
Abstract
Objective
To explore the perceived feasibility and potential applications of an augmented reality (AR) solution to address the challenges of managing pressure injuries in non-clinical settings.
Methods
This qualitative study utilized semi-structured interviews with caregivers and healthcare professionals. Conducted from January to June 2025 at Guangdong Provincial Hospital of Chinese Medicine, the study recruited 21 participants via purposive and snowball sampling until data saturation. Interview guides were grounded in the technology acceptance model. Data were analyzed using Braun and Clarke’s six-phase thematic analysis via NVivo.
Results
Most participants (90.5%) reported prior experience with general digital health technologies such as telehealth platforms, while few had used immersive technologies (23.8%). All healthcare professionals were currently involved in pressure injury care (100.0%), and most caregivers were providing current care (83.3%), with the remaining caregivers reporting recent and relevant caregiving experience (16.7%). Thematic analysis revealed that participants’ perceptions of the AR application were shaped by three main themes: perceived usefulness, perceived ease of use, and intention to use. Key external variables, such as computer anxiety and computer efficacy, also influenced these perceptions.
Conclusion
This study indicates that both healthcare professionals and caregivers perceive AR as a potentially useful tool for remote pressure injury management. Successful implementation depends on addressing key concerns related to user interface design, cost, and data privacy. These insights indicate that future development must prioritize intuitive usability and robust privacy measures to ensure successful implementation.
Introduction
Pressure injuries, also known as pressure ulcers, impact an estimated 6.5 million people worldwide each year, 1 leading to a heavy healthcare burden. The annual cost of treating and managing pressure injuries in the United States reaches $26.8 billion, affecting approximately 3 million adults,2,3 which corresponds to an estimated average cost of approximately $8930 per case annually. Pressure injuries are common in geriatric populations, individuals with impaired mobility, and patients exhibiting severely compromised health.4,5 Untimely recognition and inadequate treatment can result in pain, infection, decreased quality of life, and death.6,7 Pressure ulcers are highly prevalent not only in hospitals but also in long-term care facilities and community-dwelling environments, particularly among patients receiving care at home. 8 Approximately 25% to 35% of pressure ulcer patients receive care at home, where limited specialized oversight contributes to higher rates of complications and delayed wound healing. 9
For individuals with pressure injuries in long-term care and home-based community environments, timely access to specialized wound care remains a significant challenge, directly contributing to delayed healing and increased complications.10,11 In addition, their caregivers are typically non-specialized personnel or untrained family members, who are often overwhelmed by the complex tasks of wound assessment, dressing changes, and infection monitoring. 12 These challenges expose existing gaps in healthcare delivery, indicating the necessity and potential of remote management tools. 13
Current remote management tools for pressure ulcers mainly include mobile health applications and telehealth platforms. These applications typically provide educational resources and reminders for dressing changes. 14 Telehealth platforms involve web-based interfaces or mobile applications that allow caregivers to capture images of pressure injury. 15 However, mobile phone photos or videos often fail to provide accurate wound dimensions and classifications, potentially hindering clinical decision-making. 16
In response to these limitations, augmented reality (AR) has recently been viewed as a technology with considerable potential for telehealth applications. 17 Unlike virtual reality (VR), which immerses users in a fully computer-generated environment, AR overlays digital information onto the real-world environment, allowing users to remain aware of and interact with their physical surroundings. 18 As noted by Klinker et al., 19 unlike smartphones that disrupt clinical workflows by requiring manual input, AR smart glasses allow professionals to document procedures and access information without disengaging their hands from patient care. Building on this utility, recent research has begun to explore the implementation of AR in home-based settings. Schneider et al. evaluated a mixed-reality system for professional home care, identifying wound care as a primary use case where hands-free interaction and smooth service handovers provided significant benefits. 20 Despite advancements in remote wound support, there is a lack of empirical research on its feasibility for precise pressure injury assessment by informal caregivers in home settings.
This qualitative study aims to explore the perceptions and experiences of both informal caregivers and healthcare professionals regarding the application of AR in remote pressure injury assessment. Through in-depth interviews, this research seeks to understand the perceived benefits, challenges, and practical preferences of integrating AR technology into current practices. The findings will provide crucial insights into the feasibility and acceptability of AR-based solutions from the perspective of end-users, thereby informing the development of more effective, user-centered remote management tools to improve pressure injury outcomes.
