
Abstract
Keywords
Introduction
Diabetes is a major public health issue worldwide, and the prevalence of prediabetes and diabetes is increasing. 1 The estimated number of people with impaired glucose tolerance and diabetes worldwide was 352 and 425 million, respectively, in 2017, and is projected to increase to 532 and 629 million, respectively, in 2045. 1 This presents a great burden on health care systems. Accumulated evidence shows that changes in diet and physical activity among people with impaired glucose tolerance can reduce the incidence of type 2 diabetes by 50%, and that effective interventions should be group-based to reduce cost and call attention to specific behavioral changes.2,3
The prevalence of pre-diabetes and diabetes in Thai adults aged ≥20 years has been estimated at 15% and 8.9%, respectively.4,5 To meet the growing challenge, healthcare service providers should focus on the prevention or at least delay in onset of type 2 diabetes. Several randomized trials have provided scientific evidence that the incidence of diabetes can be reduced through lifestyle interventions, although a few interventional studies were carried out in contexts different from real-world settings.6-8 Systematic reviews have reported that the effectiveness of lifestyle interventions in real-world settings varied widely.3,9,10 More practical research is required, to apply the knowledge into clinical and public health practice accounting for local context. The effectiveness of the group-based approach in middle-income Asian countries is unclear. To assess whether lifestyle modification can delay or prevent diabetes, we conducted a clustered randomized controlled trial in a community-based primary care setting. The Thai diabetes prevention program was a 2-arm primary care-based clustered trial designed to evaluate the effectiveness of lifestyle intervention among adults with prediabetes versus one-time health education as standard care. Our hypothesis was that individuals in the intervention program would see a greater mean reduction in weight and body mass index (BMI) and a lower incidence of diabetes over the succeeding 24 months.
Material and Methods
Study Design
The Thai diabetes prevention program was a 24-month, matched-pair cluster-randomized controlled trial. A total of 68 primary care units (PCUs) in 8 provinces distributed in 4 geographic regions of Thailand participated in the study. A matched-pair design for PCU was developed to ensure balance on 2 characteristics of PCU: total number of health care personnel, and type of occupation in the community as proxy of socioeconomic status. Each PCU is the unit of randomization. In each province, 8 to 10 PCUs were paired 1:1; one of each pair was randomly assigned to the intervention or the usual care arm by computerized random allocation by a researcher in the central office who was blinded to the identity of the primary care unit.
Participants and Setting
Study participants were recruited by a screening program for individuals with a high risk of diabetes conducted by district PCUs. The inclusion criteria for screening into the intervention study were (a) age 30 to 65 years, (b) no previous diagnosis of diabetes, and (c) local people of the villages in the jurisdiction of the PCUs under study. Based on the Thai national health survey in 2014, the prevalence of impaired fasting glucose in the Thai population was 20%. 5 Therefore, in each PCU, a total of 150 to 300 individuals were screened to identify a total of 30 to 65 individuals with a high risk of diabetes. The screening and recruitment of study participants took place between February and August of 2013. Recruitment strategies included meeting with community leaders and village health volunteers to inform and recruit members. Informed consent was obtained from the participants after verbal and written descriptions of the study were provided. Initially, participants aged 30 to 65 years were screened using the Thai diabetes risk score questionnaire 11 and random capillary glucose testing. Those at high risk of developing diabetes (risk score ≥6) or with a random capillary glucose reading of ≥120 mg/dL were then administered an oral glucose tolerance test (OGTT). A total of 11 449 individuals without a previous diagnosis of diabetes were tested for glucose tolerance; 2381 individuals with impaired glucose tolerance (IGT, 2-hour plasma glucose ≥140 mg/dL and <200 mg/dL after ingestion of 75 g oral glucose load) but without diabetes were identified and further invited to participate, and 1903 consented. 12 Finally, the eligible inclusion criteria were (a) age 30 to 65 years, (b) no diabetes, (c) local people of the villages in the jurisdiction of the PCUs under study, and (d) impaired glucose tolerance (2-hour plasma glucose ≥140 mg/dL and <200 mg/dL after ingestion of 75 g oral glucose load).
Sample Size
The number of participants in each cluster and PCUs was calculated based on the requirement to detect a 50% relative decrease in the incidence of diabetes over 2 years with a type I error of 0.05 and 80% power. The decision for the number of clusters and cluster size was made concurrently in order to maintain the power. 13 The sample size for number of cluster per group (C) with a assigned cluster size (n) was calculated based on the following formula14,15:

where π0 and π1 are the incidence of diabetes in the usual care (6.2%), based on a previous study, 16 and intervention arm (3.3 %), respectively, k is the between-clinic coefficient of variation (CV) of the true proportions = 0.25. Let zα/2 = 1.96 and zβ = 0.84. Consequently, the cluster (PCU) number required per study arm was 34, with 30 individuals at high risk of diabetes in each PCU.
