
Abstract
Keywords
Diabetes mellitus (DM) is recognized as a major global public health problem. Diabetes is one of the main contributors to ill health and premature mortality worldwide. 1 Diabetes accounts for a huge burden of morbidity and mortality through microvascular and macrovascular complications.2,3 The total number of people with DM is projected to rise from 171 million in 2000 to 366 million in 2030. The urban population in developing countries is projected to double between 2000 and 2030. 4 Several guidelines and diabetes management programs have been developed to improve the DM care in the community. Treatment and preventive care in persons with DM can slow the progression of end-stage complications and reduce the risk of cardiovascular and other diabetes-related diseases.
Diabetes care is shared care, and consequently a close cooperation between hospitals and general practice settings is essential. In the last decades, the focus of care for people with diabetes has shifted from hospital clinics to family practice, and family practice is supposed as the first-contact source of diabetes management. 5 There is considerable variation in diabetes care models internationally, with care anchored in primary care, in secondary care specialist centers, or in shared care systems involving both general practice and hospital-based care. 6 Census in the United States and the United Kingdom has shown the increasing role of generalists in diabetes care. 7
Diabetes mellitus has been described as a modern epidemic 4 that is emerging rapidly in developing countries. Previous research done in Qatar by Bener et al 8 found a high prevalence of DM in the Qatari population. Over the last century, there has been rapid socioeconomic development in many countries, resulting in a move from a traditional to a modern way of life. The state of Qatar is a rapidly developing country with a change that influenced the lifestyle of the people towards urbanization, particularly over the recent decades. Qatar has a well-established primary health care (PHC) system that provides comprehensive services to the entire population on equitable bases. The PHC system protects and promotes the health of the population through the 23 health centers that are distributed across the country with a referral system to hospitals for highly specialized care. It is predicted 2 that the prevalence of DM will increase rapidly owing to changes in the population with a higher proportion of elderly, increased body weight, decreased physical activity, improved life expectancy due to earlier detection of the disease, screening for complications, and progress in medical treatment.
Evaluation of health care is a complex but important issue, especially regarding chronic diseases, to ensure the best care possible for the patients and to preserve and increase quality and compliance within the caring centers. Audit of diabetes care is now becoming common in general practice. 9 In the Middle East region, no studies exist on the quality of diabetes care; the lack of resources and services may result in a lower quality of diabetes care. Hence, this study was undertaken to determine the outcome of diabetes care provided in 2 different types of medical care facilities: PHC and hospitals.
Materials and Methods
This is an observational cohort study that was conducted among the diabetic patients registered in diabetic clinics of PHC centers and hospitals of the Hamad Medical Corporation during the period 2005 to 2010. Diabetes care is organized in most of the PHC centers and the outpatient clinics of 2 hospitals. During the study period from January 2010 to August 2010, the study included the diabetic patients registered in these diabetic clinics. The complete details about the recruited patients were collected during the 8-month period. Of the 2134 registered with diagnosed diabetes, 1678 agreed and gave their consent to take part in this study, thus giving a response rate of 78.6%. There were 575 patients from hospitals and 1103 patients from different PHC centers (9 urban area and semi-urban area) who agreed to participate and gave verbal consent to take part in this study. Any patients with incomplete data in the medical records were excluded from the study. The study was approved by the Hamad Medical Corporation before commencing data collection.
The nurses at the diabetic clinic performed all measurements of the clinical parameters during patients’ visits to diabetic clinics, and their lab reports are available in the patient files. Face-to-face interviews were conducted with patients to complete the questionnaire with the sociodemographic variables and satisfaction score of the patients. Physical examinations including height, weight, and blood pressure were recorded. Their previous physical examination measurements were extracted from their patient files. Family physicians and research nurses reviewed the medical files and recorded all lab investigation measurements from their files at the time of audit as a baseline and the lab values a year before baseline measurements.