Methods
Study design
This study employed a qualitative descriptive design using thematic analysis to explore perceptions, feasibility, and perceived challenges associated with applying AR technology for pressure injury assessment, guided by the technology acceptance model (TAM). 21 The reporting of this qualitative study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines, 22 and the completed checklist is provided in Supplemental material 1. The study was conducted between January and June 2025 and was coordinated by the Guangdong Provincial Hospital of Chinese Medicine, China. To ensure a broad and diverse perspective, participants were also recruited nationwide through online social media communities, including WeChat and RedNote.
Sample and recruitment
This study aimed to understand the multi-faceted perspectives on the application of AR for remote pressure injury assessment. Two target population groups were identified: informal caregivers of individuals with pressure injuries and healthcare professionals with experience in pressure injuries care. In the context of this study, informal caregivers refer to family members or relatives providing unpaid care in home-based community settings. In China, the responsibility for long-term wound care often shifts from the hospital to the family unit within the local community residential environment, where professional home-nursing resources may be limited. The inclusion criteria for informal caregivers included: (1) aged 18 years or older; (2) currently providing direct care to an individual diagnosed with a pressure injury in home or community settings; and (3) willing and able to participate in a Mandarin-speaking interview. Inclusion criteria for healthcare professionals included: licensed healthcare professionals, including (1) registered nurses, nurses practitioners, and physicians; (2) regularly involved in pressure injury assessment and management; and (3) willing and able to participate in a Mandarin-speaking interview. Students or individuals who are not actively practicing wound care were excluded.
Participants were selected using purposive sampling, supplemented by snowball sampling, to recruit informal caregivers and healthcare professionals with experience in pressure injury care. Given that many families in China manage pressure injuries independently at home due to cultural preferences for family-centered care, these informal caregivers often remain outside formal clinical circles. Snowball sampling was therefore essential to access a more diverse and representative sample of this lay population. Recruitment was conducted through posters and e-recruitment materials distributed in hospitals and clinics. Participants were primarily recruited from the Departments of Geriatrics and Orthopedics, as well as wound and ostomy clinics. To ensure a diverse sample, additional cases were recruited via social media platforms, specifically WeChat and RedNote. Healthcare professionals were additionally recruited through departmental outreach, with clinical leaders assisting in disseminating study information to eligible staff. Interested individuals contacted the research team via telephone or online messaging platforms and underwent eligibility screening. A total of 24 individuals expressed interest, of whom 21 completed interviews. Three individuals declined participation due to scheduling conflicts or time constraints.
The decision to cease recruitment was guided by the principle of data saturation. Interviews continued until no new themes or insights emerged during the interviews and preliminary analysis.23,24 Data saturation was achieved after 21 interviews. Demographic information for the study participants is presented in Table 1.
Basic characteristics of participants.

SD: standard deviation; N/A: “not applicable” for the respective participant group; AR: augmented reality; VR, virtual reality.
General digital health tools refers to non-immersive digital tools, such as telehealth platforms, video consultations, mobile health applications, or remote-monitoring systems.
Immersive technology (AR/VR) refers specifically to three-dimensional spatial computing devices, including head-mounted displays like Microsoft HoloLens, VR headsets, or mobile-based AR that utilizes spatial anchoring.
Development of the AR pressure ulcer application
The AR pressure ulcer application was deployed on head-mounted devices (Microsoft HoloLens 2, Microsoft Corporation, USA), which was developed to support remote pressure injury assessment and management. Core functions included (1) wound area measurement, (2) pressure injury classification, (3) hands-free documentation, and (4) consultation support. The device provided real-time holographic visual feedback; users could align the virtual interface with the wound area and interact with the system using gesture-based controls. The application enables visualization of wound dimensions using the device's built-in spatial sensing system, which previous studies have reported to achieve sub-centimeter spatial resolution under controlled conditions.25,26 Illustrations of the simulated assessment environment, classification feedback, pressure injury measurement, and hands-free documentation interfaces are presented in Figure 1.
