
Abstract
Keywords
Introduction
Clinical practice guidelines (CPGs) in medicine are best-practice recommendations supported by systematic review of evidence to provide optimal patient outcomes.1-3 Currently, for primary care physicians in the United States, these CPGs encompass activities as diverse as assessing tobacco use, ordering eye exams for patients with diabetes, and assessing adherence to medication for individuals with depression. 4 Adherence to CPGs can reduce unnecessary services and improve patient satisfaction and outcomes. 5 It is surprising, then, to find that adoption of CPGs is poor throughout primary care services in the United States, hovering around 42%. 6 Causes of poor adoption of CPGs are multifactorial, but explanations have been proposed, which include various organizational, psychological, and behavioral theories.7-9
The most successful strategies to improve guideline adherence encourage physicians to be involved in implementation6,10,11 and use multifaceted approaches—such as continuing medical education with simulation exercises, practice coaching, electronic reminder systems, and computerized decision support.6,11 Furthermore, implementation strategies are more successful when they can be instituted over long time frames, (ie, several years), which helps assure consistent adoption, working through each aspect of CPGs by involving the entire patient care team, and using Plan–Do–Study/Check–Act methods for continuous quality improvement.10,12,13
One significant barrier to guideline implementation is the tremendous number of CPGs (more than 200) that primary care practices are expected to implement, which can overwhelm those trying to make improvements one at a time. 12 Additionally, lack of physician training in topics related to successful system change and implementation has been identified as a barrier to CPG adherence. To facilitate implementation of multiple quality measures, it is natural that the numerous guidelines would be grouped together. It is important to understand why office managers and physicians choose to group CPGs together and why they find grouping beneficial for multiple CPG implementation. These findings would enable the development of an implementation framework that could lead to improved patient outcomes. The purpose of this study, then, is to identify perspectives and priorities of office managers and physicians for grouping and implementation of CPGs.
More than 200 primary care CPGs are proposed by the Centers for Medicare and Medicaid services and the National Committee for Quality Assurance14,15 and have potential for significant public health impacts. However, neglecting to study the phenomenon of implementation of multiple CPGs will prevent realization of CPG adherence benefits. 16 Nonadherence to CPGs is now included in the definition of medical error and identified as the third leading cause of death in the United States, bringing ever more urgency to strive for feasible solutions to the problem of multiple CPG implementation. 17
Methods
Design
A qualitative study design was employed to identify the perspectives and priorities of physicians and their office managers for implementation of multiple clinical practice guidelines. A total of 6 physicians and 7 office managers (2 of whom were also registered nurses) represented 6 separate practices in the safety net of Fort Wayne, Indiana. Specific perspectives and priorities of office managers and physicians were obtained using a semistructured interview guide—asking about personal experiences in CPG implementation, including organizational strengths and weaknesses that contribute to implementation, combined with an open card-sorting exercise (Figures 1 and 2).
