
Abstract
Introduction
Urbanization and lifestyle changes are occurring rapidly in India, which has resulted in rising prevalence of diabetes in urban and rural areas. In another 20 years, nearly one-fifth of the world’s diabetic population is expected to live in India. 1 The National Urban Diabetes Survey (NUDS), a population-based study conducted in six major cities covering all regions of India reported that the age standardized prevalence of type 2 diabetes was 12.1% and in Chennai, a city in southern India, the prevalence was 13.5%. 2 But according to INDIAB, a national study conducted to determine prevalence of diabetes and prediabetes in India, the prevalence of diabetes in rural Tamil Nadu was 7.8%. 3
As the prevalence of diabetes rises, it is more important to focus on maintaining target blood glucose levels and the prevention of complications among those affected. The patient plays an important role in diabetes management. The patient has to follow self-care practices to achieve target blood glucose levels and prevent poor health outcomes. These self-care practices include regular physical activity, appropriate dietary practices, foot care practice, self-monitoring of blood glucose, and compliance with the treatment regimen. 4 Self-care activities, such as increasing physical activity and maintaining healthy nutrition, can slow disease progression.5,6 Compliance to treatment guidelines helps the patient achieve target glucose level and reduces risk of diabetic complications and mortality.7,8 However, diabetes self-care measures demand a high level of motivation and consistent efforts from the patients
Previous research works have reported poor compliance to self-care practices among patients with diabetes. In a study done in Dehradun, Uttarakhand, in north India in 2010 among patients attending a government hospital, drug compliance to antidiabetic medications was only 16.7%. 9 In a study done in a medical college hospital in Andhra Pradesh, a neighboring state of Tamil Nadu, an area similar to the current study setting in 2010, patients who had higher knowledge scores about diabetes were more regularly involved in self-care practices and achieved better glycemic control compared with those with lower knowledge scores. 10 A cross-sectional study in Canada among persons living with chronic diseases concluded that lifestyle behavior change was prevalent among those who received a health professional advice on self-management in the past 12 months. 11
Studies that evaluate perceived barriers to self-care practices of diabetic patients will bring such issues to light. Few studies have focused on this issue, but they are done in Western populations.12-15 Studies done in India measured self-care practices of diabetic patients but have not focused on barriers to practices.4,6,9,10 To understand in depth the patients’ perceptions on barriers to self-care practices, qualitative research designs will be more helpful rather than quantitative methods. So this qualitative study was taken up to determine perceptions of patients with diabetes about barriers to self-management of diabetes in a rural area.
Methodology
This was a descriptive qualitative study using focus group discussions (FGD) for data collection. Study subjects were recruited from the diabetes outpatient clinic of the Rural Health and Training Centre (RHTC), attached to a medical college hospital in Chennai located 15 km away and where 1200 diabetic patients are registered and are on regular follow-up once in 2 weeks The thematic design of the study is given in Figure 1.