Questionnaire
We have developed a structured medical audit/evaluation questionnaire for audit measures consisting of questions relating to sociodemographic data, medical history and comorbid factors, lifestyle habits, lab investigations, and patient satisfaction. The first part included information about sociodemographic characteristics including age, sex, marital status, education level, occupation, height, weight, blood pressure, and parental consanguinity. The second section collected information about family history of DM, diabetes treatment, and complications after the onset of diabetes. Lifestyle habits like physical activity, smoking, dietary pattern, and hours of sleep were included in the third section. The fourth section included items about laboratory investigations such as blood glucose, glycated hemoglobin (HbA1C), HDL and LDL cholesterol levels, triglyceride, urea, creatinine, bilirubin, albumin, and so forth. The investigators have made the necessary corrections and modifications after considering the minor differences and discrepancies that have been found during the pilot study. Content validity, face validity, and reliability of the questionnaire were tested using 50 subjects. These tests demonstrated a high level of validity and high degree of repeatability (κ = 0.84). Family physicians and research nurses reviewed the medical files and recorded all lab investigation measurements from their files at the time of audit as a baseline and the lab values a year before baseline measurements.
Physical Examination and Measurements
Physical examination and measurements were performed by a trained nurse. Height was measured in centimeters using a height scale (SECA, Hamburg, Germany) while the subject was standing bare feet and with normal straight posture. Weight was measured in kilograms using a weight scale (SECA). Body mass index (BMI) was calculated as the ratio of weight (kilogram) to the square of height (meters). Obesity and overweight were classified according to World Health Organization (WHO) criteria. 3 A person was considered obese if the BMI value was ≥ 30 kg/m2 and overweight if BMI > 25 kg/m2 and < 30 kg/m2.
Hypertension was defined according to WHO standardized criteria as systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or using antihypertensive medication. 10 Two readings of the systolic and diastolic blood pressure were taken from the subject’s left arm while seated and his or her arm at heart level, using a standard zero mercury sphygmomanometer after at least 10 to 15 minutes of rest. Then, the mean of the 2 readings was obtained. Smoking habits were classified in terms of currently being smoker or nonsmoker. Patients were classified as physically active if they reported participating in walking or cycling for more than 30 min/d.
Laboratory Measurements
Subjects reporting a history of DM and currently taking oral medications for diabetes were considered to have DM. Diabetes mellitus was defined according to the WHO expert group 1 ; that is, fasting venous blood glucose concentration ≥ 7.0 mmol/L and/or 2-hour post– oral glucose tolerance test venous blood glucose concentration ≥ 11.1 mmol/L. In all subjects, fasting blood glucose was determined by glucose meter, and an oral glucose tolerance test was conducted only if blood sugar was < 7 mmol/L. Samples were processed within 30 minutes of collection, and the laboratory tests were measured. Glycated hemoglobin (HbA1c) was analyzed using a high-performance liquid chromatography method with a range >6.5% defined as “unsatisfactory” metabolic control. 11 Other biochemical values like total cholesterol, HDL cholesterol, LDL cholesterol, and triglyceride were defined according to the WHO criteria. The classification of total cholesterol, HDL cholesterol, LDL cholesterol, triglyceride, creatinine, potassium, bilirubin, uric acid, and so forth were collected from their medical records.
Statistical Analysis
Student’s t test was used to ascertain the significance of differences between mean values of 2 continuous variables and confirmed by nonparametric Mann-Whitney test. In addition, a paired t test was used to determine difference between baseline and year before regarding biochemistry parameters, and this was confirmed by the Wilcoxon test, which is a nonparametric test that compares 2 paired groups. Chi-square and Fisher exact tests were performed to test for differences in proportions of categorical variables between 2 or more groups. Pearson’s correlation coefficient was used to evaluate the strength of concordance between variables. The level P < .05 was considered as the cutoff value for significance.
