
Abstract
Introduction
Anemia is a common public health problem worldwide, affecting 32.9% of the total population. 1 Southeast Asia has the largest number of women and children who suffer from anemia, with more than 200 million women and 96 million children, and more than half occurring in developing countries.2,3 In Indonesia, anemia is a frequent health concern, with a prevalence of 22.7% in women of childbearing age, 37.1% among pregnant women and 30.0% to 46.6% among female workers.4-6 Anemia, particularly iron deficiency anemia, is associated with nutritional problems, which are considered national health issues. 7 In 2012, the United Nations Children’s Fund collaborated with the Indonesian government to conduct a nutritional survey in three districts. They found that around 6% of children and 45% of pregnant women suffered from anemia, and among children, 30% were stunted, 20.8% were underweight, 8.6% were wasted and 1.2% were malnurished. 8 Maternal anemia has been linked with low hemoglobin concentrations in infants, regardless of nutritional intake. 9 Anemia should be taken seriously in women of childbearing age as it not only affects the health and work performance of the women themselves but also the growth and development of their children, productivity of communities, and national development. The World Health Organization (WHO) has recommended and supported various programs, such as iron supplementation, food fortification, health education, and parasitic infection control to reduce the prevalence of anemia. 10 However, global trends in decreasing anemia prevalence suggest that current efforts are still insufficient. Likewise, the Indonesian government established a 90-day iron supplementation program for pregnant women. Nevertheless, only 89.1% of all pregnant women receive supplementation, and only 33.3% take this supplementation for at least 90 days. 4
The workplace not only represents the place in which a high proportion of female workers spend most of their day but also presents a high potential risk to health and anemia. Workplace-based health promotion efforts should be reinforced to target female workers as they play an essential role in the family and are increasingly involved in labor.
Aim of the Study
The present study aimed to investigate anemia from the perspective of female workers and their anemia-related experiences in the workplace as well as identify strategies for improving workplace-based intervention.
Methods
We used a qualitative method with the phenomenology approach to explore phenomena or personal experiences. In the present study, we evaluated the phenomenon of anemia among female workers through their experiences. 11
Data were collected via focus group discussion (FGD) since this was an ideal approach to assess female workers’ knowledge, perception, and beliefs on anemia prevention and related factors. The present study assessed their eating patterns, iron intake, occupational and individual risk factors, and health service from social and cultural aspects that were all included in the FGD questionnaire developed based on the combined model of the theory of reasoned action and the enabling factor.12-14 Seven main questions relating to definition, etiologies, signs and symptoms, consequences, and participants’ experiences related to anemia treatment and prevention encouraged a more in-depth discussion among participants. Questions aimed to explore 3 kinds of influencing factors: beliefs and attitudes, subjective norms, and enabling factors. Questions on beliefs and attitudes related to participants’ understanding, awareness and experience of anemia, and the importance of its prevention. Subjective norm questions were related to influencing factors and reasons for choosing particular foods, such as family, culture, and religion. Finally, questions relating to enabling factors focused on the factory canteen service, economic factors, and health services. The initial question was always about participants’ experiences or understanding of anemia, while subsequent questions were not asked in any particular order to allow the participants to express their ideas and views in their own way.
FGDs were conducted in a factory located in East Jakarta, Indonesia, which employed 1975 workers, among whom 440 (22.3%) were female. Of the 440 female workers, 279 (63.4%) worked as production line operators. Participants were allocated to 1 of 14 FGDs according to anemia status (anemic, nonanemic) and potential affecting characteristics, including marital status (unmarried, married with <3 children and married with ≥3 children), educational level (≤12 years, >12 years), ethnicity (Javanese, Sundanese, Sumatran), religion (Muslim, non-Muslim) and health consultation frequency per year (<6 times, ≥6 years). 15
Female workers were selected according to their work shift schedule and willingness and ability to participate. Fifteen female workers were invited for each FGD group but were excluded if they had health problems or were unable to actively participate in discussions.
The FGDs were moderated by the main researcher, and an observer, who has been trained for the study, helped to record the discussion using an audio tape and noted the verbal and nonverbal expression. Data were transcribed and analyzed via coding. Any similarities in keywords were clustered together as categories. Themes related to belief and attitudes, subjective norms, and enabling factors (BASNEF model) of anemia were identified. 13 Analysis of verbatim data was performed manually by listening to the recording and reading all the notes, summarizing content areas and themes and making tables, where appropriate.
The present study received ethics approval from the Health Research Ethics Committee, Faculty of Medicine, Universitas Indonesia. Participants gave written informed consent prior to taking part in the interviews.