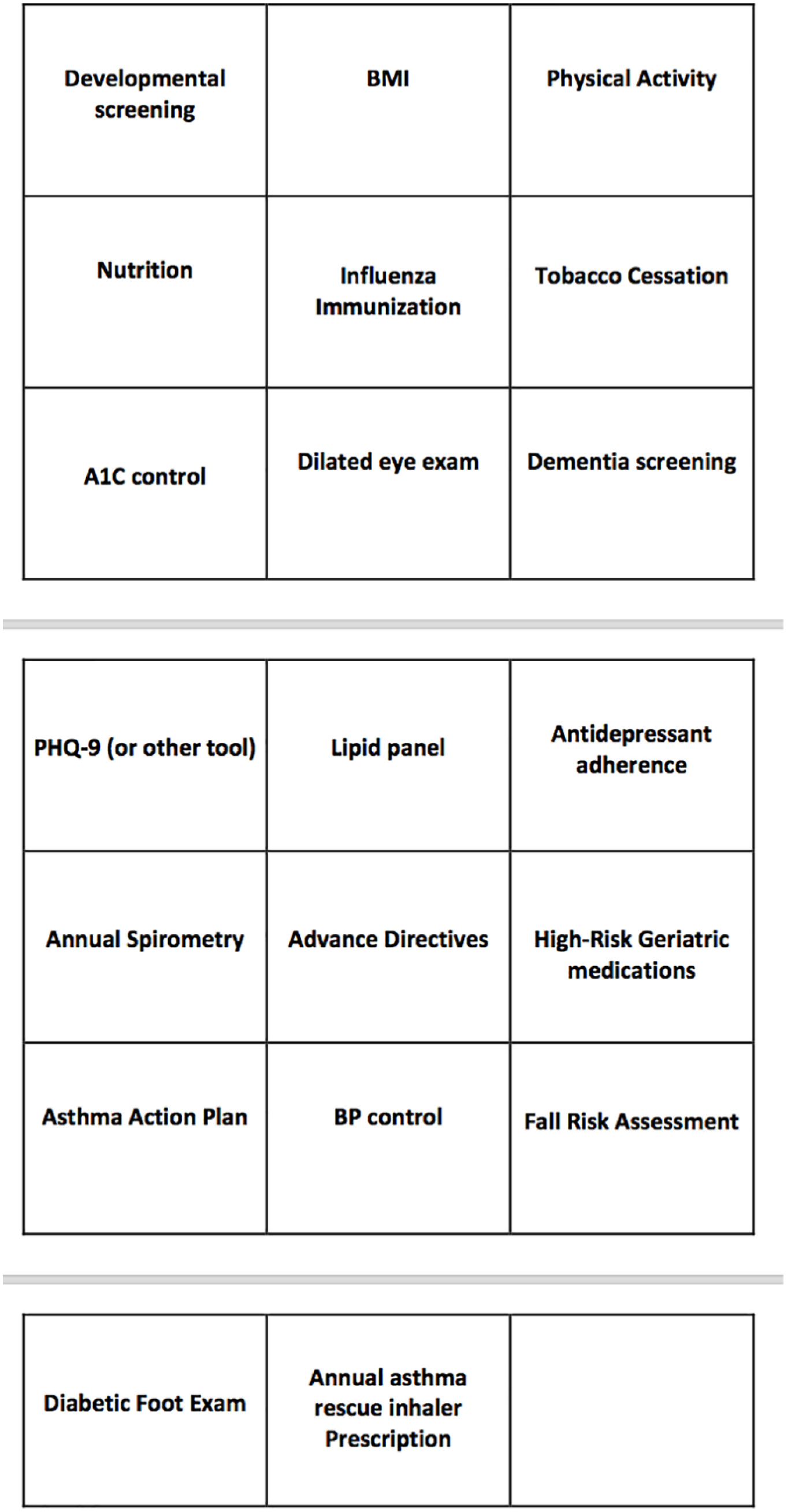
Cards used in card-sort exercise.

Interview schedule.
Setting
Fort Wayne, Indiana, is located in the Midwestern region of the United States. It is the second largest city in Indiana with a population of 260 000. 18 Nineteen percent of the county lives below the poverty line, and the safety net encompassing these urban poverty areas,18,19 were the primary settings for recruitment of participants.
Participants, Criteria, and Recruitment
The inclusion criteria for this study were family medicine physicians practicing at least half-time and in low-income zip codes, full-time office managers involved in creating office workflows who were associated with participating physicians. Exclusion criteria were physicians without at least 2 days a week directly caring for patients, not in safety net zip codes, or with less than 1 year of practice experience. Office managers with less than 2 years’ experience overall in office administration, or less than 6 months in a current position were also excluded. Family medicine physicians and their office managers were sent a letter of invitation. The letter was followed with a phone call to answer questions, ascertain willingness to participate in the study, and schedule an interview time at each participant’s convenience. Snowball sampling was used to obtain recommendations for additional participants after nine interviews were completed. The first physician and office manager interviewed were used to pilot the interview questions’ face and content validity. 20 Since no changes were made after the pilot, these interviews were included in the final analysis. The number of interviews anticipated to identify and saturate themes based on a narrow focus of investigation could reasonably be found between 6 and 50.21,22
After informed consent was obtained, the interviews were audio-recorded and transcribed by the research team. In addition to the transcriptions, field notes were taken to provide context to the interviews, record the groups created in the card sorting exercise, and record the interviewer’s thoughts as the interviews progressed. Card sorting has been used in prior studies as a visual aid to facilitate depth and specificity in the interview responses. 23 Participants were asked to describe prior CPG implementation experience, detailing specific workflows and job duties. Participants were then asked to sort 20 CPGs into groups where all items in a group could be implemented simultaneously. Using the examples from the card sort, participants were able to explain why they had grouped individual CPGs together and how implementation had worked in their experience. The card sort was used during the interview to bring specificity to the conversation about clinical practice guidelines, roles of care team members, and detailed descriptions of experiences or expectations in implementation. Participants were then asked to identify organizational strengths and weaknesses influencing implementation. Finally, the groupings were prioritized for implementation, with participants describing their reasoning.
