
Abstract
Introduction
Diabetes has been declared as one of the largest global health emergencies of the 21st century. 1 Statistics show that diabetes is ranked amongst the top 10 major causes of death globally—approximately 80% of all premature non-communicable disease (NCD) deaths are attributable to diabetes. 2 At present, a total of 424.9 million people are afflicted by diabetes worldwide and these trends are projected to steadily increase to 628.6 million by the year 2045. 1 The annual financial burden incurred on the world economy as a result of diabetes is at a staggering USD 727 billion, which translates to 1 for every USD 8 spent on health care. 1
Type 2 diabetes (T2D) is largely preventable and accounts for 90% of all cases of diabetes. 1 As a sizeable number of risk factors linked to T2D are potentially modifiable, the cornerstone of T2D treatment are often self-management behavior such as the adherence to a healthy diet, increased physical activity and the maintenance of an ideal body weight. 1 The sustenance of these self-management practices give rise to favorable health outcomes in T2D patients, which are primarily reflected by better glycemic stability.3,4 However, self-management behavior demands changes to be made to deeply ingrained habits that permeate the daily life of an individual (Figure 1). Therefore, these strategies remain a major stumbling block to most people with T2D—the maintenance of behavioral changes pertaining to these interventions require long-standing commitment to optimal self-management practices.5-8
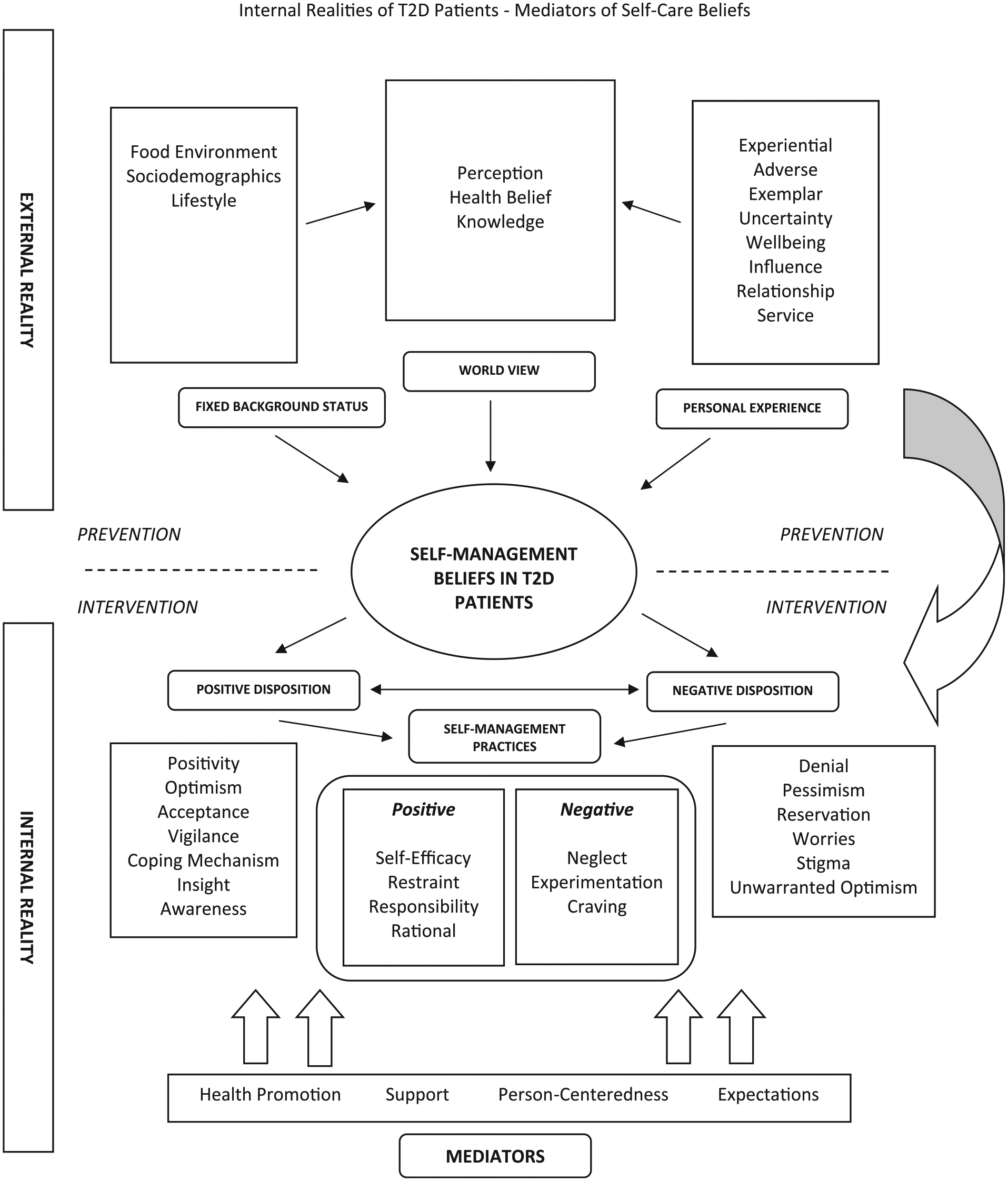
Conceptual framework describing the external reality, internal reality and mediators related to self-management of type 2 diabetes (T2D).