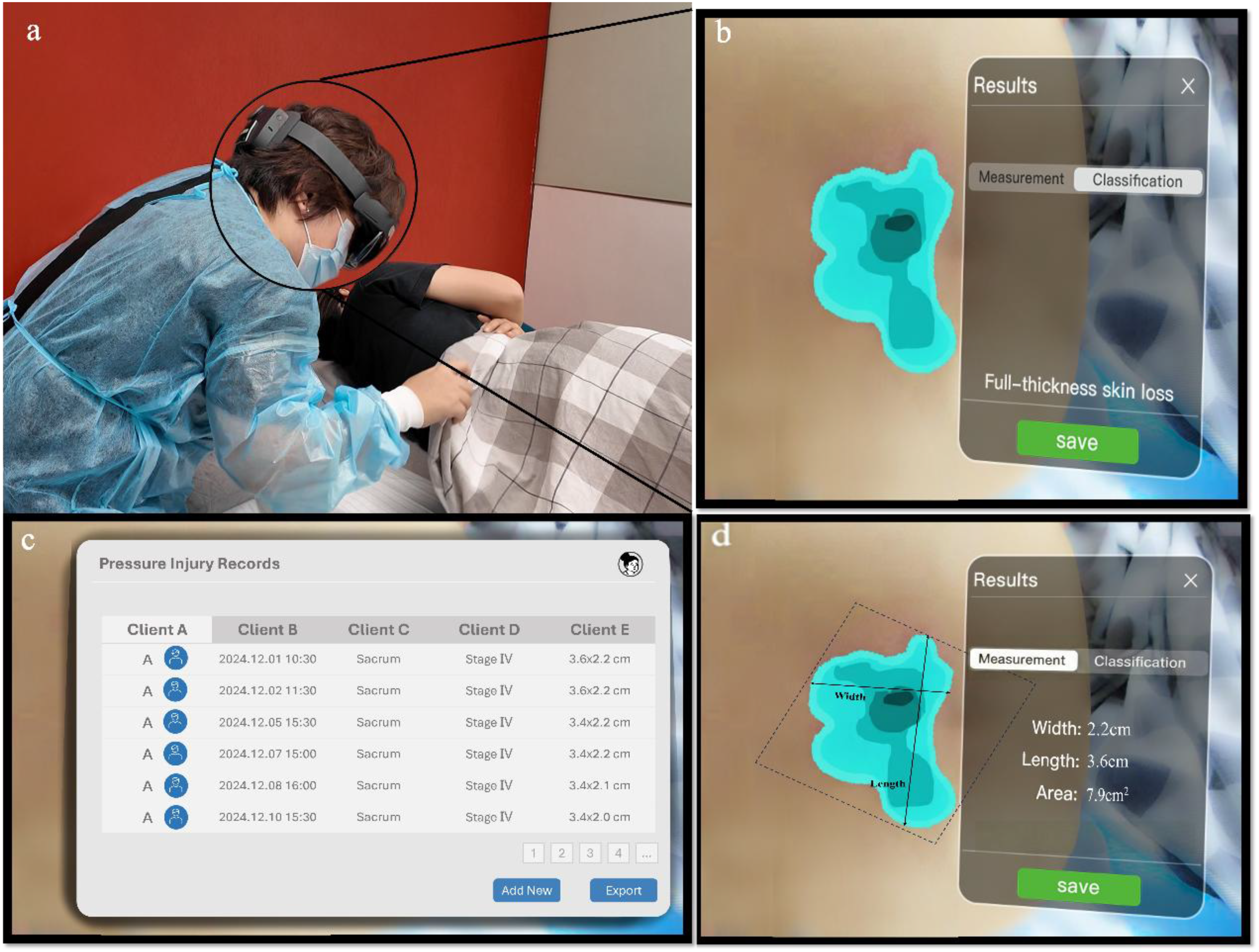
Application scenarios for HoloLens-based AR pressure ulcer application: (a) simulated assessment environment; (b) first-person view of real-time classification feedback; (c) documentation interface illustrating hands-free recording and data management; (d) first-person view of real-time measurement feedback. AR: augmented reality.
Data collection
Data was collected through semi-structured individual interviews. Semi-structured interviews allowed for in-depth exploration of the emerging theme. To ensure a common understanding of the AR system during interviews, a standardized demonstration was conducted via screen sharing prior to each interview. The demonstration followed a narrated walkthrough illustrating how the AR head-mounted device visualizes pressure injury areas, performs real-time measurement, and enables documentation of assessment results. Participants were encouraged to ask questions throughout the demonstration, which continued until participants confirmed adequate understanding of the system functions.