Results
Table 1 shows the sociodemographic characteristics of the studied diabetic patients by place of treatment. On average, primary care patients (46.1 ± 15.1 years) were older than were hospital patients (44.5 ± 14.8 years; P = .03). The proportion of diagnosed diabetic patients in primary care was particularly high in the age group 46 to 60 years (48.1%), whereas most of the hospital patients were in the age group 31 to 45 years (34.6%; P < .001). There was a significant difference observed in terms of age group, gender, marital status, occupation, and consanguinity of the DM patients attending the 2 medical settings (P < .001).
Sociodemographic Characteristics of the Studied Diabetic Patients by Place of Treatment (N = 1678)

US $1 = 3.65 Qatar Riyals (QR).
Table 2 reveals the important characteristics of the studied diabetic patients by place of treatment. Proportionally less primary care patients were overweight (40.4%% vs 46.4%; P = 0 .018) or obese (24.5% vs 32.7%; P < .001) compared to hospital patients with a significant difference. Type 1 diabetes was less prevalent in primary care (14.3%) compared to hospital patients (15.5%). The majority of DM patients attending primary care (64.8%) were involved in physical activities than were patients attending hospitals (49.9%). Smoking behavior was less prevalent in primary care patients. A greater proportion in the hospital sample had tobacco use status (13.6%) compared to PHC (9.2%). Some of the complications were significantly lower in the primary care sample than in the hospital sample.
Important Characteristics of the Studied Diabetic Patients by Place of Treatment (N = 1678)

Table 3 presents the evaluation of diabetic care provided by place of treatment. The mean level of glycated HbA1c dropped to 8.32 in the baseline from 9.10 in the primary care sample, which was a significant change (−0.78; P < .001) in the primary care. In the hospital cohort, the change was very narrow (−0.3; P = .05). Similar to the HbA1c assessment, patients in PHC had a slightly lower mean fasting glucose level (8.74; P < .001) than did patients in hospitals (9.43; P = .05) at the time of audit, with a significant difference in both medical settings.
Evaluation of Diabetic Care Provided by PHC Center and Hospital

Data are means (±SD) unless otherwise indicated. CI, confidence interval; PHC, primary health care.
Table 4 shows the satisfaction score of the studied diabetic patients with diabetic care. Primary care DM patients had a better satisfaction score in most of the satisfaction domains, particularly with current treatment (3.9 ± 1.3), controlling blood sugars (4.1 ± 1.5), convenience for treatment (4.3 ± 1.3), flexibility in treatment (4.1 ± 1.5), understanding of DM (4.1 ± 1.4), recommending the treatment (3.9 ± 1.4), and satisfaction to continue the present form of treatment (4.1 ± 1.5).
Satisfaction Score of the Studied Diabetic Patients With Diabetic Care (N = 1678)

Data are means ± SD unless otherwise indicated.
Figure 1 compares the patient outcome in diabetic care provided by PHC. There was a remarkable increase in proportion of DM patients with normal range of fasting blood glucose (25.3%-31%) in primary care, as compared to the fasting blood glucose measurement 1 year before.

Comparison of the patient outcome in diabetic care provided by primary health care centers. FBG, Fasting Blood Glucose
Figure 2 compares the patient outcome in diabetic care provided by hospitals. The proportion of DM patients with normal range of FBG increased slightly from 31.5% to 34.6%.
