
Abstract
Good health is a prerequisite for individuals to function in everyday life. The same applies to newly arrived immigrants, where good health is crucial for successful establishment. The aim of this study was to describe stakeholders’ experiences of how newly arrived immigrants’ health affects their opportunities to establish themselves in society. The study had a qualitative design where open-ended questions were analysed following Braun and Clarke’s guidelines for conducting a qualitative thematic analysis. The results consist of three themes: Mental health problems, disabilities, and tormenting concerns about absent family members; A precarious life situation related to housing, education, and income; and Deficiencies in responding to health challenges in organisations and in society. Stakeholders face health problems among newly arrived immigrants that they do not have the right skills to deal with. We argue for the presence of nurses in organisations working with newly arrived immigrants, and that nurses’ competence is necessary to capture their needs.
Introduction
Approximately 80 million people around the world have been forced from their homes because of conflicts and war, and nearly 26 million of them are refugees. 1 In the early 2000s, around 30,000 people applied for asylum in Sweden every year. This figure increased around 2012, and in 2015 the number of asylum seekers was the highest ever, with over 160,000 people applying for asylum, and in 2016, the total number of newly arrived immigrants in Sweden was over 163,000. 2 In Sweden, the introduction of newly arrived immigrants is organised through a policy programme ‘Establishment programme of newly arrived immigrants in Sweden’ (EP). 3 This programme is addressed to individuals aged between 20 and 65 years according to the concept above, and aims to speed up the introduction of new arrivals into the labour market. The EP includes municipal adult education in Swedish for immigrants (SFI), work preparation and community orientation. 3 In this article the concept ‘newly arrived immigrants’ is used consistently. The concept includes individuals who have recently been granted a residence permit as a refugee, individuals with subsidiary protection status or who are family members to any of those mentioned with temporary residence permit.
Good health is a prerequisite for an individual's development and for being able to function in everyday life. 4 The same applies to newly arrived immigrants, where good health is crucial for successful establishment in the new country. 5 A scoping review of migrants’ and refugees’ health status and healthcare in Europe 6 has shown that refugees and migrants tend to have higher prevalence of mental distress compared to non-refugees in Europe. This is consistent with studies of refugees and newly arrived immigrants in Sweden.7–10 Furthermore, a Swedish study has shown that newly arrived immigrants with temporary protection have worse mental health outcomes than those granted a permanent residence permit. 11 Previous studies have reported that social participation has positive effects on health. Being an active member of a community and having close relationships play key roles in physical and mental health and protect against poor psychological health outcomes.12–15
Health is a key concept for nurses and for other professions that deal with health issues. In this study, health should be understood as multidimensional and interlaced with the human experience of being a ‘self’, through existence and interaction with other human beings capable of realising life projects. 16 Health can be understood from another perspective as processes aimed at strengthening the individual's ability to control and influence different health-promoting factors. 17 There is a current shift regarding addressing health and concerns about the well-being of newly arrived immigrants, where the responsibility for addressing these concerns has moved to employees working in the establishment programme and to voluntary work done by civic organisations. This shift is interesting to research, not least in nursing, since the need to understand social participation is fundamental to health-promoting activities for newly arrived immigrants. And there are many unknown stressors that need to be understood to offer appropriate preventive healthcare and to be able to continue working with evidence-based evaluations and interventions.18,19
In this article, ‘stakeholders as volunteers’ refers to persons who organise various social activities for newly arrived immigrants such as language cafés, wellness and sports activities, and cultural activities within municipalities and organisations. Stakeholders can also work in areas such as language education, mainly in Swedish for adult immigrants or in areas aimed at supporting immigrants’ orientation in Swedish society. Staff in the labour market, such as employees of the Swedish Public Employment Service or similar private alternatives, are also included in this group. Stakeholders are facing a variety of challenges when responding to the needs of newly arrived immigrants as they adapt to their new situations. In a newly published scoping review 13 from the stakeholder's perspective, bureaucracy, including time pressures, linguistic and cultural differences, as well as a lack of continuity in the establishment process, are named as factors that act as barriers and consequently have a negative impact in the organisational context. 13 These challenges can also have an impact on the health of newly arrived immigrants.4,12 Stakeholders meet newly arrived immigrants in different environments and situations and thus together possess great knowledge and broad experience about the establishment process and what can affect it. By raising this knowledge, a broader understanding of the establishment process can be obtained. The aim of this study was to describe stakeholders’ experiences of how newly arrived immigrants’ health affects their opportunities to establish themselves in society.
Study design
This study had a qualitative inductive design. Data were collected from the open-ended questions in a Delphi study. 20 The question areas were about stakeholders’ perceptions and experiences of newly arrived immigrants’ opportunities, obstacles and conditions for learning Swedish, getting a job, social participation and being established in Swedish society. The questions were generated from a study of policy documents linked to the ‘Establishment programme of newly arrived immigrants in Sweden’. 3 The first version of the questionnaire was tested based on whether the questions could be understood and answered by colleagues in the same field, after which the questions were adjusted.