Thematic Content Analysis
After the interviews were completed and transcribed by the researcher, thematic content analysis was applied to the transcripts and notes including the open card-sorting visual aid portion of the interview. An iterative assessment of themes was performed, allowing comparison in perspectives and priorities between office managers and physicians. 24 The first 3 transcripts were coded, then re-examined multiple times and common themes and meta-themes recorded. The transcripts were then coded updating the theme template as additional transcripts were coded until a common set of themes and meta themes was created. When no new themes emerged, saturation was achieved, and the results were finalized.
Reflexivity, Credibility, and Trustworthiness
Reflexivity was used to continuously evaluate the researcher’s assumptions and create self-awareness of the biases being introduced into the interview process. 25 Researcher bias was mitigated through member checking and independent peer coding of one physician and one office manager interview transcripts. 26
Credibility in thematic analysis was reinforced through the constant comparative method, 27 arriving at stability of the findings. 25 Trustworthiness in the research process was reinforced with member checking, sending finished transcripts to participants to check for errors in intended meaning, through placement of quotations and emphasis.21,27 Triangulation was used between interview questions and card sorting and between themes resulting from both office manager and physician responses, along with thick description of participant responses in the findings allow the reader to judge the transferability and confirmability of the findings.28,29
Results
Characteristics of the respondents are listed in Figure 3. The interviews were conducted in each participant’s office and each interview lasted an average of 45 minutes, ranging from 21 to 68 minutes for a total of 9 hours and 13 minutes.

Characteristics of respondents.
Card-Sort Exercise
Participants grouped guidelines into preventive care exams, wellness services, and disease-based care (Table 1). Themes arising from this exercise showed that the standardized visit was important in CPG grouping for both physicians and office managers. Nearly all the respondents noted that annual geriatric wellness visits were an efficient way to accomplish multiple CPGs. Additionally, standard preventive visits for well-child exams and adult physical exams were also important.
Card-Sort Exercise.

Abbreviations: EMR, electronic medical record; OM, office manager; P, physician; WCC, well-child care.
Disease-based card groupings were also efficient ways of grouping related clinical guidelines, and most providers indicated they had a mental checklist to follow that included the CPGs in the card-sort exercise. However, only two providers noted they had written standing orders to accompany their mental checklist. A few had developed electronic medical record (EMR) disease-based templates, but those were only used by physicians and not something that staff members could see. Office staff could not access the disease-based EMR templates so there was little delegation to the rest of the clinic team to assist with CPG adherence.
Standardized rooming procedures, EMR templates, and discharge processes within the clinic were also a focus using standard appointment types. In addition, patient health questionnaires were used to address multiple CPG’s, especially during preventive care visits.
Standard office processes were not reflected in the card-sort groupings. One office manager, after a lengthy commentary about implementation strategies using standard office processes, paradoxically grouped all the cards based on disease: Is that . . . how you go about implementing guidelines? It seems a little different than what you described earlier. (Interviewer) Right. And it is. It seems it’s just that with these groups, that’s how automatically my mind wanted to put them in those disease processes. …Now whenever we’re implementing things in the office, it’s… we don’t do anything disease-based like this. (OM 3)
Meta-themes
Thematic analysis was applied as described above to the interview transcripts, revealing four meta-themes:
Delegation of supporting tasks within the office
Personalization of CPGs for patient benefit
Interoffice workflow triggers and CPG reporting
Change management for CPG implementation
Delegation
Delegation of supporting tasks within the office was reported by both physicians and office managers as playing a key role in implementing multiple clinical practice guidelines (Tables 2 and 3). The increased amount of work that was generated by the CPGs mandated that the tasks be shared between the staff and physicians.
Meta-theme: Delegation.

Abbreviations: CPG, clinical practice guideline; OM, office manager; P, physician.
Examples of Delegated Activity.

Abbreviations: CPG, clinical practice guideline; OM, office manager; P, physician; POCT, point-of-care testing.