Results
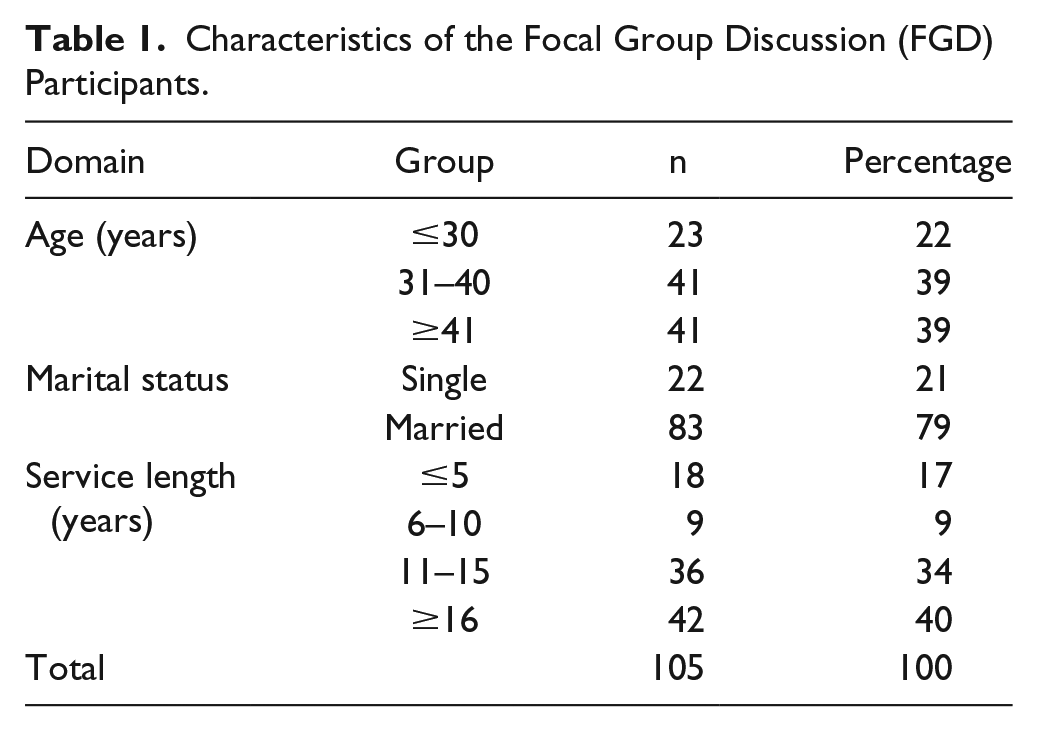
For each FGD group, 15 female workers were invited to participate; however, only 6 to 9 female workers per group chose to participate, resulting in a total of 105 participants. Table 1 presents the characteristics of the participants, and Table 2 presents the characteristics based on the FGD groups.
Characteristics of the Focal Group Discussion (FGD) Participants.
Characteristics of Participants According to Focal Group Discussion (FGD) Group.

The results examined (1) beliefs and attitudes, (2) subjective norms, and (3) enabling factors. Beliefs and attitudes explored female workers’ understanding, experience, and awareness of anemia. Subjective norms included various factors related to eating patterns, such as family, work environment, culture, and religion. Enabling factors identified accessibility of food supply, economic factors and available factory and public health care services.
Beliefs and Attitudes
More than half of the participants had heard about anemia and were able to answer questions on its signs and symptoms correctly; however, some did not understand the meaning of anemia. The term anemia in Bahasa means kurang darah and describes having low blood volume. Some participants defined anemia as having more white than red blood cells, while others thought it meant having low blood pressure.
The reason for this misunderstanding may be associated with the term pil tambah darah, which means “pill to increase the volume of blood.” Pil tambah darah is a popular name for iron supplementation tablets. Many participants mistakenly believed this drug was a medicine to increase blood pressure, instead of increasing the oxygen carrying capacity.
Symptoms were commonly described as the 3 Ls, standing for lesu, letih, and lemah. These words are translated as weary, fatigue, and weak. Lesu refers to a person who is psychologically weak but physically well. Letih describes a person who is both physically and psychologically weak. The term lemah is used to describe a person who is physically weak. These 3 terms were originally introduced in a famous commercial advertisement for an iron supplement. Participants described symptoms such as headache, nausea, and tiredness. When asked about the possible causes, most participants answered exhaustion from work, lack of sleep, and menstruation. They also mentioned possible causes in the workplace such as lead, which was used during the soldering process and use of benzene or toluene as a solvent.
Subjective Norms
All participants agreed that prevention and treatment of anemia were important. They believed that family and personal circumstances required them to be in good health and perceived that anemia would affect their ability to work and take care of family members. The concept of anemia was heavily influenced by advertisements, particularly from television. One advertisement selling iron tablets described symptoms of anemia, such as tiredness, headache, weakness, and feeling weary. Moreover, it marketed the iron supplements as part of anemia prevention.
