
Abstract
Introduction
Many different types of digital innovations for health and medical care (eg, Capio Go, Mindoktor, and KRY) have been developed in Sweden under the concept of eHealth. Based on primary healthcare conditions in Sweden, it is estimated that the implementation of various digital tools could achieve costs savings, if they allowed 1 in 10 primary care visits to be conducted over the Internet instead of a physiological meeting. 1
There is currently intense controversy within both the health and medical care services about the ongoing development of different eHealth solutions. Health care providers raise questions about eHealth both from a cost and resource perspective. Private companies are currently allowed to use increasingly aggressive marketing for providing “quick solutions” for a patient group that generally has the lowest need for medical contact. It is also of concern that this type of care is paid for with limited tax resources, and does not follow the health and medical care rules regarding prioritization of care for persons with the greatest needs. 2 It has thus been suggested that a first triage level should be used rather than allowing patients to voluntarily apply for care. 3
Notable benefits of eHealth are that it likely facilitates increased availability and time-efficiency for the patients. However, the impacts of eHealth from the stakeholders’ perspectives are less clear. Such interventions could be described as a complement to traditional primary health care but may also challenge the role that health professionals will play in the future. At the same time, it is clear that different patient groups require different types of care, and that the needed care cannot be delivered in a standardized manner. The employees’ interest is of great importance in determining the success of different new digital interventions and technologies—for example, whether an organization’s performance will be improved. 4 Mapping out employees’ views can help in achieving an increased understanding of the various perspectives and their level of influence.
Region Skåne in southern Sweden has completed a pilot project—the Digital Doctor Reception (DDR)—which involved digital written patient dialogues, and the use of the Nurse Telephone Counseling Service as a first “gatekeeper” to triage according to a specific diagnostic list. That tested protocol could be a first step toward a different way of using eHealth. Since this development also affects the Nurse Telephone Counseling Service, in the present study, we aimed to elucidate the nurses’ experiences with this innovative concept.
Methods
This study had a descriptive design, and was conducted with a partly qualitative inductive approach, to obtain greater insight into nurses’ experience of possible benefits and weaknesses in triaging primary care patients in an eHealth context. The first part of the study was a quantitative questionnaire survey with fixed response options. The second qualitative part comprised 2 open questions that asked the informants to write down their experiences and/or perceptions of the DDR concept in their own words.
The Digital Doctor Reception Concept
The DDR concept began when a patient called Nurse Telephone Counseling Services (1177 Vårdguiden på Telefon 5 ) or the primary care service about a health condition, and the nurses identified the patient as eligible. The patient was then informed about the available DDR. If the patient agreed to utilize the digital technology, the patient received a log-in code to access a referenced website. The patient inclusion criteria were age >18 years, having a diagnosis listed in Appendix A, speaking Swedish, and being assessed by a nurse as able to participate in the study. Excluded patients were those with diagnoses not meeting the inclusion criteria, evaluated by the nurses as having anxiety and/or stress that prevented participation, evaluated as being unable to take in information about the study, or not having access to the application Bank.ID.
For the present study, the included informants were nurses who were educated in the DDR concept, and who had identified eligible patients as well as triaged patients to the website. A total of 21 informants were identified, of whom 16 (76%) responded to our questionnaire.
Data Collection
Data were collected using a web-based electronic questionnaire that was modified by the authors. 6 All informants received an email containing a web-link to the active questionnaire. On connecting to the web-link, the informants reached the web server where the questionnaire (Appendix B) was available. After completing the questionnaire, the informants submitted their responses. Detailed information about the study aim and background was provided before the questionnaire.
The questionnaire with fixed options contained 4 demographic questions, and 8 thematically constructed questions covering the experiences and perceptions of the following themes: collaboration and challenge, technical functionalities, and DDR as an activity (Appendix B). There were also 2 open questions asking the informants to write down their positive and negative experiences and/or perceptions of the DDR concept in their own words. The informants were given unlimited space for their written responses.