Semi-structured interview guides were developed based on the TAM, 27 and were adapted separately for caregivers and healthcare professionals to reflect their different roles and contexts. The interview guides are provided in Supplemental material 2. Key thematic areas of the interview guides included Perceived Usefulness, Perceived Ease of Use, and Intention to Use. Both guides were pilot-tested with two informal caregivers and two healthcare professionals who met the inclusion criteria but were not part of the main study sample. Minor adjustments were made to ensure clarity and comprehensiveness.
All data were collected through online video interviews conducted via secure conferencing platforms to accommodate participants located across different regions. No non-participants were present during the interviews. Interviews were conducted once per participant; repeat interviews were not performed. Each interview lasted 15–45 min. All eligible individuals received detailed study information and provided written informed consent before the interview was scheduled.
Interviews were conducted by two female researchers (YH and JG). YH is a PhD candidate in public health, and JG holds a master's degree and was employed as a clinical nurse at the time of the study. Both interviewers had formal training in qualitative research methods and prior clinical experience in pressure ulcer care. The interviewers had no prior relationship with participants and were not involved in their clinical care, helping to maintain a neutral interviewing position. Before the interviews, participants were informed of the researchers’ professional backgrounds, their roles as researchers, and the study objective of improving remote pressure ulcer care through technology. Participants were aware that the researchers were conducting the study for academic research purposes and had professional interests in enhancing pressure ulcer management and patient care through technological approaches. To promote reflexivity and minimize potential bias, the researchers acknowledged that their clinical and research backgrounds might influence data interpretation. Field memos were documented immediately after each interview to capture non-verbal observations, and preliminary analytical reflections that might not be fully reflected in audio recordings. These memos were revisited throughout the data analysis process to ensure analytic rigor.
Analysis
Data analysis was conducted using a theory-driven thematic analysis approach. During the analysis process, the TAM theory provided the preliminary theoretical framework for the study. Following the completion of the coding process, a thematic map was developed to illustrate the integration of emergent, inductive sub-themes within the deductive TAM constructs. NVivo 14 software was used for data management, coding, and thematic organization.
The audio recordings were transcribed verbatim by YH. Interview transcripts were returned to participants, who were invited to verify the accuracy of transcription. Minor linguistic clarifications were received and incorporated into the dataset. Two researchers (YH and JG) independently coded the transcripts following Braun and Clarke's six-stage thematic analysis framework. 28 The analytic process involved: (1) familiarization with the data through repeated reading of transcripts; (2) generation of initial codes using a combination of deductive coding informed by TAM constructs and inductive coding to capture data-driven insights; (3) searching for candidate themes; and (4) reviewing, refining, and defining themes in relation to the research objectives. A shared codebook and coding tree were developed and iteratively refined during the coding process. Disagreements in coding and thematic interpretation were resolved through discussion and consensus between the two researchers. When consensus could not be reached, a third researcher (SL) reviewed the relevant transcripts, analytic memos, and original audio recordings to facilitate final agreement. Preliminary themes and interpretations were shared with participants via online communication platforms. Participants were invited to review the findings, and feedback confirmed the consistency of interpretations.
Ethical considerations
This study was approved by the Human Research Ethics Committee of City University of Hong Kong (approval number: HU-STA-00001179). Written informed consent was obtained from all participants prior to study participation. Participation was voluntary, and participants were informed of their right to withdraw at any time without consequence.
Results
As shown in Table 1, a total of 21 participants were included in the study, comprising nine healthcare professionals and 12 caregivers. The mean age of the participants was 49.6 ± 9.7 years. All participants met the study inclusion criteria at the time of recruitment. All nine healthcare professionals (100.0%) were currently involved in pressure injury care, 10 of the 12 informal caregivers (83.3%) were providing current care, with the remaining two participants having significant recent caregiving experience.
Additionally, a substantial majority of the total participants (90.5%, n = 19) had prior exposure to general digital health technologies, such as telehealth platforms, mobile health applications, or video-based consultations. And a minority had direct experience with immersive AR or VR technologies (n = 5, 23.8%). The average interview duration was 37 min.