Figure 1 is a flow diagram of the study. This study was approved by the Ethical Clearance Committee on Human Rights Related to Research Involving Human Subjects, the Faculty of Medicine Ramathibodi Hospital, Mahidol University. The trial was registered and approved by Thai Clinical Trial Registry committee which is one of the World Health Organization’s International Clinical Trials Registry platform.

Flow diagram of the study.
Intervention Program
The intervention program consisted of 3 steps. First, a preparation step, the research team design the contents of the intervention program all of which were approved by specialists related to the topics. Second, a preparation step included carrying out a workshop for the local health care providers on creating learning activities for the participants and the way to facilitate group activities. Third, an implementation step, participants in the intervention group attended a 3-day workshop followed by a half-day workshop once a month for 6 months. Over the following 18 months, participants engaged in group activities every 2 months for a total of six sessions and every 3 months for the last 2 sessions. The intervention aimed to empower participants to manage their own risks by acquiring knowledge (what to do) and skills (how to do it), developing confidence and motivation to perform appropriate self-management (want to do it), and developing problem-solving and coping skills to overcome barriers to self-management (can do it). 17 In each workshop, participants engaged in predesigned activities and knowledge sharing, exchanging experiences related to their lifestyle practices and learning from each other in a small group setting. The workshop sessions covered topics: raising awareness of diabetes, smart food choices, spiritual and mindfulness, exercise and physical activity, weight management, and emotional management, sufficient economy, self-reliance.
Control Group
Participants in the PCUs randomized to the standard-care arm received standard advice concerning lifestyle modification for individuals at high risk of diabetes. This included information on weight reduction, physical activity, and dietary patterns to reduce unnecessary fat intake.
Data Collection and Measurement
Participants were interviewed by research nurses on demographic data: age, sex, educational level, and occupation. At baseline, 6, 12, 18, and 24 months, individuals in both groups were measured for their body weight using calibrated balance beam scale. Height was measured with standard stadiometer. Blood samples were obtained for measurement of fasting plasma glucose (FPG), 2-hour plasma glucose (after ingestion of 75 g oral glucose load) and serum lipid parameters. Plasma glucose was measured by hexokinase enzyme method. Serum total cholesterol and triglyceride were measured by enzymatic colorimetric methods. High-density lipoprotein cholesterol was analyzed by homogeneous enzymatic colorimetric methods using the Hitachi 917 model. The lipid measurement was standardized to the criteria of the Center for Disease Control and Prevention Lipid Standardization Program.
Outcomes
Primary outcome: Incidence rate of diabetes among subjects with a high risk of diabetes at 6, 12, 18, and 24 months after the intervention commenced. Diabetes was defined as an FPG level ≥126 mg/dL, or a 2-hour plasma glucose level ≥200 mg/dL after ingestion of 75 g oral glucose load.
Secondary outcomes: Reductions in body weight, BMI, FPG, and serum lipid parameters such as total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides.
Data Analysis
Means and standard deviation were calculated for continuous variables (age, weight, BMI, and lipid parameters). Comparison of means between groups at baseline was performed by t test. Chi-square test was used to compare between categorical variables. Changes in primary and secondary outcomes were calculated and presented with descriptive statistics. The incidence of diabetes per 100 person-year in the intervention and control groups was calculated at 6, 12, 18, and 24 months and compared. Changes in weight, BMI, and lipid parameters between baseline and month 24 in each group were calculated. A survival curve of probability of participants remaining free of diabetes was constructed by Kaplan-Meier method. A Cox proportional hazard regression was used to examine factors associated with the incidence of type 2 diabetes. Test of proportional hazard assumption was conducted, and the results showed no violation of the assumption (χ2 12.3, P = .07). Hazard ratio and 95% confidence interval (CI) in the intervention group compared to control group was calculated with adjustment for age, sex, baseline FPG and BMI. A mixed model was used to determine the differences of changes in weight, BMI, and lipid parameters at 12, 18, and 24 months, between the intervention and control group adjusted for age and sex. All the statistical analyses were performed using Stata 13 (StataCorp LLC, College Station, TX, USA). Intention-to-treat was applied in the analysis for the incidence of diabetes.