Analysis
For statistical analysis of the quantitative data, the collected variables were analyzed using the statistical software SPSS version 24.0 (IBM Corp, Armonk, NY). These data are described with absolute values and relative frequencies (n, %), when appropriate. Then, the relative frequencies were dichotomized to evaluate the rates of positive responses to the concept, based on a 5-degree index-scale. Our aim was to objectively achieve overall comprehension in three domains: collaboration and challenge, technical functionality, and DDR as an activity. The index value (IV) summarized the percentages, strengths, and appellations as follows (inspired by Altman 7 ): <0.20 = None or very bad experience; 0.21-0.40 = Bad experience; 0.41-0.60 = Fairly good experience; 0.61-0.80 = Good experience; and 0.81-1.00 = Very good experience. These IVs are described as question index values (Q-IVs) and domain index values (D-IVs), as appropriate. Finally, question 8, Overall satisfaction with the concept, was described with a median (Md) and interquartile range (IQR) value.
The qualitative data were analyzed using conventional content analysis inspired by Hsieh and Shannon. 7 These data comprised short textual elements, which were read through to identify meaning units related to the study’s aim. Then these units of text were condensed and coded by the investigative team. Thereafter, the codes were grouped into subcategories and categories.
Results
This survey included 16 informants (response rate, 76%), including 94% women and 6% men, with a mean age of 52 years (SD, ±17). They had worked in their profession as nurses for a mean of 30 years (SD, ±13), and had triaged patients in the Nurse Telephone Counseling Service for a mean of 11 years (SD, ±11). On a 10-point Likert-type scale (1 = Not at all satisfied; 10 = Completely satisfied), Overall satisfaction with the DDR concept was described with an Md of 6.5 (IQR, 6-9).
Collaboration and Challenge
Table 1 presents the overall relative answers to questions in the domain Collaboration and challenge. The responses yielded a domain index (D-IV) of 0.66 (Table 2), reflecting a Fairly good experience. These results indicated that the concept provided the same ability to consult, support, and/or coordinate health resources (Q1). However, the informants felt the service was less challenging compared with normal working methods (Q2).
Summary Frequencies of Answer Options and Question Index Values (Q-IV). a
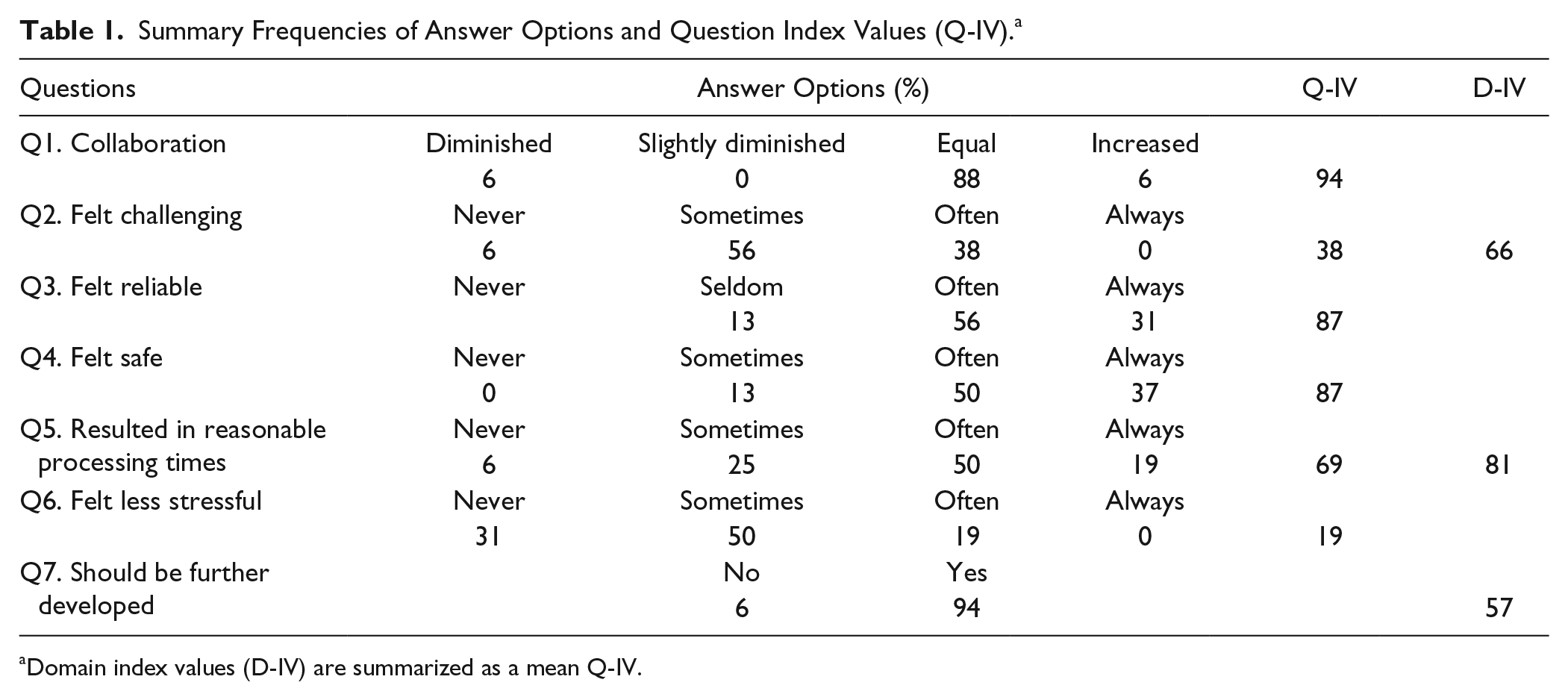
Domain index values (D-IV) are summarized as a mean Q-IV.
Present Domain Index Values (D-IV) Summarize the Percentages, Strengths, and Experience Appellations. a
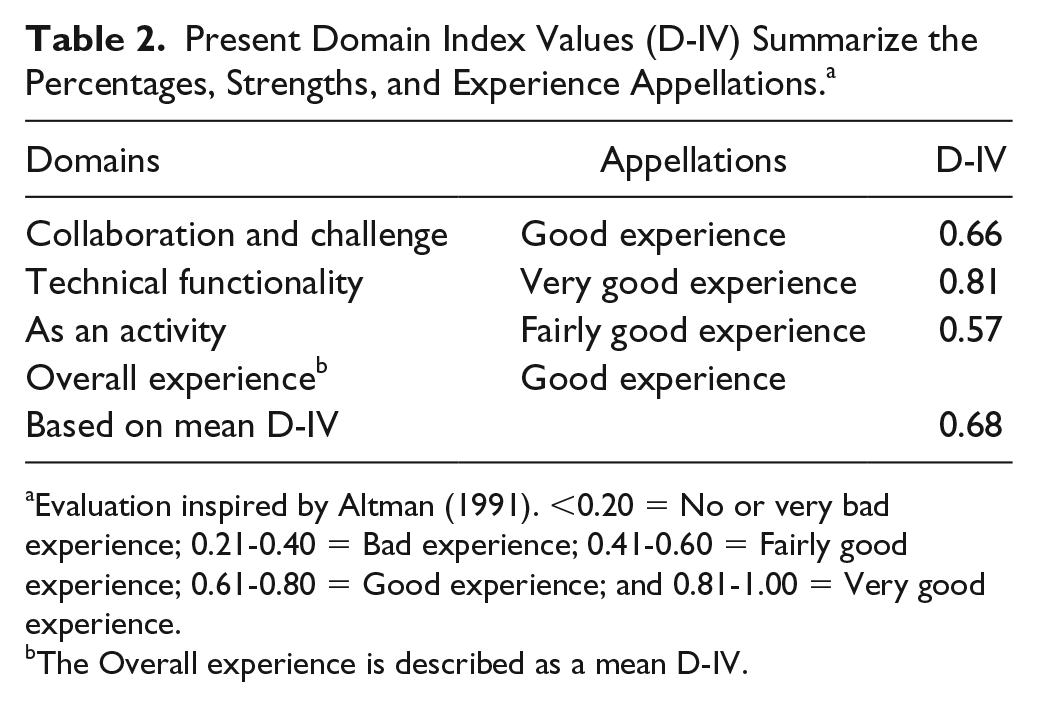
Evaluation inspired by Altman (1991). <0.20 = No or very bad experience; 0.21-0.40 = Bad experience; 0.41-0.60 = Fairly good experience; 0.61-0.80 = Good experience; and 0.81-1.00 = Very good experience.