The paucity of robust scientific literature related to the assessment of self-management practices in T2D patients in Malaysia impedes steps to mitigate perceptible lapses seen in day to day clinical practice. For the most part, research effort within the field of self-care behavior have been geared toward a solely “niche area” qualitative exploration of this problem area.9-12 The emphasis of such qualitative inquiry appear to be fragmentary and primarily focuses on the investigation related to blood glucose self-monitoring, barriers to optimal diabetes control and “experimentation” in the selection of medications.9-12 Therefore, there is an absence of a holistic approach toward uncovering the naturalistic behavioral dimensions witnessed in the archetypal T2D patients in relation to their self-management practices.
We employed a grounded theory approach to our qualitative exploration in order to facilitate theory-building efforts relevant to the essential mediators of self-management practices that have direct influence on the internal psychological milieu of T2D participants. 13 Procedurally, this strategy involves the systematic collection and interpretation of qualitative information resembling any other inferential study design. Unique coding techniques (from example, the utilization of gerunds to connote action in the data) are utilized to iteratively unearth novel hypotheses arising from emergent themes obtained from the qualitative data. 13 Finally, these new concepts are incorporated into a behavioral model that might help explain the lived experience of the participant with regard to the area of scientific exploration.
The purpose of this study was to (1) determine the inherent expectations of T2D patients that can help support self-management practices, (2) expound and classify the beliefs surrounding their psychosocial support, and (3) create a functional model by exploring the interactions between these variables. This strategy that underpin the qualitative exploration of this study can be found in a research protocol that was published separately. 14
Methods
A grounded theory approach was adopted to elucidate detailed behavioral patterns pertinent to the objectives of this study. Thus, we conducted an inductive qualitative inquiry to (1) discover the mediators of the self-care practices, (2) iteratively interpret and amend inferences based on emergent data, and (3) use theory-building techniques to help uncover novel insights other than those already documented in literature. 13
Participants and Setting
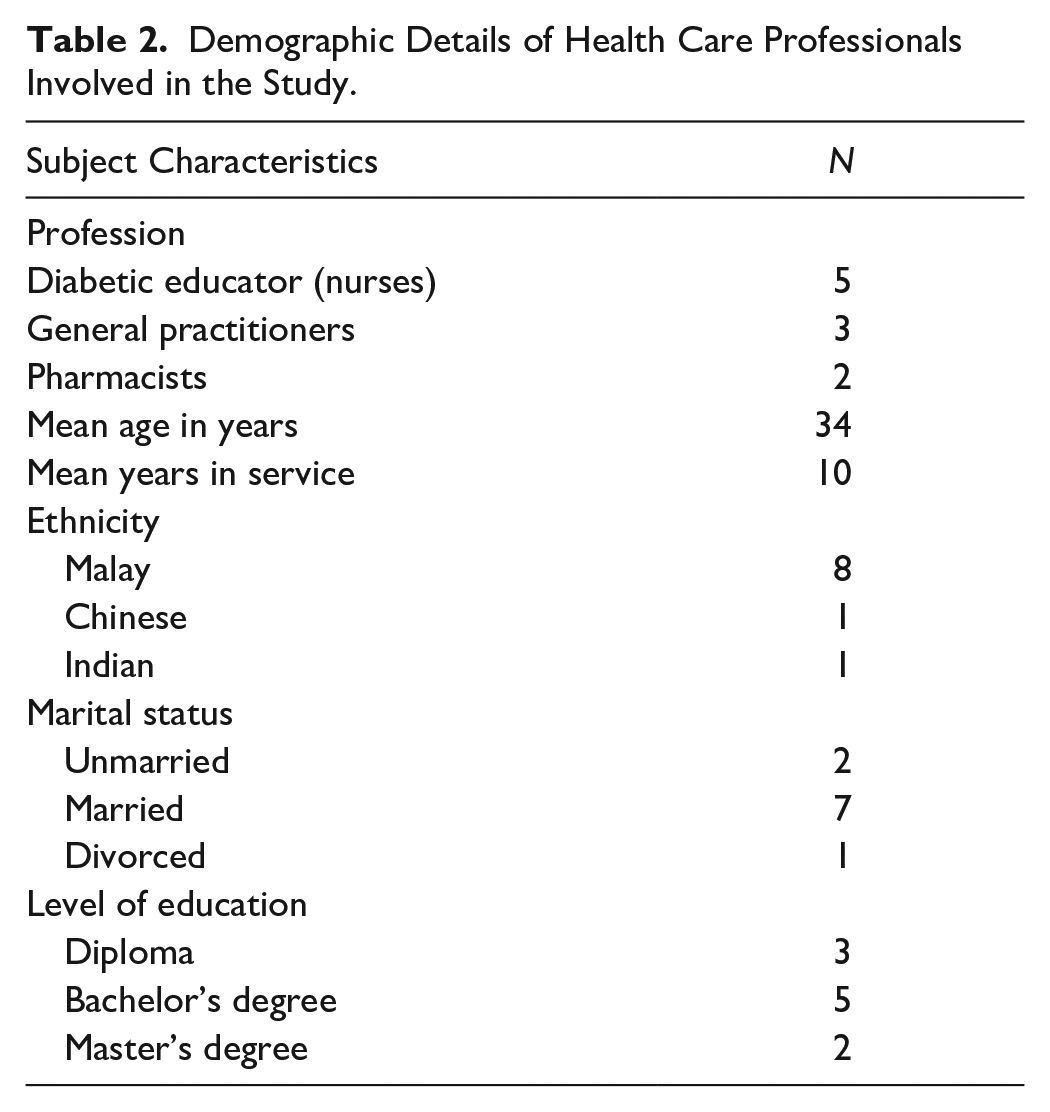