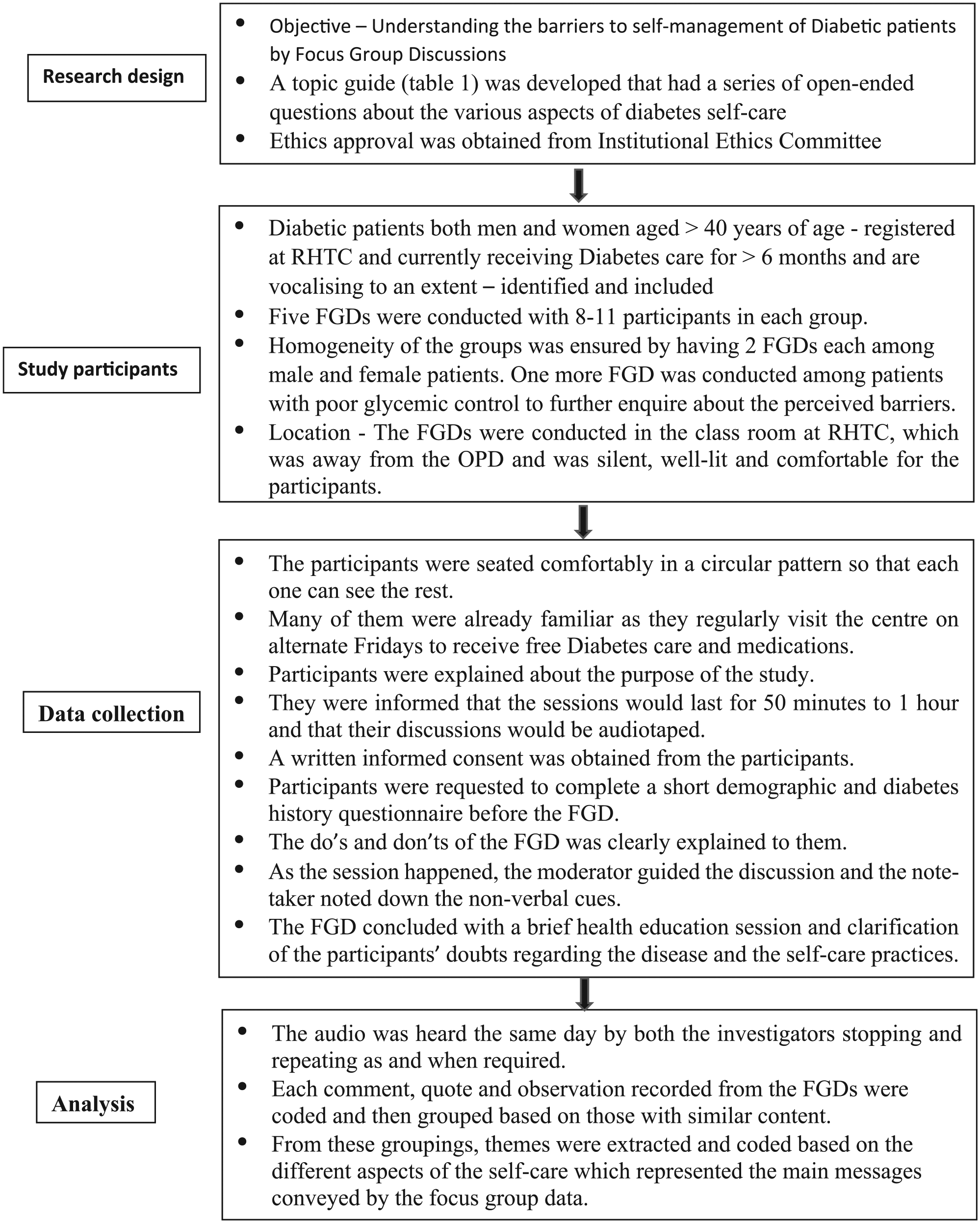
Thematic design of the study.
Study participants were patients with diabetes, men and women >40 years, and on treatment for at least 6 months.
Data Collection
Five FGDs with 8 to 11 participants. A topic guide (Table 1) consisting of a series of open-ended questions covering various aspects of self-care was used by the principal investigator to conduct the session.
Focus group discussion guide used to facilitate discussion in focus groups.

FGDs were moderated by the principal investigator and the co-investigator was the note taker. Both were trained in qualitative research methods. Each comment, quote, and observation recorded from the FGDs were coded, grouped themes were extracted representing the main messages conveyed.
Ethical Considerations
Written informed consent was obtained from every participant. The study protocol was approved by Sri Ramachandra Institutional Ethics Committee (Ref: IEC-NI/15/Feb/45/13)
Results
A total of 50 diabetic patients participated in the FGDs. Mean age of study participants was 58 years with SD of 10.5 years. Nearly 65% of them were living with spouse and other family members and 35% of them were living alone. Nearly 30% of them were illiterate, 27% of them were currently employed, and mean duration of their diabetes status was 4.5 years. The major barriers to self-care mentioned by the diabetic subjects are given as themes in Table 2.
Themes Extracted on Barriers to Self-Care by Patients With Diabetes.

Dietary Modifications
Most patients made dietary restrictions like restricted intake of sweets, nonvegetarian foods, roots, tubers and certain fruits, cut down sugar in tea/coffee following the doctor’s advice. Majority of men had even stopped or moderated alcohol and tobacco use. While restriction was possible with certain items, increasing the number of fruit or vegetable servings was difficult for them due to reasons such as cost and partaking by more family members.
Several of them reported that doctors gave inconsistent advices with regard to intake of rice, porridge, use of millets, restricted use or avoiding tubers and roots and certain fruits like banana, and found this quite confusing.
Many were unable to restrict the quantity of foods. They feared that they will feel hungry or tired after few hours. Also, they were unable to follow divided meals as taking 3 meals a day was their culture. “Will it look nice—eating every now and then?” It was difficult to prepare for one person as the other family members preferred rice-based diet. A man quoted “Roti is to be eaten with gravy, who will prepare for me all this regularly?” One woman said, “Who likes to eat that dry roti everyday?” Millet (ragi, bajra, jowar) porridge or pancakes are more culturally acceptable for them and the whole family partakes them.
Most men were dependent on their wife or daughter-in-law for food and so their cooperation/food preferences played an important role in their compliance to dietary modifications.
Physical Activity
All participants had positive attitude toward exercise programs. Majority of the participants had regular exercise schedule, mostly in the form of brisk walking 30 to 60 minutes a day. Lesser proportion of the participants, mostly women, did not have any exercise regimen. The important barrier perceived by them was their health issues particularly knee joint/leg pain and fear of giddiness/fall. Some expressed their concern of fall—“If I fall who is there for me to support?”