Communication was described as essential to delegation. Written instructions with clear expectations empowered clinical staff to help accomplish CPG adherence. CPGs that had been personalized for the particular patient were more likely to fall back on the physician to accomplish. At times, physicians perceived delegated CPGs as more likely to be done too often or too aggressively. Physicians expressed unwillingness to risk unnecessary expense for the patient or potential harm from overtreatment.
Physicians relied on shared responsibility of other clinical staff to accomplish CPG adherence, yet some physicians felt that since ultimate responsibility rested on them, the physician should be responsible for doing the tasks.
. . . When you delegate you just can’t trust as much [the clinical practice guidelines are] going to get done, because they don’t care as much. It doesn’t reflect on them. (Phys 1)
Some tasks were more consistently delegated: clerical tasks, insurance coverage appeals (eg, prior authorizations), distributing screening questionnaires, converting return appointments into wellness visits, obtaining vital signs, ordering referrals to in-house services, and reinforcing patient education. Tasks less likely to be delegated included point of care testing, labs, procedures, referrals, and routinely adding preventive services to a prescheduled visit. Tasks such as manual data entry and manual information retrieval from other hospital systems raised concern of introducing error. These concerns about error were mitigated by scanning documents into the chart, duplicating manually entered results, creating waste and further restricting staff time that could otherwise be used for patient care.
Physicians cited lack of training in some subjects as limiting their ability to provide robust patient education: In medical school our training in nutrition was we had lunch at the . . . hospital one day and they told us how many calories we ate. That was it. No diabetic training, nothing. (Phys 5)
Finally, both office managers and physicians felt that the number of CPGs was overwhelming.
. . . and that’s why I think the burnout rate is so high because all of these things are great. But it just kills us sometimes. (Phys 1) . . . I’ll jump in and help when I can, when I have a minute and everything, but it is . . . it’s just so much. (OM 5)
Triggers and Reporting
Delegation of CPGs was dependent on triggers enabling staff to recognize that certain CPGs applied to the visit (Table 4). For example, the appointment scheduler needed to know when a patient was due for an annual wellness visit, so the visit could be scheduled appropriately, and the health questionnaire(s) mailed out to the patient prior to the appointment.
Meta-theme: Triggers and Reporting.P – Physician, OM – Office Manager.

Abbreviations: EMR, electronic medical record; OM, office manager; P, physician.
Since CPG adherence gaps were not accessible to the appointment schedulers, some clinics had the office nurse review the appointments a day or two ahead of time and call the patients again to let them know if they had any labs or questionnaires that needed to be done prior to the visit. This duplication of work indicated a lack of universally visible triggers, especially disease-based triggers, for seamless distribution of duties among all the clinical staff.
“Care Gaps” and “Health Maintenance” triggers were present in some EMRs and did help the clinical staff divide up the work to accomplish more items in the patient visit. Yet for both physicians and office managers, there often seemed to be just too much to cover in a visit. Patients were able to accomplish some CPGs, like filling out the questionnaire for the annual wellness visit prior to the visit, but even then, there was no easy way to enter the information back into the electronic record, so the time saved was lost by reentering the data.
Standing orders allowed clinical staff to help address CPGs. Three physicians had developed written instructions detailed enough for the clinical staff to implement. Other clinical staff accumulated knowledge of verbal instructions and eventually became adept at predicting what the physician might want. The office managers and clinical staff expressed a desire to have written instructions as much as possible. Physicians, however, often ended up feeling that they would like to see the patient first and then verbally direct the assistant with the orders to maximize efficiency.
Patient-Centeredness
Patient-centeredness for respondents included tailoring CPG target goal, rate, and priority in adherence (Table 5). Office managers wanted to present options for patients to choose a preferred method of compliance. For physicians, emphasis on patient-centeredness involved considering patient preference, shared decision making, and availability of patient resources.
Meta-theme: Patient-Centeredness.

Abbreviations: OM, office manager; P, physician; PE, physical exam.
Barriers to care such as transportation, cost of compliance, access to needed services, and food insecurity were factors that physicians mentioned that they wanted to address in CPG adherence. The number of changes that needed to be made at a single visit was perceived to degrade the quality of the office visit and overwhelm the patient, turning the visit into a “checklist” for the physician and patient interaction.