T2D patients were recruited based on a purposive sampling method from the non-communicable disease department at the Seremban Primary Care Centre, a regional multidisciplinary general practice clinic within the state of Negeri Sembilan. A maximum variation strategy was employed to ensure representativeness of the data obtained from the interviews. T2D patients who were invited to participate in the study had the following characteristics: (1) age >18 years, (2) fluent in both English and Malay language, (3) a diagnosis of T2D as documented in their case records, and (4) received followed-up at the clinic for a minimum duration of 2 years. 14 The details about the study was conveyed directly to each patient by the principal investigator during their routine medical consultation at the clinic. Similarly, health care professionals (HCP) comprising general practitioners (GP), diabetic educator nurses (DE), and pharmacists were invited to join the study. After obtaining informed consent, all participants were given an appointment to attend a scheduled interview session.
Data Collection
A total of 24 patients and 10 HCPs were interviewed between May 2018 to February 2019. Subsequently, 2 focus group discussions (approximately 8 T2D patients in both sessions) were conducted as a part of the data triangulation process. All interviews were conducted at a designated research room within the premises of the clinic. A previously published protocol highlights the interviewing techniques, topic guide, and the instruments used during the qualitative inquiry process of this study (Appendices A and B in the Supplementary Material available online). 14 The interviews were audiotaped and transcribed verbatim. One researcher (YSN) conducted all interviews.
Data Management and Analysis
Proofread transcripts were manually coded using a qualitative software (Atlas.ti qualitative analysis program, version 7, Cincorn Systems Inc, 2008) to identify specific themes. The data was coded in accordance with the classical and constructivist grounded theory methods.13,15 In order to connote action into the data, we adopted a process coding technique to interpret all quotations by using gerunds.13
Transcripts were coded independently, and a list of emerging themes and categories were generated. Two independent researchers were also involved in coding the transcript (AACP and GYK) to further establish the robustness of the codes (Cohen’s κ = 0.84). Subsequently, a consensus was established between 4 independent experts on the interpretation of the various themes derived from the transcripts (Cohen’s κ = 0.88).