Setting and informants
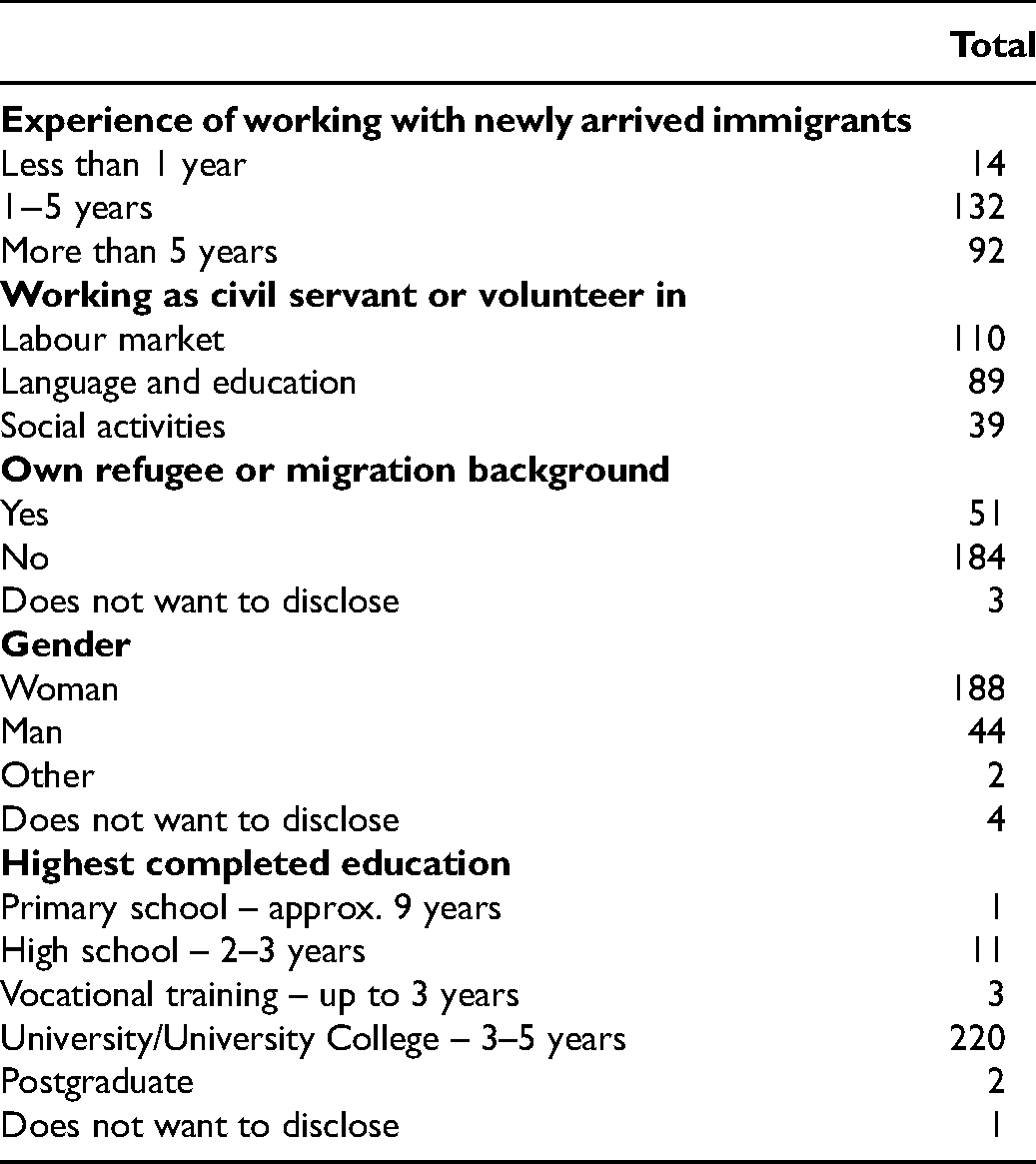
The stakeholders were recruited by a key person who was asked to find people they considered relevant experts for the study. Data were gathered between October 2018 and March 2019. All the answers from 15 open-ended questions were collected from a total of 237 stakeholders (Table 1); 55% of the stakeholders had worked with newly arrived immigrants for one to five years and 39% for more than five years; 46% worked with immigrants in the labour market, 37% in language and education, and 17% with social activities. About 20% of the participants had their own experiences of being a refugee or migrant.
Characteristics of the included stakeholders.