Results
A total of 1903 individuals participated in the study. Of these, 873 participants were in the PCUs assigned to the control group and 1,030 were in the PCUs of the intervention group. The mean age was 50.9 and 50.7 years in the intervention and control groups, respectively. About 80% of participants in each group were female.
Table 1 shows the baseline characteristics of study participants. There were no significant differences between the intervention and control groups in sex, age, educational status, occupation, baseline FPG, 2-hour plasma glucose, and low-density lipoprotein cholesterol levels. Body weight, BMI, and triglyceride levels were slightly lower in the intervention group; high-density lipoprotein levels were lower in the control group. There were 146 (16.7%) participants in control group and 111 (10.8%) in the intervention group who were lost to follow-up due to several reasons as shown in Figure 1. During the follow-up period, 5 individuals in the intervention group died; causes of death were asthma (1 case), motor cycle accident (1 case), cirrhosis (1 case), hepatitis (1 case), and 1 case of breast cancer. Three people in the control group died due to motor cycle accident (1 case), renal failure (1 case), and 1 case of asthma with pneumonia. All the deaths were not related to the program and no adverse event was reported (Figure 1).
Baseline Characteristics of Study Participants. a

Chi-square test was used to compare categorical variable and t-test was used for comparison between two means.
Venous plasma glucose 2 hours after ingestion of 75 g oral glucose load.
Incidence of Diabetes and Normal and Impaired Glucose Tolerance
After the 2-year program, the incidence rate of diabetes in the control group was higher than in the intervention group (16.6%; 95% CI 14.6% to 18.8% vs 12.1%, 95% CI 10.7% to 13.8% per year, respectively, P < .001). At the 6-, 12-, 18-, and 24-month time points, the diabetes incidence was 26.5%, 17.6%, 9.8%, and 7.3%, respectively, in the control group and 17.3%, 13.2%, 6.1%, and 10.1%, respectively, in the intervention group. Figure 2 shows the proportion of participants remaining free of diabetes during the study.

Proportion of individuals without diabetes by group over time.
The hazard ratio for diabetes incidence was 0.61 at 6 months (95% CI 0.47-0.81), 0.65 at 12 months (95% CI 0.53-0.81), 0.64 at 18 months (95% CI 0.53-0.78), and 0.71 at 24 months (95% CI 0.59-0.85). The relative risk reduction after 24 months was 29%. The number of participants who adhered to the program over time was higher in the intervention group than in the control group. A total of 627 (71.8%) individuals in the control group and 919 (89.2%) individuals in the intervention group completed the study.
Changes in Body Weight and BMI
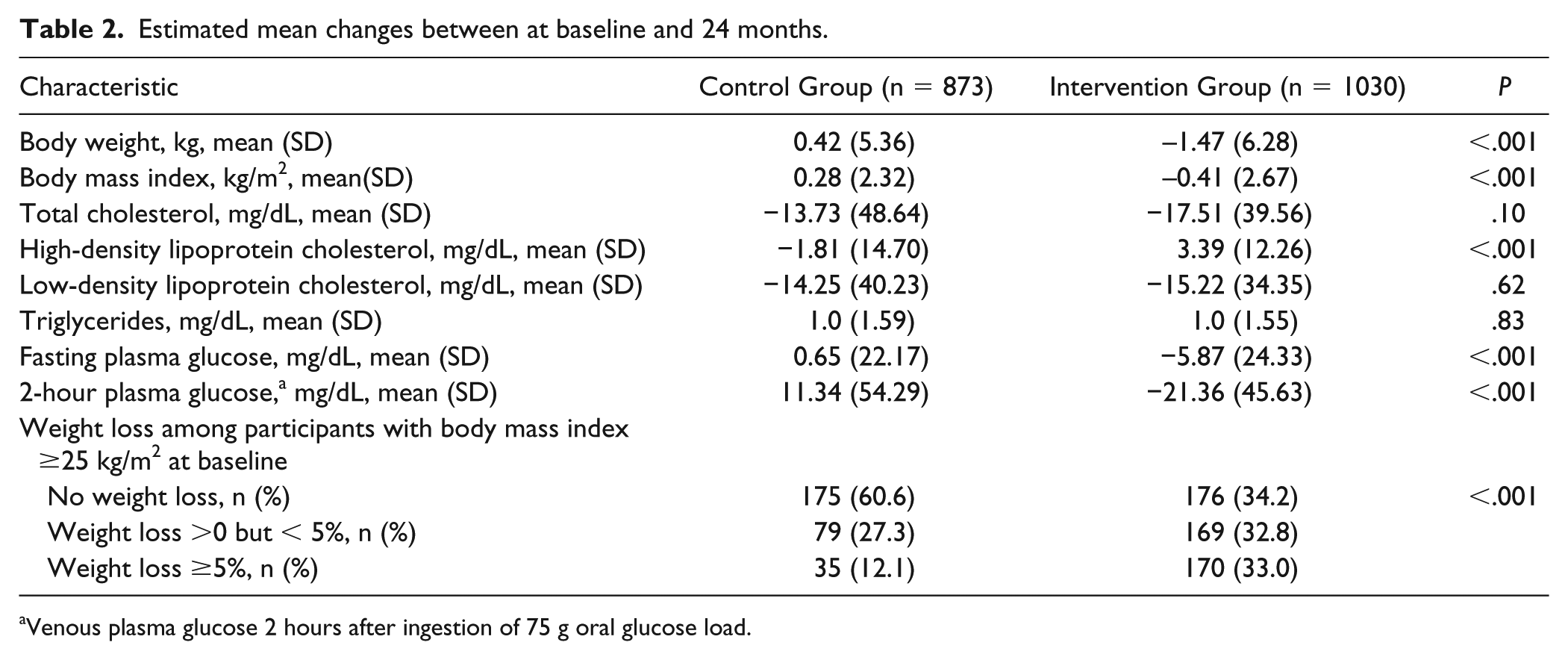
