until several months into participant enrollment. Therefore, the FS analysis only represents a portion of families who participated and were interviewed. Overall, 61% of participants had complete pre-post survey data which could have led to non-response bias. However, interviewees and non-interviewees did not differ in demographics or FS score, so our sample adequately represents the majority of participants. Post-intervention surveys and interviews were completed within 1 and 2 months following the completion of the study in order to help limit recall bias. Additionally, some of the interviewers were known to participants which may lead to social-desirability bias. Study surveys were intentionally self-administered to minimize social desirability but we do acknowledge that self-report tools also have a risk of recall bias. We had no control group and cannot determine causality. FS data were collected through parent self-report, which may be inaccurate as adults tend to overestimate FS experienced by their children.61-63 However, we used parental report for pre and post FS scores, so the change in scores is likely to accurately represent the longitudinal change in child FS scores. Possible changes to consider for evaluation of the program include having adolescent reported quantitative FS and F&V data and qualitative data, rather than just caretaker reported data. 64
Conclusion
This study investigated the impact of a pediatric PRx on FS and the family’s nutrition-related behaviors. Results showed that PRx participation improved FS and families perceived improvements in access to and consumption of healthy food. The F&V delivery and nutrition education were cited as key factors in these improvements. However, participants were concerned about sustaining lifestyle changes after program completion, highlighting the need for sustainable medical and policy solutions that address the deeply entrenched structural inequities that underlie FS. Future studies should explore the impact of PRxs on long-term healthy eating behavior change and reduction of diet-related disease risk.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319241276780 – Supplemental material for Impact of a Pediatric Produce Prescription Intervention on Food Security and Perceived Nutrition-Related Behaviors: A Mixed-Methods Study
Supplemental material, sj-pdf-1-jpc-10.1177_21501319241276780 for Impact of a Pediatric Produce Prescription Intervention on Food Security and Perceived Nutrition-Related Behaviors: A Mixed-Methods Study by Hemen Muleta, Laura Fischer, Qadira Ali, Shannon Menezes, Noah Kim, Emily Minkah-Premo and Kofi Essel in Journal of Primary Care & Community Health
Footnotes
Author Contributions
Dr. Hemen Muleta conducted and coded interviews, participated in thematic analysis of interviews, drafted the initial manuscript, critically reviewed, and revised the manuscript. Dr. Laura Fischer conceptualized and designed the study, conducted and coded interviews, participated in thematic analysis of interviews, designed and supervised quantitative data collection and statistical analyses, critically reviewed, and revised the manuscript for important intellectual content. Dr. Qadira Ali coordinated and supervised quantitative data collection, critically reviewed, and revised the manuscript for important intellectual content. Dr. Shannon Menzes conducted, transcribed, and coded interviews, participated in thematic analysis of interviews, drafted the initial manuscript, critically reviewed, and revised the manuscript. Noah Kim conducted and coded interviews, participated in thematic analysis of interviews, performed quantitative data collection, drafted the initial manuscript, critically reviewed, and revised the manuscript. Emily Minkah-Premo assisted with the quantitative statistical analyses, critically reviewed, and revised the manuscript. Dr. Kofi Essel conceptualized and designed the study, participated in thematic analysis of interviews, coordinated and supervised quantitative data collection, critically reviewed, and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by No Kid Hungry [AWD00003121]; Children’s Health Board [na], Capital One [AWD00003715], Morningstar [AWD00004246]; and the Vitamix Foundation [AWD00003856].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.