Ethical Approval
This study protocol received approval from the Medical Research and Ethics Committee, Ministry of Health Malaysia (NMRR-18-151-39886) on May 30, 2018 and also Monash University Human Research Ethics Committee (Project ID: 17062).
Results
The description of the population involved in this study is summarized in Table 1 and Table 2. Table 3 illustrates the main constructs obtained from the qualitative exploration of T2D patients conducted in our study. Our findings demonstrate that the mediators of optimal self-management behavior in T2D patients are determined by 4 major factors—patient expectations, availability of health promotion services, psychosocial support, and a person-centered care (Table 3). These results form a smaller part of a larger study and illustrates the interactions between these factors in the form of a conceptual model (Figures 1 and 2). 14
Demographic Details of the Study Participants With Type 2 Diabetes.

Demographic Details of Health Care Professionals Involved in the Study.
Relevant Themes Describing the Mediators of Optimal Self-Care.

Abbreviations: T2D, type 2 diabetes; CAM, complementary and alternative medicine; DE, diabetes educator; HCP, health care professional.

Conceptual framework the mediators related to self-management beliefs of type 2 diabetes (T2D).
Patient Expectations From Routine Consultations
Patients feel that there is much room for improvements in the way GPs communicate or convey to them information about the nature of their disease. In fact, patients frequently offer suggestions about how an ideal encounter with their GP should be. They feel doctors should take the initiative to recall their medical progress from previous consultations. Additionally, they want GPs to provide them with more information about their disease, medications and test results. A word of encouragement from their GPs appears to boost their motivation to follow through on self-management practices.
If the doctor is nice to us and communicates well, it makes a huge difference. We will not be too stressed about being reprimanded for bad control. And we will be more open towards volunteering information. (Male, IDM 023) I feel it will be better if the doctor could remember the patient’s progress, so that the doctor is aware of the type of medications we’ve been taking and whether there is really a need increase or decrease the dose of the medications. (Male, IDM 010) I hope the doctor can update us better about our condition and give us a clearer picture on our health . . . once they get the results (lab tests), I hope they can explain it to us clearly. (Male, IDM 002) When the doctor communicates well, I feel like I want to control my disease better. (Female, IDM 005)
A commonly held expectation among T2D patients is the desire to reduce the number of medications they need to consume on a daily basis. They harbor the misperception that they will be able to safeguard their health from the negative effects of taking too many medications by doing so.
The doctor keeps increasing (the dosage of) my medication. I don’t like that feeling. I prefer it if I could reduce (the dosage of) my medicine. At least then I won’t feel so sick. (Female, IDM 003) I need to take so much of medications. So many different types of medications, every day . . . it’s killing me, doctor. (Female, IDM 021)
Availability to Health Promotion Services
When asked if they have received any information crucial to their self-care behavior, almost all patients commend the effort of their HCPs in ensuring patients receive practical information pertaining to their disease. Majority of patients believe that their GPs provide adequate information about dietary measures, medication utilization, and insulin administration techniques. Moreover, GPs advise against the use of complementary alternative medication (CAM) without prior consultation with any HCPs.
So I asked my doctor about insulin, whether there are any side effects or anything of that sort. Subsequently, the doctor explained everything to me in detail. (Female, IDM 019) We can’t get upset with the doctor if something goes wrong (after taking CAM). The doctor has already informed us [side effects] about traditional medications. (Female, IDM 006)
Many patients appear to favor health promotion strategies employed by nurses who are trained DEs. Patients feel they benefit from a more personal approach to their disease during a consultation with a DE. Similarly, patients also forge a close relationship with both pharmacists and dietitians with regards to the management of lifestyle factors related to their disease.
Then the diabetic educator told me how to take insulin correctly. And also she motivated me to live my life well. (Male, IDM 007) Then I spoke to the dietician, and she told me what to eat, how I should eat more fruits and things like that. And so I did it for a year. (Female, IDM 024) There was this pharmacist who instructed us how to take the medicine, and also how to store it. (Male, IDM 018)
Psychosocial Support
Majority of patients acknowledge that family support is essential to their disease management. In general, patients share the burden of their disease with their family members and confess their spouses are highly supportive in jointly managing their disease. Children of T2D patients are often concerned about the health of their diabetic parents. They often stress the importance of regulating their diet and frequently remind them to take their medications accordingly. A minority of T2D patients claim that having a close friend makes a positive difference in the way they handle their disease.