The analysis identified sub-themes organized under the three main themes of the TAM: perceived usefulness, perceived ease of use, and intent to use. The relationship between these emergent sub-themes and the theoretical framework is summarized in the thematic framework depicted in Figure 2.

Analytic synthesis of themes and sub-themes derived from the thematic analysis, informed by the technology acceptance model.
Perceived usefulness
Based on the demonstration of the AR system, most participants perceived the AR tool for remote pressure injury assessment as potentially useful. Both caregivers and healthcare professionals articulated ways in which the demonstrated AR functions could potentially support current practices, particularly when compared with existing remote assessment methods. Four sub-themes emerged: enhanced monitoring and early detection, accuracy and reliability, improved communication and collaboration, and quick response.
Enhanced monitoring and early detection
Participants from both groups described the demonstrated functions as having the potential to support more consistent monitoring of pressure injuries and to assist in recognizing changes at an earlier stage. Caregivers emphasized that they often found it difficult to judge whether changes in a wound indicated deterioration, and perceived AR-based visualization as a possible way to reduce uncertainty. In the beginning, honestly, her skin was already red in that area, but we didn't care… the skin hardened and we still didn't care because we didn’t understand these things. Then it got worse and worse and now it's so rotten that you can see the flesh. (Caregiver 7)
Accuracy and reliability
Healthcare professionals and caregivers discussed the potential value of AR-assisted wound measurement and classification. Caregivers compared the AR system with prior experiences of video calls or photo-based consultations, noting difficulties in judging wound size and depth using existing methods: The downside (of the video) is that the pressure sore still needs to be seen in person, and the video can't be very clear on that. (Caregiver 8) I think one of the first pain points it solves is that doctors can better see what the wound really looks like, which should be better than video or photos. (Caregiver 3) Previously judging the size was not possible and required a measuring card … which is now skipped. (HP-B) Machines are not like humans, humans don’t measure wrong, machines sometimes go wrong, how can this problem be solved? (Caregiver 1)
Improved communication and collaboration
Participants perceived AR technology as a possible means of facilitating remote communication between caregivers and healthcare professionals, particularly for patients with limited mobility or those living in rural areas. Caregivers described practical difficulties in traveling to hospitals for in-person consultations: My brother is unable to move, so I went to the hospital to get a prescription from the doctors on his behalf. (Caregiver 7) We are in a rural area and it was more of a hassle to get to the hospital, so we had to manage it on our own. (Caregiver 6) It's actually a big trouble for the elderly to go to the hospital, especially those who have mobility problems. (Caregiver 4) The medical skills of doctors in community hospitals are not very reassuring, so we still prefer to go to specialists in large hospitals. (Caregiver 11)
Quick response
Participants highlighted the importance of timely access to professional guidance. Healthcare professionals acknowledged that caregivers often lacked direct contact channels, which limited opportunities for rapid consultation: There was no way for them to ask us in time because they didn’t have our private contact information, so they had to come to the hospital and ask us. (HP-F) The main thing is that you can consult a specialist remotely, which I think is important, and you can ask if you don't understand something. (Caregiver 3) In the beginning, I didn’t know anything about cleaning, changing dressing, turning and massaging … he kept shouting ‘pain’, I didn't know whether it was because of the pain of the leg or the pain of the wound, and it made me very scared. (Caregiver 4)
Perceived ease of use
Perceived ease of use emerged as an important consideration influencing potential adoption of the AR pressure injury assessment tool. Participants discussed the anticipated effort required to learn and operate the system based on the demonstrated interface and workflow. Three sub-themes were identified: user interface (UI) design, navigation, and appointment waiting time for remote introduction.