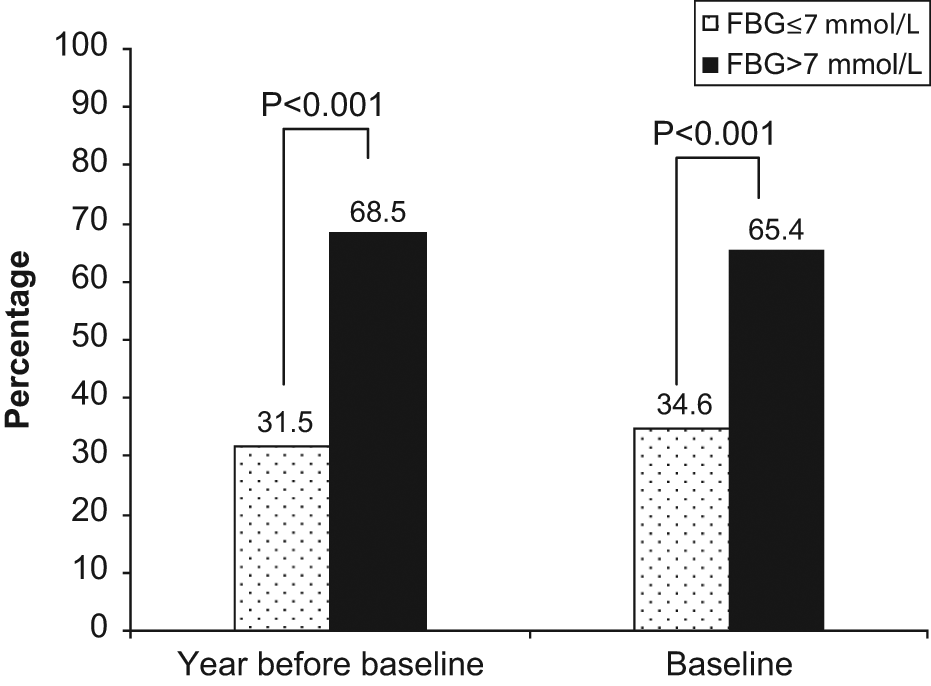
Comparison of the patient outcome in diabetic care provided by hospitals. FBG, Fasting Blood Glucose
Discussion
Diabetes mellitus is a major public health problem, causing significant morbidity and mortality.2-4 The present study is the first to compare results on diabetes care and its outcome for patients in primary care and hospitals. In this study, data outcomes of DM patients were analyzed according to 2 types of medical care facilities: primary care settings and hospitals. Evaluating diabetic care in both study settings showed conflicting results. In the PHC setting, the diabetic management improved blood glucose, HbA1c, total cholesterol, LDL, albumin, bilirubin, and triglyceride with a significant difference. In the hospital setting, there was no significant effect on these physiological parameters. Overall, the medical audit highlighted that primary care provides better diabetes care to patients than do hospitals. The study sample revealed that PHC had a considerable increase in DM patients with normal range of fasting blood glucose at the time of audit compared to the measurement 1 year before (25.3%-31%). There was even an improvement in the complicated cases (>7.0 mmol/L) during the last 1-year treatment (from 74.7% to 69%). This improvement in diabetes care shows that primary care gatekeepers can effectively reduce referrals to specialist care. These results are in accordance with another study 12 that showed general practice achieved standards of diabetic care as good as or better than that of hospital outpatient care. In diabetes care, knowledge about what is achievable in primary and secondary care is important.
In the study sample, the proportion of type 2 DM was higher in primary care (85.7%) compared to hospitals (84.5%), whereas type 1 DM was higher in hospitals (15.5%) than in primary care (14.3%). A similar result 13 was observed in a study done with a sample of 1678 patients in which 86% had type 2 DM and 13% type 1 DM. The high prevalence of type 2 diabetes represents a huge burden of disease that needs to be tackled at all levels, ranging from improvements in public health education and individual self-care skills education to improvements in PHC and tertiary care facilities.