They also believed that eating healthy foods, such as green leafy vegetables, meat, and poultry, could treat anemia. For the Sundanese, eating raw green leafy vegetables was very common since it was part of their culture. They believed eating vegetables would make them healthy and beautiful. Unfortunately, participants were reluctant to consume iron supplement tablets and were concerned about the symptoms they experienced, such as headaches, nausea, loss of appetite, and weight gain. They preferred to give tablets to male workers to feed their chickens. Some participants argued that consuming iron supplements would increase their blood volume, leading to increased blood loss during menstruation and childbirth.
Chronic blood loss due to menorrhagia is one of the causes of nutritional anemia. However, many women were reluctant to see a gynecologist, especially male physicians. In terms of religion, the largest population in the factory was Muslim, followed by Protestants and Catholics. Other religions, such as Hinduism, Buddhism, and Confucianism, were not found in this study. There was no difference between Muslims and Christians in terms of patterns of iron-rich food intake, and none of the female workers were vegetarian.
Enabling Factors
Health Services
The present study revealed that many participants were dissatisfied with the available health services in the factory and complained about insufficient health information during the consultation time. One participant stated that she preferred to visit a private clinic, despite having to pay for it, as it would provide a more satisfactory service.
Participants also discussed the most convenient methods and times to deliver health information. Health professionals were preferred over their own peers, factory management, or trade union.
Health information in the form of bulletins or leaflets was considered ineffective. Most workers reported being too tired during their spare time and not having time or an interest in reading information leaflets. Overtime work schedules, conflicting work shifts, and after-work family obligations were major barriers for workers receiving health information via reading material.
The factory established a “Healthy Friday” program, which provided health education to all workers. However, many participants were not interested in the program since the health information was delivered in the style of a lecture to hundreds of participants.
Food Quality and Quantity in Factory Canteen
The Indonesian government established regulations stating that companies must provide food for night shift workers as stated in the Decree of the Minister of Manpower and Transmigration. 16 However, in terms of quantity, participants complained that the food provided in the canteen was insufficient. Many were reluctant to have lunch in the canteen because there was not always enough food to go around. Many participants also complained about the taste of the food, as well as hygiene and quality. Some workers that complained about the taste preferred a home-cooked meal, street food, self-cooked instant noodles, or even fasting. Those who complained about hygiene mentioned finding a piece of rope or worm in their meal and that the chicken was not cooked properly.
Participants who ate in the canteen were satisfied with the menu, especially meat and poultry, since these were considered expensive and not available at home. The menu offered several options, such as chicken, meat, fish, tofu, tempeh (a soybean product), and various vegetables. Each meal comprised a combination of 2 or 3 dishes with rice as a staple.
Discussion
The present study adopted Hubley’s behavioral change model as the template analysis and explored female workers’ perception of iron-deficiency anemia, examined its risk factors and identified the most suitable prevention and management strategies for anemia in the workplace.
Beliefs and Attitudes
Some participants mistook anemia for low blood volume, instead of low hemoglobin level. They received information mostly from the media. Television commercials for iron supplements were popular among participants and highly influenced their understanding of anemia. Griffiths 17 previously highlighted the influence of the media in promoting positive as well as potentially risky health behaviour. However, the message delivered in the commercials only focused on consumption of iron supplements and did not mention the importance of consuming iron-rich foods.
For participants, consuming iron tablets was one of the main anemia treatments, but acceptance was very low since many participants were reluctant to consume them due to their perception that they caused heavy blood loss during menstruation or childbirth. A study by Galloway et al 18 among pregnant women in eight developing countries found that most women had a false perception of iron consumption causing high blood volume and challenging childbirth. Another predisposing factor was weight gain, as mentioned by participants during decisions about taking iron supplements.
Regarding the etiology of anemia, many participants were aware of the possible effects of chemical exposure on their health. Lead exposure may inhibit several enzymes involved in heme biosynthesis and destroy cell membranes. 19 Moreover, King 20 reported that lead toxicity increased intracellular iron in bone marrow erythroblasts, intensifying the production of amino levulinic acid dehydratase and protoporphyrin, eventually increasing ferritin synthesis and leading to anemia. 20 Additionally, benzene could interact with oxyhemoglobin and form superoxide radical species in red blood cells, potentially exposing red blood cells to oxidative stress, causing cellular damage and affecting the integrity of lipid membranes. This process would increase the risk of membrane rupture and haemolysis. 21 However, there was no active prevention for the potential risk of these exposures as no cases were reported.