UI design
Both caregivers and healthcare professionals emphasized that the interface would need to be simple and intuitive, particularly for users with limited technological experience. As one healthcare professional noted: It might be possible if the glasses were simple to operate, but it's more difficult to operate for some of the older age groups who don’t use electronics much. (HP-B) I would actually prefer that the caregivers, even if they only have a junior high school education, can learn to operate quickly. (Caregiver 6) We can’t operate well with English, and that's the aspect I’m most worried about. (Caregiver 10) My mom and dad probably couldn’t understand the specialized terminology. (Caregiver 9)
Navigation
Participants highlighted the importance of clear guidance for first-time users. Caregivers emphasized the need for a comprehensive tutorial and step-by-step instructions: Definitely need a tutorial. Just like I didn’t know how to use VR glasses the first time I used them and needed to read the instructions. (Caregiver 3) It is important to tell about the effectiveness of AR glasses and to make them understand it in common tongue so that it is easy to convince them. (HP-E) I think we should first let the patient and family experience it. You can have them try to measure with AR glasses on a dummy. (HP-A)
Availability of immediate remote guidance
Caregivers described a desire for timely professional support, especially when they lacked experience in pressure ulcer care: Many people are scared when they see a pressure sore. We're scared too. (Caregiver 1) It would be much easier to get reminders and guidance from a professional than to take care of it yourself. (Caregiver 5) When I've asked for help remotely from a doctor before, the doctor wasn't always available and sometimes couldn't respond within a day. (Caregiver 9) The wait time, like if it will wait long and if it's going to get response all at once. (Caregiver 4)
Intent to use
Intent to use reflected participants’ conditional willingness to adopt the AR device following exposure to the demonstrated system functions, including cost and effectiveness, patient privacy and data security, as well as user experiences related to the AR devices. Participants would consider concerns such as perceived benefits and cost to decide whether to use the device.
Cost and effectiveness
Caregivers generally indicated that their willingness to adopt the technology would depend on its perceived value relative to cost. During the interviews, the upfront cost of the AR hardware (approximately US$3500 for a Microsoft HoloLens 2) was identified as a primary economic barrier, which participants described as equivalent to the price of three high-end smartphones. A caregiver noted: Overall, I think this technology should help, but first there's the price. (Caregiver 3) If it is quite expensive, some patients’ families may not be able to afford it. (HP-C) Middle class families may be okay with it, but the normal family will be very concerned about these aspects (cost). Usually if we use more consumables, they will ask questions on discharge. Cost is also a big thing. (HP-G) It's only more acceptable if it goes into health insurance, which is good for the patient and the family. (Caregiver 10) In terms of cost, I think AR may be cheaper than visiting a doctor offline due to saved transportation costs and time. (Caregiver 4) As long as I can stay up less, worry less, and my dad suffers less, it's good enough … I care more about whether it would help … and I don't care about the price if it helps me solve my problem. (Caregiver 3)
Patient privacy and data security
Participants raised concerns about image storage, data security, and the sensitivity of wound-related visual data. These concerns were particularly significant given the use of camera-enabled devices in private care settings.
First, participants expressed anxiety about the security of images and the potential for unauthorized access. As one caregiver noted: Where to store the pictures taken is more of a concern because my brother is younger and cares a lot about privacy and he is afraid that his pictures will be seen by others. (Caregiver 3) My aunt is more concerned about privacy, she even refuses to go to the hospital because she doesn't want to be face-to-face, and she will be more concerned if her face is photographed when remote video is used. (Caregiver 7)
User experiences
Participants with prior experience in AR or related technologies expressed curiosity and cautious optimism, particularly valuing the ability of AR devices to interact with real-world surroundings. This capability was seen as a useful complement to video during remote pressure injuries consultations. I've used AR before, it was combined with cultural tourism, or interactive games in scenic spots … When you put it on, there is a screen suspended in the air, and your fingers can operate it, like a science fiction movie. (Caregiver 8) I've tried AR glasses, and these seem to be particularly heavy, so I might wear them for 15 minutes at most. So I think the weight has an impact on the experience. (Caregiver 12) I’ve tried VR, not AR, and it's easy to get dizzy, so I’m kind of concerned about that. (Caregiver 11)
Computer anxiety
Participants expressed concerns about computer anxiety, particularly regarding caregivers’ varying levels of familiarity with digital devices. Many caregivers reported being unfamiliar with digital devices in general, which led to anxiety about using AR technology for pressure injury assessment. This anxiety often stemmed from a fear of being unable to operate the AR application correctly: I don’t use my smartphone much, so I'm afraid I can't handle these glasses. (Caregiver 4) Some people are not as receptive as others … they may not necessarily be able to operate it, even if it is a simple operation. (HP-F) Everyone has a different attitude, some elderly people will not be so positive and may feel that what is in the glasses is cheating him. (HP-G)
Computer efficacy
In contrast to concerns about computer anxiety, some participants demonstrated a notable sense of computer efficacy, expressing confidence in their ability to use new digital devices. Healthcare professionals often displayed less worry about adopting AR technology due to their previous experiences using various electronic devices during work: We usually used video or phone to communicate with patients and caregivers before … and the AR technology helps me see the wounds more clearly, which I think is a nice improvement. (HP-B) I used to ask DOUBAO (an AI product) when I had problems … and then I realized that I couldn't trust all of its answers. So I think it's good to have such an AR to solve the problems. (Caregiver 12)
Discussion
This study aimed to explore users’ perspectives on the feasibility of applying AR technology for remote pressure injury assessment. The findings suggest that while the technology is perceived as highly useful for improving assessment accuracy, its adoption hinges on overcoming specific barriers related to hardware costs, interface complexity, and the digital literacy of older caregivers.