Both my children are working (away from home). But I still need them. I need their love and support as I continue to take these medications for the rest of my life. (Male, IDM 002) My children no longer live with me, but they still call up and ask if I’ve taken my medication. (Male, IDM 016) I have a friend; we’ve been friends for 25 years. He’s really a close friend to me. He always advises me about diabetes. He’s also a diabetic too. (Male, IDM 013)
The Influence of Person-Centered Care
Patients anticipate their GPs to embody certain set of positive traits during consultation. For example, patients want more openness from their HCPs and prefer a 2-way discussion about their disease. More importantly, they want GPs to understand their inherent lifestyle and socioeconomic background.
If the doctor is more conversant, I too will ask more questions and volunteer more information. (Female, IDM 006) The doctor has his own duty to advise me. But I have a job as well, with its own struggles. And it’s not easy to just change things to suit the doctor. (Male, IDM 007)
At a personal level, they feel GPs should have more empathy and be appreciative of their needs as a patient. Patients also believe that their adherence to self-management practices is dependent on the quality of the consultations with their GPs.
Doctors these days don’t even talk to you. They just look at you and prescribe the medicine . . . If the doctor is nice, he will talk to them (patients) and that will help us improve the sickness as well. (Female, IDM 003) When patients come to see the doctor, we are already feeling down. So a few words of encouragement will go a long way. (Female, IDM 011)
In general, they are glad that their GPs play the role of being their health advisor reasonably well. Patient-doctor interactions are often cordial and most GPs are often considered very approachable. GPs usually express concern for their patients and treat patients respectfully.
Some doctors are really nice. They go the extra mile for you. (Male, IDM 008) I felt like the doctor looked after me like she was looking after her own son. (Male, IDM 007)
Discussion
Summary of Main Findings
We pursued this study with the objective of deciphering the mediators of self-care beliefs in T2D patients using a qualitative theory-building strategy (Figures 1 and 2, Appendix C). We have primarily described the needs of people with T2D in relation to their disease and the manner in which these factors can help foster better self-management practices. The emergent nature of the data collection process of this study allowed the investigation of novel topics (such as “wanting openness”) that would not have been normally explored using conventional survey techniques. Furthermore, these findings add context to the psychosocial circumstances that surround the daily lives of an archetypal T2D patient. Additionally, this information permits a more practical assessment of behavioral change strategies that are in line with the intrinsic personality of the patient.
Comparison With Literature
There is overwhelming evidence that HCPs should be well-equipped to undertake high-quality person-centered diabetes care. 16 The sustenance of a therapeutic relationship closely hinges on the degree of empathetic interaction between both patient and their caregiver.16-18 Coincidentally, this view resonates with the expectations of a large proportion of T2D patients interviewed in our study—almost all patients suggest that they are willing to be receptive to advice on behavioral change so long as their HCPs demonstrate a clear interest in their personal identity and inherent lifestyle habits. This perception is in line with other studies that show openness to dialogue and genuine expression as an important determinant of effective patient-provider relationship. 19 Therefore, it is evident that both psychological and physical needs of people with diabetes has to be met prior to the utilization of any form of persuasive techniques aimed at instilling better self-management practices.
Our study demonstrates that an optimal family environment plays an important role in empowering T2D patients to comply with self-care practices as advocated by their GPs. This finding is consistent with information found in preexisting scientific reviews, highlighting the significance of psychosocial support in maintaining lifestyle changes essential to self-management behaviors.19-21 In addition, the level of social support received by T2D patients also appears to enhance their degree of perceived self-efficacy in conducting diabetes related tasks. 19 Paradoxically, patients receiving either (optimistically) highly enthusiastic or (counterintuitively) even far too little support from family members may worsen overall diabetes outcomes. 22 Hence, a measured strategy is required to provide the right balance of support to patients and continuously manage the constant psychological distress experienced by family members as a result of looking after T2D patients.16,20
Strengths and Limitations
In Malaysia, a comprehensive chronic disease model was developed from the synthesis of local scientific evidence closely linked to self-care management of T2D patients. 23 However, the conceptualization of this model was not based on meticulous empirical testing nor was it supported by psychological theories fundamental to health behavior research. Thus, this particular process of model building potentially precludes any subsequent attempts to quantitatively evaluate the variables that purportedly influence the mediators of self-care behavior in T2D patients. On the other hand, the hypotheses generated from our study using theory-building techniques (Figure 1 and Appendix A) clearly outlines the mediators of self-care behavior in the form of actionable codes that are amenable to the development of a realistic psychometric inventory.14,24 This specifically designed inventory can help to identify predictors of self-management behaviour and facilitate the implementation of targeted behavioral change interventions in people with T2D.