There was slightly increase in body weight and BMI among the control group, but significant reductions in body weight and BMI were observed in the intervention group in 6, 12, 18, and 24 months. Compared with baseline, at month 24, the average changes in body weight in the intervention was −1.47 kg, which equated to a reduction of −0.41 kg/m2 for BMI. At the end of the study, among participants with BMI ≥25 kg/m2 at baseline, 33.0% lost ≥5% and 32.8% lost some weight but less than 5% in the intervention group. In the control group, however, 12.1% lost ≥5% and 27.3% lost some weight but less than 5%. There were no significant differences in changes of lipid parameters between groups except for a significantly increase in high-density lipoprotein cholesterol (HDL-C) only in the intervention group with an average of +3.39 mg/dL. Overall, there were significant reductions in FPG and 2-hour plasma glucose in the intervention group, but not in the control (Table 2).
Estimated mean changes between at baseline and 24 months.
Venous plasma glucose 2 hours after ingestion of 75 g oral glucose load.
Table 3 lists the incidence of diabetes at the end of the study, stratified by various factors. Overall, after adjusted for age, baseline weight, FPG, and 2-hour plasma glucose, the risk of diabetes was lower among participants in the intervention group (adjusted hazard ratio [HR] 0.72, 95% CI 0.6-0.86). The intervention group reduced the risk of diabetes incidence in both sexes; female (adjusted HR 0.77, 95% CI 0.62-0.94), and male (adjusted HR 0.64, 95% CI 0.44-0.92). The incidence also significantly decreased in those aged <50 years and those ≥50 years. However, the HR was significant among those with BMI ≥25 kg/m2 with (0.68, 95% CI 0.5-0.84), FPG ≥110 (0.55, 95% CI 0.40-0.74) and oral glucose tolerance level ≥153 mg/dL (0.69, 95% CI 0.56-0.86).
Diabetes Incidence (per 100 Person-Year) at the End of the Study, Stratified by Patient Characteristics.

Abbreviations: HR, hazard ratio; CI, confidence interval.
Adjusted hazard ratio controlling for sex, age, baseline body mass index, fasting plasma glucose, and 2-hour plasma glucose.
Venous plasma glucose 2 hours after ingestion of 75 g oral glucose load.
Discussion
The present study shows that in primary care settings, lifestyle modification programs to prevent diabetes among Thai adults with impaired glucose tolerance are effective. The incidence of diabetes at the end of the study was significantly lower in the intervention group than in the control group. The lifestyle changes and consequent reduction in body weight led to the improvement of glycemic status and even reversion to normal glucose levels. After 2 years, the intervention prevented 28% of individuals at high risk from developing diabetes.
The incidence rate of diabetes in the cohort after the 2-year program in the control and intervention group were 16.6 and 12.1 per 100 person-year, respectively. This incidence is relatively similar to figures reported in India 18 (18.3% per year) and in a Chinese cohort, 19 but much higher than figures reported in studies conducted in Finland 6 and the United States. 8 The higher incidence may be due to a lower threshold for risk of diabetes in Asian populations. 20 Factors influencing the effectiveness of the intervention include contents and intensity of the program. Our program included topics such as diet modification and increased physical activity, which appear to be the norm for diabetes prevention; however, we used group activities as a bottom-up process rather than a top-down approach to promote participation, as a result, for example, choices of food intake and types of physical activity used were conformed to the culture of the community.