For some, their occupation demands active physical labor, so they do not have separate exercise schedule. One woman said, “I do household work. I don’t need to go for walking.” Another said “I climb stairs 8-9 times a day. So I do not walk.” Few women perceived lack of time was the constraint as they have more household chores.
Foot Care Measures
Almost all of them reported burning sensation in the feet. The symptoms worsen when they walk barefoot and so they always use footwear when they go out. Few said that doctor has advised them to wear socks. No other information on foot care has been given to them by health care professionals. Wearing footwear within the homes is not culturally appropriate in this population.
Drug Compliance
Majority of them regularly take medicines. Some forget to take drugs at least once per week often due to increased household work. One widower mentioned, “My wife used to remind me when she was alive. Now, how can I expect that from my son or daughter-in-law?”
Some do not take drugs during fasting and reported no effect or development of symptoms on skipping of drugs. Few skip the medicines when they go out of town. “Those medications bought in drugstores in those places won’t suit me.”
Complications
Almost all of them agreed that they were not given information on diabetic complications. Very few were only examined for complications and referred. But they are reluctant to go to medical college hospital for screening unless they have got the complications. Others quoted reasons like, “See how crowded the OP is? Where is the time for the doctor to do thorough check-up? I too need to go back soon and cook for my grandchild and so can’t wait.”
Target Blood Levels and Self-Monitoring
Most patients lacked awareness on normal and target blood values. They said, “Doctors say if my sugar levels are high or normal and modify medicines accordingly. But what level should I achieve, none has told.” Charts depicting target values in native language are kept just outside the lab at RHTC, yet people reported not having observed them. Self-monitoring of sugar levels using glucometer was not in practice among the study participants. Most of them were treated with oral hypoglycemic agents and a small proportion with insulin and so use of this device is not routinely prescribed by the treating physicians at the center. Almost all checked their sugar levels once in 3 months at RHTC.
Discussion
FGDs conducted among diabetic patients registered with RHTC of a medical college hospital in Chennai revealed barriers for their self-care practices as culturally inappropriate dietary advice from health care providers, physical constraints, and fear to regularly practice an exercise schedule, poor family support to adhere to dietary modifications and medications, lack of information on foot care measures, target glucose levels, and diabetic complications.
A cross-sectional study in rural and urban slum areas in Gujarat showed similar findings namely, more males were adherent to physical activity than females, 63% could restrict sweets and fats but only 19% reported taking at least one fruit/vegetable serving most of the days. 4 Simmons, 16 in his article, has quoted barriers to self-management such as low diabetes knowledge, lack of family support, increased family demands, negative perception of time, and so on, which are similar to that identified in our study.
In south India, the staple diet is rice and diet advice is given on wheat-based diet (rotis) by the health care providers with the intention to decrease the quantity. People find this culturally unsuitable for them. But they have preference to include millets mainly ragi, bajra, and so on, in their diet. It is better for health care providers to be familiar with local cultural practices and identify individual preferences and difficulties before giving advices on diet.
Physical constrains and fear are the barriers for majority of the diabetic women in following a regular outdoor walking. A qualitative study from Baghdad has reported similar reasons such as busy with household chores, physical restraints as barriers for regular exercises. 17 Studies have proven that even simple feasible exercise programs are effective in improving glycemic control such as post meal walking for 15 minutes. 18 A recent study in Chennai proved that mild physical activity of 5 minutes walking/hour every day and compliance to medications are effective in glycemic control. 19 These can be promoted among diabetes patients who have limitations in mobility and who cannot walk for sustained period of time.
Although the Indian Council of Medical Research has given guidelines on various aspects of foot care among patients with diabetes, 20 hardly any are aware of these. The main barrier identified for noncompliance to foot care measures is inadequate information received from health care providers. A study in central India in a similar rural training hospital reports that 63% of the patients have not undergone foot examination or received education regarding foot complications or foot care by their treating physicians. 21
Lack of information from health care providers was the barrier for foot care measures, target blood levels, screening for complications. Other qualitative studies also reported similar finding that majority of participants were not aware of target blood glucose levels.22,23 Providing them information proactively through small group education programs will go a long way in promoting healthy lifestyle practices and drug compliance. This would promote early health seeking, better reporting of complications and bring down the cost of care for both the patients and the provider.
Conclusion
The barriers to self-management identified in this qualitative study are amenable to intervention that could improve health outcomes. Health education on lifestyle modifications must be tailor made taking into consideration their family and social background.
Footnotes
Authors’ Note
This study was presented at the Indian Association of Preventive and Social Medicine Conference 2016, Gandhi Nagar, Gujarat on January 7, 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.