Perceived usefulness motivates users to utilize AR. Our results demonstrated that participants specifically identified the AR tool's ability to provide real-time, objective wound measurement as its most distinct advantage over traditional photo-based consultations. Healthcare professionals in our study noted that standard two-dimensional photos often suffer from lighting inconsistencies, whereas the AR device's spatial mapping offered actionable data for staging injuries. This aligns with findings by Dinh et al., 29 who demonstrated that AR enhances efficiency through real-time image superimposition. It should be noted that the performance of AR devices may be influenced by environmental lighting conditions, including strong backlighting or insufficient illumination, which can affect sensing accuracy and visual clarity. 30 Therefore, while AR-assisted visualization shows promise for improving remote assessment, stable environmental conditions remain important for reliable clinical use.
Beyond environmental constraints, the ultimate clinical impact of AR depends on the fundamental precision of its measurements and classifications. Existing literature confirms the clinical potential of head-mounted displays such as Microsoft HoloLens 2.30,31 Studies indicated that the device typically maintains an error margin within 2 to 10 mm during clinical mapping tasks. 25 Yet, despite these validated technical capabilities, participants in this study expressed concerns regarding the system's reliability. Such mixed attitudes reflect a common phenomenon in technology adoption, where user trust requires not only hardware capabilities but also perceived security. 31 Consequently, rigorous evaluation is required before deployment in the real world. Additionally, AR's ability to provide immersive learning experiences and enhance practical skills suggests that it can be an effective tool for training healthcare professionals in pressure ulcer care. Studies have shown that nursing students significantly improve their pressure ulcer assessment skills and motivation after receiving AR-based training. 32
Regarding perceived ease of use, our results revealed a significant digital divide between mobile app proficiency and the complex gesture controls of the HoloLens 2. Participants expressed concerns about the difficulty in learning how to use AR. This confirms prior research indicating that inaccurate gesture recognition can adversely affect user experience. 33 Uniquely, our study identified a projected anxiety among caregivers—not just for themselves, but for older family members. This validates the TAM in a family-care context, showing that ease of use is a collective family concern. 34 To address this, our participants specifically requested hands-on simulation training. This extends the work of other studies indicating that even highly beneficial AR applications may fail to gain widespread adoption if users perceive them as overly complex.35,36 Effective UI design communicates an application's utility clearly and ensures a low-friction learning curve.37,38 Additionally, current AR glasses still face limitations in visual instability and inaccurate gesture recognition, which can adversely affect user experience. Therefore, an easy-to-use AR interface for remote pressure injury assessment must balance ease of operation with robustness to minimize errors and user discomfort.
The intent to use AR for remote pressure injury assessment is determined by a specific economic calculation identified by our participants. While the high upfront cost of the hardware was a major barrier, caregivers expressed a willingness to invest if it offsets the long-term costs of ambulance transport and professional home visits. This confirms the findings of previous studies that remote consultations reduce the burden of travel.39,40 Although hardware cost was identified as a major adoption barrier, the price of AR head-mounted devices is expected to decrease as such technologies become more widely adopted and commercially mature, potentially improving accessibility in home-care settings over time. 41 Furthermore, consistent with general privacy literature, 42 our participants expressed hesitation regarding data security, specifically fearing that live camera feeds into their homes might be intrusive, highlighting the need for privacy-by-design in AR home-care tools.