And then you can miss you know, a tear in their eye, or something like that but you’re bogged down with everything else—you missed some of that. And they feel the coldness, feel they have been talked at as opposed to being talked to. (Phys 1)
Physicians and office managers were in agreement that CPG adherence had to be meaningful and clinically relevant to the patient.
They signed a contract that says we do all those things within the first six months of the year, which means you might do one in December and then have a patient coming in January and do the same thing again. So that’s an example to me of treating statistics instead of patients. (Phys 5)
Change Management
Repeatedly, physicians and office managers discussed change management principles in the context of both CPG grouping and implementation (Table 6). Communication was seen as a key to meaningful change. Both broad input as well as universal consensus were seen as critical aspects of change management:
And one thing that has been very helpful for me is understanding that even though I’ve sat down and looked at something six ways from Sunday in my mind, when I come to present it to somebody it’s going to be their first time. (Phys 4)
Meta-theme: Change Management.

Abbreviations: CPG, clinical practice guideline; EMR, electronic medical record; OM, office manager; P, physician; WCC, well-child care.
Physicians pointed out that real adherence was a very lengthy process: I don’t think [CPGs] are difficult, I think they just take time, and you just can’t expect everyone in the clinic to be at the same level as you. So obviously the clinical staff they need a little bit more education since they don’t know the background of everything . . . But I realized . . . if we explained to them why things were the way they are, they were more . . . they understood it . . . (Phys 6)
The ability for the staff and physicians to influence the CPG implementation protocol was perceived as very important.
Actually, from the manager perspective I would take all 20 of these [CPGs] and let them decide. Because honestly that’s the best way you’re going to get things to go through. . . . You know, getting ideas from the people who are actually going to be doing it is setting yourself up for success. (OM 3)
For patient adherence as well, change management was seen as an essential factor. Helping the patient understand why a behavior needed to change, or a medication needed to be prescribed was the first step in adherence. Trust in the physician, with authenticity in the patient relationship was perceived as critical in affecting healthy behavior and acceptance of the CPGs.
Simplicity and continuous optimization benefitted concomitant implementation of CPGs. Simple CPG’s or simple CPG implementation mechanisms promoted adherence in CPGs requiring substantive patient behavior changes. It was important to have a well-thought out plan prior to implementation to avoid rework but also to be able to continuously improve the workflow over time.
Discussion
Card-Sort Exercise
Participants arranged groups in the card sort by standard visit type, standard office roles, and disease process. In an article detailing a highly successful, CPG-adherent practice, standardization of office processes was key to teamwork development. 30 After standard visit type, cards were nearly universally grouped by disease process, although this grouping provided less opportunity to delegate items because disease-based workflows and triggers were underdeveloped compared with those for standardized visits. This finding was unexpected, as literature on organizations and workflows reinforce the benefit of delegating items to clinical staff within the office.31,32
Grouping cards by disease process reflected the influence of medicalization on office workflows. Even for the most highly workflow-attuned office manager, CPGs were sorted by disease-state and not by office workflow. The card sort exercise identified a predisposition by the participants to take a medical view of workflows, which may be compounding the difficulties in developing and implementing new clinical processes to address CPGs. The danger with medicalization of implementation, is that implementation strategies involve team-based care and standard workflows, while disease-triggered decision making leads to the physician initiating all of the CPG adherence tasks. Unconsciously reverting to a medical frame of reference when developing medical office workflows may contribute to difficulties in implementation. 33
Delegation of Supporting Tasks Within the Office
Delegation of supporting tasks was recognized as an important component of CPG adherence and workflow efficiency. Research on lean process in particular calls for efficient team-based care. 34 The presence of a high-functioning team in health care was encouraged and described by the Institute of Medicine as an important asset in CPG adherence. 35 In this study, most participants described partial delegation of CPG tasks to clinical staff.
Patient-Centeredness
Patient-centered application of CPGs remained important throughout the study but at the expense of delegation and efficiency that came from standardization. Physicians described examples of inflexible CPGs causing harm to patients, so personalization was perceived as essential for positive patient outcomes. In contrast, studies on workflow and CPG adherence demonstrate that variation threatens consistency and efficiency.30,34,36 In medical care, patient-centeredness and shared decision-making are key principles for CPG adherence, accommodating patient priorities and resources.9,36,37 CPG personalization needs be communicated effectively across all office functions to maintain the benefits of delegation and efficiency. 32
Triggers and Reporting
Standardized communication of triggers for CPG adherence were important, but often lacking. 38 Disease-based EMR triggers were not communicated to the front desk. Communicating CPG triggers allows implementation at the most logical locations in the office for the workflow to take place. Written standing orders and triggers promote consistent and efficient CPG implementation,1,39 yet few practices had them.