Weight reduction in the present study was, on average, 1.5 kg in the intervention group whereas, increase 0.4 kg in the control group. This reduction is smaller than reported in European 6 and American 8 cohorts, perhaps because of the lower baseline weight (mean BMI: 31-33 kg/m2) and the lower proportion of obese subjects (mean BMI: 27 kg/m2) in our study, although the BMI in our cohort was slightly higher than BMI in the Indian 18 and Chinese 19 studies. Systematic reviews have so far noted that in real-world settings, weight reduction varies and is lower than in intensive-efficacy clinical trials. 10 A meta-analysis by Cardona-Morrell and colleagues calculated an average weight loss of 1.6 kg after 12 months, higher than the weight loss in our study. 21 This may perhaps be attributable to the lower baseline body weight in the present study.
A high frequency of contact contributes to achieving weight loss outcomes, and programs with low participation rates tend to be less effective at reducing the incidence of diabetes, 3 but even smaller reductions in weight can result in a lower incidence. Factors other than weight loss may also contribute to a lower incidence.18,22 Compared with other studies, the present study found a high rate of conversion to diabetes. The effect size (relative reduction) of 28% of diabetes prevented was smaller than effect sizes reported in cohorts in Finland (58%), the United States (58%), China (42%), and India (38%).6,8,18,19 The length of the intervention and rates of compliance may account for the differences, as well as genetic profiles. The difference in incidence between groups became less pronounce in the second year might be due to the lower intensity of the program in term of frequency and length of each meeting. However, this has to trade-off with the participation rate as the more frequent of meeting might lead to lower availability to participate as already reflected by the rate of lost to follow-up. However, one of the benefits of the program, other than the outcome indicators, is the learning process of assisting individuals at high risk of diabetes. The local teams expressed that they acquired knowledge and practices to improve the quality of diabetes screening and prevention in the community. The multi-professional research group from 8 provinces had opportunities to share their experiences and support and learn from each other, resulting in better work performance and strengthening the diabetes care network. Apart from the knowledge gained and experience-sharing, support from others is spiritually beneficial and valuable.
The implication of the present study is that the findings seem to be applicable to wide population in Thailand since we included samples from all regions and probably to other communities in Asian populations with similar culture context. The results of the study were presented to the National Health Security Office Board, and the program guidelines have been adopted and distributed to primary-care practices throughout Thailand.
The present study had some limitations. There are high numbers of participants who were lost to follow-up, which might bias the results; however, the characteristic of those who were missing were relatively similar to those with completed the follow-up so that the estimations were barely affected. The high percentage of individuals lost to follow-up also reflects feasibility in real world as some participants had to go to their daily work and we did not pay monetary incentive to participate. We did not measure some of the process indicators, such as changes in dietary intake. The sample did not include populations in urban areas such as Bangkok, so it may not be generalizable on a country-wide level. We cannot compare differences by region because of the small sample. The participants were not individually randomized because of the community approach; however, selection bias is not likely as both groups had similar characteristics. The study’s strength, however, is the relatively large multiregion samples, and findings may be applicable in similar low- to middle-income countries. Using clustered randomized trial with high number of clusters in the present study provided sufficient power. 13
In conclusion, the present cluster randomized controlled trial of diabetes prevention in primary care settings demonstrates that lifestyle intervention can significantly prevent or delay the incidence of diabetes in Thai populations with impaired glucose tolerance. The identification of individuals at risk and participatory group activities plays a role in the effectiveness of lifestyle modifications.
Footnotes
Acknowledgements
We sincerely thank the participating Thai Diabetes Prevention Team: Nakhon Ratchasima City Municipality: Wilarwan Sripho; Thasala Hospital: Tuanjai Burapasiriwat; Buddhachinaraj Hospital: Rachada Pipatsart, Premsuree Sansom; Samutsakhon Hospital: Pongpat Chawarokorn; That Phanom Crown Prince Hospital: Anek Thanonghan, Watchira Lakhamkaew; Pakplee Hospital: Aungsumalin Mungkung Rungnapa Boonkean; Phrae Hospital: Chanidsa Chantapoon, Mayure Kungsri; Wang Wiset Hospital: Kasetsak Luanseng, Kornsinun Chaiyajit
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a BRIDGES grant from the International Diabetes Federation. BRIDGES, an International Diabetes Federation project, is supported by an educational grant from Lilly Diabetes. This project has also received the support of the National Health Security Office of Thailand, Walailak University, Mahidol University, and the Foundation for the Development of Diabetes Care.