External elements are recognized as individual differences that shape perceived usefulness and perceived ease of use. These commonly include computer self-efficacy, computer anxiety, and experience with technology. 43 Interventions aimed at alleviating computer anxiety, such as specialized computer courses and web-based training, have been shown to increase acceptance of new digital tools. 44 Our results highlighted that prior experience with smartphones did not necessarily translate to confidence with AR glasses. This challenges the previous assumption that general computer self-efficacy automatically predicts AR acceptance. 45 Older participants in our study exhibited higher anxiety, which is consistent with the findings of Jokisch et al. 46 However, our findings suggest that this anxiety is not insurmountable; it is mitigated by the presence of real-time remote guidance. Participants felt empowered when they knew a professional could see what they see and guide them step-by-step. This indicates that for remote pressure injury assessment, the human element is the critical external variable that transforms computer anxiety into confident care management, such as the real-time guidance from the professionals.
Strengths and limitations
This study was one of the first to investigate AR applications in remote pressure injury assessment. In-depth qualitative insights were provided from the multi-dimensional perspectives of healthcare professionals and caregivers based on technology acceptance modeling theory. While the findings provided valuable insights into user perceptions, there were still limitations. First, the focus on user perspectives did not encompass the views of all stakeholders. Viewpoints from healthcare administrators and technology developers were not captured, whose perspectives were also critical for developing a comprehensive adoption strategy. Second, although the sample size met saturation requirements for qualitative research, the number of participants remained relatively small. Consequently, the generalizability of the findings was limited by specific backgrounds and characteristics of the participants. Fourth, participants were introduced to the AR pressure injury assessment system through standardized demonstrations rather than direct hands-on use. While this was effective for exploring perceived usefulness and acceptance, it may not fully capture experiential factors related to embodied interaction associated with wearing head-mounted AR devices. Finally, we did not directly measure clinical efficacy and patient outcomes, broader evidence requires further research to address the existing gap.
Conclusions
This study explored the perspectives of healthcare professionals and caregivers regarding an AR application for remote pressure injury assessment. The findings indicated strong perceived usefulness and high intent to use, highlighting the AR tool's potential to enhance assessment accuracy and communication in remote care. Additionally, considerations like UI design, navigation, cost, and data privacy were consistently raised by participants. These insights underscore that while AR can help to improve remote pressure injury management, prioritizing intuitive usability and addressing privacy concerns is critical for successful adoption. Future research should quantitatively assess the effectiveness of AR applications on patient outcomes and healthcare efficiency.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261435730 - Supplemental material for Perceptions and feasibility of augmented reality for pressure injury care among healthcare professionals and caregivers: A qualitative study
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261435730 for Perceptions and feasibility of augmented reality for pressure injury care among healthcare professionals and caregivers: A qualitative study by Yan He, Jiayu Gong, Siyi Li and Liling Zhang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076261435730 - Supplemental material for Perceptions and feasibility of augmented reality for pressure injury care among healthcare professionals and caregivers: A qualitative study
Supplemental material, sj-docx-2-dhj-10.1177_20552076261435730 for Perceptions and feasibility of augmented reality for pressure injury care among healthcare professionals and caregivers: A qualitative study by Yan He, Jiayu Gong, Siyi Li and Liling Zhang in DIGITAL HEALTH
Footnotes
Ethical considerations
This study was approved by the Human Research Ethics Committee of City University of Hong Kong (approval number: HU-STA-00001179). Written informed consent was obtained from all participants prior to participation. To protect participant privacy and confidentiality, all personal data were de-identified, and audio recordings were securely stored and accessible only to the research team.
Consent for publication
Consent for publication was obtained from all participants. They were informed that their anonymized data and quotes would be used for publication.
Author contributions
Yan He: investigation, formal analysis, data curation, writing—original draft, and writing—review and editing. Jiayu Gong: data collection and formal analysis. Siyi Li: supervision and writing—review and editing. Liling Zhang: supervision and writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Guangzhou Science and Technology Program, grant number 2025A03J3144.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data availability statement
The datasets generated during and analyzed during the current study are not publicly available as they are being used for a larger, ongoing research project. They will be made available in future publications. However, the data are available from the corresponding author upon reasonable request.
Generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the authors used Gemini (Google) to improve the linguistic quality, flow, and grammatical accuracy of the manuscript. This technology was also utilized to help translate qualitative participant quotes into an academic format while preserving the original meaning. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Supplemental material
Supplemental material for this article is available online.