This study was conducted on the participants originating from only one regional primary care institution. However, the richness and the quality of the data were established through the process of triangulation where selected HCPs from adjacent clinics were interviewed to verify the views expressed by the participants with T2D. Moreover, we emphasized on inclusivity by obtaining participants (1) from a community-based setting and (2) with a mixed sociodemographic background. Although this strategy could have had an impact on the representativeness of constructs obtained from our study, focus group discussions conducted in our study reinforced the view that the belief system in these patients did not deviate much from the narrative collectively shared by the rest of the participants.
Conclusion
In this study, we explored important personal expectations that could help engender a state of positive emotional health in T2D patients. The evidence from our study strongly indicate that effective patient–health care provider communication is one of the major determinants of optimal disease management. Indeed, it has been shown that an increased level of psychological care is associated with better engagement with self-management behaviors in T2D patients.25,26 Furthermore, higher levels of self-efficacy and perceived personal control was seen in T2D patients who had meaningful interpersonal communication with their HCPs. 26 Therefore, HCPs should adopt a more person-centered consultation by modifying their interactions in accordance with the aspirations of people with T2D. 26 HCPs should be trained to be constantly aware that a constructive communication entails the use of empathetic language skills to bring forth a meaningful dialogue with each individual afflicted by T2D. 27
Supplemental Material
Appendix_A_-_Topic_Guide-jpc – Supplemental material for The Internal Realities of Individuals With Type 2 Diabetes: Mediators Influencing Self-Management Beliefs via Grounded Theory Approach
Supplemental material, Appendix_A_-_Topic_Guide-jpc for The Internal Realities of Individuals With Type 2 Diabetes: Mediators Influencing Self-Management Beliefs via Grounded Theory Approach by Yogarabindranath Swarna Nantha, Shamsul Haque, Azriel Abisheg Paul Chelliah, Anuar Zaini Md Zain and Gan Kim Yen in Journal of Primary Care & Community Health
Supplemental Material
Appendix_B_-_Variables_Explored-jpc – Supplemental material for The Internal Realities of Individuals With Type 2 Diabetes: Mediators Influencing Self-Management Beliefs via Grounded Theory Approach
Supplemental material, Appendix_B_-_Variables_Explored-jpc for The Internal Realities of Individuals With Type 2 Diabetes: Mediators Influencing Self-Management Beliefs via Grounded Theory Approach by Yogarabindranath Swarna Nantha, Shamsul Haque, Azriel Abisheg Paul Chelliah, Anuar Zaini Md Zain and Gan Kim Yen in Journal of Primary Care & Community Health
Supplemental Material
Appendix_C_-_Mediators_Quotations-jpc – Supplemental material for The Internal Realities of Individuals With Type 2 Diabetes: Mediators Influencing Self-Management Beliefs via Grounded Theory Approach
Supplemental material, Appendix_C_-_Mediators_Quotations-jpc for The Internal Realities of Individuals With Type 2 Diabetes: Mediators Influencing Self-Management Beliefs via Grounded Theory Approach by Yogarabindranath Swarna Nantha, Shamsul Haque, Azriel Abisheg Paul Chelliah, Anuar Zaini Md Zain and Gan Kim Yen in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We are infinitely grateful to Dr Goh Pik Pin from the National Clinical Research Centre, Malaysia, who has been a beacon in the night, reminding us of the interconnectedness of humanity and urging us to grasp this world and tough moments with strength and grace. In a similar fashion, we would like to thank everyone at Seremban Primary Care Clinic for being our pillar of support throughout this research endeavour.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the MOH-NIH grant (Grant No.:91000440) received from the Ministry of Health Malaysia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.