The Overall experience is described as a mean D-IV.
Technical Functionality
With regard to technical functionality, the informants described their experience as Very good, with a D-IV of 0.81 (Table 2). The nurses felt the technical design was highly reliable (Q3) and the IT [information technology] was safe (Q4) to use, and they expressed that the technology entailed reasonable processing times (Q4; Table 1).
Experience of DDR as an Activity
This domain showed trends of varying experiences, with a mean D-IV of 0.57 (Table 2). The nurses expressed that the concept sometimes felt stressful (Q6) but thought that it warranted further development (Q7; Table 1).
Table 2 presents the nurses Overall experiences, summarized as percentages, strengths, and appellations. In the conventional content analyses of 48 statements, we identified three categories with underlying subcategories, describing the nurses’ views of the DDR concept using digital written patient dialogues (Table 3).
Summary of Codes, Subcategories, Categories, and Categories With Regard to Experiences. a

Abbreviations: DDR, Digital Doctor Reception; IT, information technology.
Each subcategory is labeled with the associated numbers of statements.
Facilitators in Using DDR Experienced by Nurses
The informants felt positive about participating in the development of an eHealth service and felt confident in the knowledge that an experienced general practitioner (GP) would further treat the patients. The nurses’ expressed overall positive views of triaging patients to the DDR concept, and generally thought that the concept should be further developed. However, the nurses also expressed that the concept should be based at a health care center to provide close proximity to the patients’ resident, answering “yes” when asked if the service should be broadened.
The nurses observed increased patient satisfaction when using the DDR, as the nurses were able to quickly and easily assign the patients. The nurses described that some patients expressed relief when they were not required to physically visit a health care center. They perceived that the patients felt positively about the assurance that they would be in contact with a GP within an assigned time frame, stating that “The ability to assign patients direct to the GPs meant that the patients were pleasantly surprised.”
Barriers in Using DDR Experienced by Nurses
Some nurses stated that some of the symptoms in the predetermined symptom list could have been handled through the nurses’ self-care advice, such that a GP contact was perceived as unnecessary. The nurses also reported that certain patient groups were excluded from the possibility of a digital care meeting, such as older patients with insufficient computer skills, and citizens who had not mastered the Swedish language. It was written that “Many older people are unable to carry out the various steps to complete a medical history, including the cause of contact, background diseases, and current inconvenience.”
The new approach of triaging was perceived by some nurses as time-consuming, involving increased program management, increased information content, and an increased time aspect when transmitting various messages and links. Occasionally, the nurses experienced some problems when IT errors occurred, stating that “The system was sometimes a bit cumbersome and difficult to handle,” and the nurses sometimes feared that the patients could be affected.