Diabetic management in primary care was able to achieve significant change in clinical indicators. Also, metabolic control was good in PHC. A recent study 14 found a steady increase in the prevalence of metabolic syndrome through the decade. There was a good significant difference (−0.78; P < .001) in the mean value of glycemic HbA1C at the baseline (9.10% to 8.32%) in primary care patients compared to hospital patients (−0.2). These results show that the diabetes care process improved in PHC, with an accompanying improvement in HbA1C. Similar study findings were observed in 2 studies done by Campbell et al 15 and Saddine et al. 16 Although it appeared that DM patients attending PHC had better blood glucose and glycemic control than did patients attending hospitals, the majority of patients in both groups had fasting blood glucose level above normal range (>7 mmol/L) at the time of audit (69% vs 65.4%). It was reported in a study 17 that in some developed countries, at least half of those diagnosed with DM do not achieve satisfactory glycemic control. These study findings highlight the importance of implementing a wide range of interventions aimed at improving the provision of DM care and achieving better metabolic control for patients with DM in PHC.
A majority of the diabetic patients seeking treatment at PHC (48.1%) were in the age group 46 to 60 years, whereas most of the hospital patients were in the age group 31 to 45 years (34.6%). Hospital patients had a shorter duration of diagnosed DM than did primary care patients (6.7 vs 7.6 years). In this study, primary care patients were less overweight (40.4%) and obese (24.5%) compared to hospital patients (46.4% and 32.7%, respectively). This could be owing to the fact that primary care patients were more involved with physical activity (64.8%) than were hospital patients (49.9%). On the contrary, another study revealed that diabetic patients seeking treatment at primary care were slightly more overweight (49%) compared to patients in hospitals (42%). 18 More than studied hospital patients (34.1%), the primary care patients developed diabetes in their middle age, older than 45 years (48.1%), and they should be treated more aggressively to avoid diabetic complications in the future because it occurred in their middle age.
It is worth noting that most of the complications were lower in primary care diabetic patients than in hospital patients, except for blood pressure, neuropathy, and infertility. In both medical settings, although the DM patients have achieved adequate blood pressure control, hypoglycemia (20.7% vs 24.2%) and blood pressure (23.8% vs 17.9%) were the 2 leading complications in primary care and hospital patients. The complications found in this study are similar to the results of a previous study of Qatar19,20 that obesity, blood pressure, total cholesterol, HDL cholesterol, and triglyceride levels were higher in diabetic patients compared to nondiabetics. Basit et al 21 reported concurrent hypertension, obesity, and hypertriglyceridemia in a majority of patients having diabetes. Another study 22 revealed that strict controls of blood glucose, blood pressure, and cholesterol can reduce the risk of diabetes-related complications. However, the better control of diabetes could significantly reduce the development of these complications in PHC.
Although the overall quality of diabetes care in primary and tertiary care was different, it was very interesting to note that primary care patients were more satisfied with their treatment than were patients in hospitals in most of the satisfaction areas. This supports the current results that PHC provides a better quality of care to diabetic patients compared to hospitals.
Goudswaard et al 23 and Guldberg et al 24 reported that monitoring and careful recording of important clinical data are considered to be vital parts of diabetes care. This is true, and this study made it possible to compare past and present status to review the diabetes management in both medical settings. This addressed the issue of understanding the best way to narrow the gap between what is known to be effective in DM care and the care that is currently provided. This study proves that for the majority of patients with diabetes, particularly those with type 2 DM, it is possible to deliver care in the primary care setting that is at least as good as that provided in tertiary care hospitals. This study serves as a baseline for the assessment of ongoing interventions aimed at improving the quality of diabetes care in primary care and tertiary care settings.
Conclusion
The present study revealed that there was a remarkable increase in proportion of diabetic patients with normal range of fasting blood glucose at the time of audit in primary care compared to hospital diabetic patients. This improvement in diabetes care shows that primary care achieved better diabetic care than did hospitals. Even the satisfaction score was higher in patients attending primary care in most of the satisfaction domains, especially with current treatment, convenience of treatment, understanding of diabetes, recommending the treatment to someone, and continuing the present form of treatment.
Footnotes
Acknowledgements
This work was generously supported and funded by the Qatar Foundation grant No. UREP 07-099-3-023. The author thanks the Hamad Medical Corporation (HMC RP# 10067/10) for their support and ethical approval.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.