Subjective Norms
Leafy green vegetables were commonly consumed as appetizers or side dishes as they were affordable and part of the culture. Vegetables contain nonheme or inorganic iron, which is more difficult to absorb than meat or other heme iron food. 22 Heme iron accounts for more than 95% of functional iron in the human body and is predominantly found in meat, poultry, and fish. Certain diet, such as betel leaves, tea, coffee, and cocoa, could also reduce iron absorption. 23 However, vitamin C consumption may enhance nonheme iron absorption. 24
Anemia was commonly caused by poor intake, deficiency of iron, folate and vitamin B12 and diseases such as malaria, parasitic infection, HIV infection, chronic inflammation, and hemoglobinopathies.25,26 Certain populations are more prone to iron-deficiency anemia since the daily requirements differ with age and sex. Women generally require more iron than men, particularly those who are pregnant or breastfeeding. 27
Enabling Factors
According to the Centers for Disease Control and Prevention, the workplace is an important setting for health protection and promotion and disease prevention programs as it is where workers spend a substantial amount of their time. Therefore, companies play an important role in promoting a healthy lifestyle for their employees. Workplace wellness initiatives are reported to be growing in numbers as employers are increasingly aware of the benefits of these initiatives, such as the increased productivity and health cost savings. 28 In the present study, many participants viewed iron supplements negatively due to their perception of the side effects; however, iron-rich foods were more acceptable. Therefore, nutrition programs would be preferable for this community.
Promotion of healthy eating in the workplace is supported as a part of the WHO’s Global Strategy on Diet, Physical Activity and Health. 29 A randomized intervention study of 29 companies showed that changes in the work environment based on the ecological model for health promotion increased employees’ consumption of fruit and vegetables. 30 While hunger is the key driver for eating, several other influential factors that determine food choices include cost, income, time, availability, and physical and social determinants. 31 These factors should be considered when analyzing eating behavior and nutrient intake in female workers. Canteens should provide an appropriate alternative for female workers; however, the utilization rate of the canteen was relatively low due to insufficient quantity and poor quality of food. Therefore, companies should encourage female workers to become involved in food preparation to attract more female workers to eat in the factory canteen. Alternatively, companies could also ask workers to help decide the daily menu.
Health professionals also play an important role since they are more trusted by employees compared with their peers, management, or trade unions regarding health information. Health professionals were considered to have sufficient updated health knowledge and to spend more time to discuss workers’ health-related problems. A study among male workers in Korea by Kim et al 32 found that systematic nutritional education or consultation programs significantly improved body mass index, fasting blood sugar, and cholesterol levels. In Britain, almost all Muslim women have a strong preference for female doctors and hesitate to see male doctors for internal examinations. 33 However, in the present study, gender issues were not a serious obstacle in seeking medical advice. Three out of 5 doctors in the factory clinic were female, and the participants were willing to discuss menstruation. However, they did not consider heavy menstrual bleeding as a serious medical condition and would only attend the clinic if pain accompanied the condition.
Financial problems were another important factor. In Indonesia, workers receive a relatively low take-home pay, even those working for a multinational company. During the discussion, workers who had worked in the production lines for over 10 years only received around $205.73 per month. In comparison, the price of 1 kg of beef was around $9.17, and a whole chicken was $4.97. Financial constraints were a barrier to consumption of meat and poultry in female workers. Some participants overcame this by limiting their outgoings for clothes, household equipment and electrical equipment.
Study Limitations and Strengths
The present study has some limitations. First, the participation rate was quite low as it only included 40% to 60% of 15 invited participants in each FGD. This low participation rate may have been due to the survey taking place during working hours and participants being reluctant to leave their work despite having permission from the company. However, our results provide new insight to improve anemia prevention and control programs in the workplace.
Conclusion
Workplace-based intervention programs may be applied to anemia prevention in female workers. We propose that workplace-based intervention can be improved by integrating nutrition education as well as improving factory canteen and health services based on women perspectives. First, workplace-based nutrition education is effective in improving female workers’ knowledge of the importance of anemia prevention and control by consuming iron-rich food, such as leafy green vegetables. Second, factory canteen services should be improved to provide nourishing meals and compensate for family food shortages due to financial constraint and cultural barriers. Third, factory health services should move from a curative approach toward a health promotion and preventive approach via workplace hazard prevention and control. A workplace-based intervention program would benefit female workers by enhancing iron-rich food intake and minimizing risk of occupational and environmental anemia.
Footnotes
Acknowledgements
The authors express their gratitude to the company management for valuable supports, and all managers and women workers as study subjects for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding support from the Directorate of Research and Community Development Universitas Indonesia through the 2018 research funding No. 5282/UN2.R3.1/HKP 05.00/2018.