Change Management
Change management was identified by participants as essential to CPG implementation. Genuine adherence was felt by providers to be often neither simple nor rapid, and that the CPGs with value-based contracts did not represent the timeline for authentic patient behavior change necessary to reap the benefit of CPG adherence. Supportive relationships between practice administration, physicians and office managers were seen as essential to successful change management and CPG implementation. Respondents cited early and frequent communication along with the ability to influence proposed changes, as critical for efficient and effective implementation. Communication and small group dynamics are supported by Kotter’s book on change management, as well as the Institute of Medicine report on high-functioning teams. 35
Limitations
No studies were identified that specifically examined the strategy of grouping CPGs for implementation. However, qualitative studies examined facilitators and barriers involved with implementation of multiple clinical guidelines in primary care.40,41 In other examples, CPG adherence was studied as a part of greater practice transformation initiatives, like the patient-centered medical home. 38 None of these studies, however, specifically examined factors related to grouping of multiple CPGs for simultaneous implementation. This study had a limited number of participants and was conducted limited geographic area.
Conclusion
In conclusion, this qualitative study describes the perspectives and priorities of physicians and their office managers when grouping and implementing multiple CPGs. In the open card-sort exercise, participants grouped guidelines into three main categories: standardized preventive care exams, wellness services and disease-based care. Most physicians indicated they followed a mental checklist to accomplish the CPGs in each category and did not have written protocols. For office managers, verbal or written standing orders were important in allowing clinical staff to help address CPGs. CPG adherence was also facilitated by implementing standardized processes, such as standard appointment types, standard rooming procedures, standard EMR templates, and standard discharge processes. Importantly, the identification that an office workflow created based on medical familiarity won’t be easily adopted since actual office workflow elements are not considered.
Delegation of activities within the office was a priority for both physicians and office managers in implementing multiple CPGs. Physicians relied on shared responsibility with other clinical staff to accomplish CPG adherence, yet some tasks were more easily delegated than others. Clear communication facilitated delegation with triggers that enabled staff to recognize when CPG protocols applied to the patient visit. CPG triggers were not visible to the appointment schedulers or front desk staff in most offices so clinical staff performed a manual review of the schedule a day prior to the appointment. Office manager perspectives reflected concerns of inefficiency and waste through the duplication of work. In some EMRs, “Care Gaps” and “Health Maintenance” triggers were present and helped distribute the work of CPG adherence during the patient visit.
Both physicians and office managers prioritized reporting CPG adherence to provide positive reinforcement. Population management presented in aggregate as a “Dashboard” or as specific indicators like wellness visit rates encouraged further CPG adherence. Office manager perspectives reflected concern that resource limitations requiring manual data entry and manual retrieval of information from other hospital systems introduced error or requiring duplication of work by also scanning resulted questionnaires into the chart. Physician perspectives showed that lack of training in critical subjects limited their ability to provide robust patient education such as nutrition.
Patient-centered CPG application was a priority for physician and office managers in accommodating patient preference, using shared decision making, considering patient resources, and modifying target goals, and rate of adherence, to best promote patient adherence. Priority was also given to addressing barriers to care such as transportation, cost of compliance, access to needed services and food insecurity. Physicians and office managers were in agreement that CPG adherence had to be meaningful and clinically relevant to the patient. Repeatedly, physicians and office managers discussed change management principles in the context of both CPG adherence and grouping. The ability for the staff and physicians to influence the CPG implementation protocol was perceived as very important.
Implementation priorities for physicians and office managers involved grouping CPGs more by disease state more than workflow, reflecting medicalization of CPG implementation. Even those office managers well-trained in leveraging office processes and change management for CPG implementation continued to group CPGs by disease process. While beneficial in recognizing the circumstance for applying a CPG, disease-based grouping was ineffective in producing the triggers and communication necessary for seamless team-based delegation. Medicalization of CPG implementation should be addressed with further research into mechanisms translating disease-based triggers into office processes to improve CPG implementation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.