Discussion
Overall, the informants in our study expressed their satisfaction and described good experiences with the DDR concept, despite the changes from their traditional working methods as a telephone counseling nurse. Some informants described positive feelings about participating in the development of a new eHealth concept, and it seemed that the organization had succeeded in many aspects when designing the DDR concept. This was an important finding, since it has previously been reported that the development of different working methods can only be successful if the employees are well prepared and have the necessary prerequisites. 8
The respondents in our study reported fairly good experiences with collaboration (with colleagues) and challenges (in their profession) under the DDR concept. Possible negative aspects may have been due to an increased program management workload, which was experienced as time-consuming. Our results were based on an early minor pilot study; thus, the presented views may be related to too short a time frame, such that the nurses did not have sufficient time to get familiar with the concept. It has also been suggested that different job demands, resources, and emotional labor can affect nurses’ satisfaction in their profession. 9 When the triage nurses acted as first gatekeepers, a substantial part of their normal work was removed—notably, giving advice and support in case of suspected illness. Instead, if the nurses verified an initial diagnosis that was on the predefined symptom list, they would directly refer the patient to the chat function with the GP. This was likely a major reason that the informants felt the concept was sometimes less challenging compared to the nurses’ normal working methods. However, some informants still felt confident in the concept since the situation would be processed by an experienced GP.
The nurses felt that the technical functionality was good in terms of being reliable and safe to use, and they expressed that the technology entailed reasonable technical processing times despite minor technical errors. We believe that the nurses were not only aware of normal IT security aspects but were also accustomed to using IT tools and thus inclined to trust different IT systems in health care.
The development of new IT systems in health care opens a wide range of new communication opportunities, which should greatly contribute to improved avenues for patient treatment, communication, and care. However, the development of digital communication methods is also associated with several challenges and consequences, complicating the implementation of new concepts. When introducing innovations and new technologies, considerations must include the nature of the evidence or the innovation to be implemented; the context in which the changes occur; the communication patterns and support for change within the organization; and the professionals’ experiences, perceptions, and preferences. 10 Our present respondents described their experiences of the DDR as an activity as partly positive. The nurses felt that the concept was sometimes stressful but thought that it should be further developed. Our results suggest that participating nurses are curious about digital primary care, but also skeptical of some changes regarding their working methods. Moreover, some nurses expressed moral responsibilities for patients who could not be offered digitally solutions, including older patients with insufficient computer skills, and citizens who had not mastered the native language. Therefore, our concept should probably be considered as a complement to the traditional Nurse Telephone Counseling Service. 11
In the present study, we aimed to elucidate strengths and weaknesses, and to initiate further discussions that could contribute to digital care development—which is one future eHealth goal, according to the Swedish Government’s “Vision of eHealth 2025.” 12 No clear conclusions can be drawn from our survey. However, the results represent the first step in understanding the use of telephone counseling nurses as a first gatekeeper, and the conditions under which these nurses could work. It is important to integrate the professionals’ experiences and perceptions, especially considering the possible controversy surrounding patients’ ability to voluntarily apply for care, and what should be considered best care based on the organizations’ aptitude.
Strength and Weaknesses
In web-based surveys, the response rate is normally influenced by whether the respondents are accustomed to using computers and internet-based layouts. Since our respondents were in the habit of performing computer work in their daily lives, our method of data collection was not a weakness, as is supported by our high response rate.
A disadvantage of questionnaire surveys is that the respondents cannot convey in-depth developing responses. To obtain a more nuanced picture of the concept, we chose to include 2 open questions. We believe that our study design provided an improved depiction of this new digital concept from the perspective of the included nurses. Nevertheless, a traditional qualitative interview technique would probably further deepen the knowledge of the nurses’ experiences and perceptions of the described digital concept.
Conclusions
The results of this study suggested that telephone counseling nurses can be used as a first “gatekeeper” in a digital primary health care concept. The informants in our study expressed satisfaction and described good experiences with the DDR concept. Moreover, they felt that the concept was reliable, the IT was safe to use, and the concept entailed the ability to support and coordinate health resources. However, the informants felt that the concept was sometimes more stressful and less challenging compared to normal working methods.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.