Data analysis
A qualitative thematic analysis (QTA) is, according to Braun and Clarke, a method for identifying, analysing, and reporting patterns within data. 21 The process involves a progress from description, where data are organised and summarised, to a process of interpretation of data. The first and last authors together carried out all phases of the analysis. Beyond this the emerging analysis was regularly critically discussed several times by the whole research group. Trustworthiness of the analysis was considered throughout the whole process, 22 and this is described in Appendix 1 (see the supplemental material online). The first phase in the analysis was to become acquainted with the data through several readings to get an overall understanding of its content. After that, all open-ended answers were read again, to identify how the data corresponded to the aim of study to find extracts that could be connected to health. The second phase was to create codes. Data were read through systematically again with the intention of organising and generating initial codes, related to the content without losing its meaning. This was done by colour-marking data with similar content. In the third phase a first attempt to create potential themes was carried out. All coded data were sorted into groups with similar content, which resulted in five potential themes. The fourth phase was to re-examine the potential themes. Extracts were repeated to check that the themes were relevant to the coded extracts and the entire data set. This reading resulted in one of the potential themes being included in the other themes. The fifth phase was to define and name the themes. Through the analysis, three themes emerged that are presented in the Results section. An overview of the analysis phases is presented in Table 2.
Overview of the process of analysis.

Ethical considerations
Ethical approval to conduct the study was granted by the Ethical Review Board in Stockholm (2018/871–31/5). The General Data Protection Regulations were fully complied with. In accordance with the Swedish Research Council guidelines 23 a high priority was to protect the informants’ confidentiality. All information that could reveal informants’ identities has been concealed, such as working places, names etc. 24 All participants were given written and verbal information about the study, and were told that participation was voluntary. Informed consent was secured in an explanatory letter about the study.
Results
The results consist of three overall themes as follows: Mental health problems, disabilities, and tormenting concerns about absent family members; A precarious life situation related to housing, education, and income; and Deficiencies in responding to health challenges in organisations and in society. Themes presented in the results are delimited towards each other, at the same time as they are closely connected and create a whole.
Mental health problems, disabilities, and tormenting concerns about absent family members
The stakeholders describe how newly arrived immigrants feel unwell and suffer from mental health problems to varying degrees. Some are perceived to be traumatised due to experiences of and fleeing from war, as well of involuntary separation from family members. Some of the newly arrived immigrants testify about beatings, torture, and rape, which have affected them or their relatives. At the same time, the stakeholders describe how the newly arrived immigrants do not always consider themselves to have mental health problems, but rather see themselves as ‘feeling bad as a consequence of their situation’. The concept of mental illness is unknown to many, or associated with prejudice and stigma, which is an obstacle to seeking help. There is also a lack of knowledge about the possibility of seeking help. One stakeholder described it this way: They do not understand how healthcare works in Sweden and for many of these (newly arrived) students needing psychiatry means that they are crazy, which is a loaded word.
The stakeholders also state that the consequence of this is that newly arrived immigrants are not able to fully participate in various activities, such as going to school, language education, work training or other social activities. They feel too overburdened to find motivation, or to concentrate and interact with new people. This makes it difficult to absorb information and new knowledge. Some stakeholders also state that they have met persons with serious physical illnesses for which they have not sought care, or persons who have illnesses where additional treatment is required.
In addition, there is often a lack of knowledge about current illnesses, medication, and the ability to self-care. At the same time, stakeholders state that it is common for newly arrived immigrants to suffer from various types of disabilities, ranging from mild to more severe. These disabilities sometimes occur in combination with mental illnesses, and often go undiagnosed. Visual and hearing impairments are widespread, and aids are often lacking. Some stakeholders report that younger people do not want to use hearing aids or glasses because it is perceived as stigmatising. Furthermore, the stakeholders believe that ‘cognitive difficulties’, and ‘intellectual disabilities’ are common. Although illiteracy is not considered a disability, it is highlighted as a problem. The following quotation illustrates this: Those I meet cannot cope with school; they often have a previously undiagnosed intellectual disability (developmental disorder). Extremely vulnerable young people!
The stakeholders also state that many newly arrived immigrants have strong concerns about family members who remain in their home country and are in or fleeing a war zone or are missing. Concerns about what is happening to them and how they can help them, not least financially, are often debilitating. The anxiety and uncertainty cause feelings of being distressed, sometimes aggravating already established mental health problems, which makes it difficult to recover. In addition to concerns for family members, there is also a great concern about permanent residence permits, which is often a prerequisite for family reunification. The process is perceived as uncertain, and the long wait for a decision has a negative impact on their already fragile health. Likewise, the uncertainty regarding the possibility of returning to one's home country can be a source of concern. One stakeholder described it this way: I have met many who find it difficult to focus on language learning if their family members are still on the run. Every effort is made to try to reunite the family and, in the meantime, support them in their homeland and while fleeing.
The stakeholders also state that many new arrivals express a great sense of loneliness. They lack family, friends, and social networks both within and outside their own ethnic group, and many live in isolation and struggle with loneliness every day.
A precarious life situation related to housing, education, and income
The stakeholders declare that new arrivals often have an uncertain housing situation. They are homeless, have temporary housing, are forced to move around, or are referred to live with people they have not chosen. They must sometimes also move to smaller municipalities to get housing, where it is more difficult to find a job. For the new arrivals, housing and apartment contracts are an important step in the effort to be reunited with their families. Furthermore, stakeholders state that precarious housing situations have a negative impact on the ability of new arrivals to concentrate and manage activities such as language learning and education, not least for those who are already feeling unwell. The following quotation illustrates this: The housing situation is very stressful for many and does not provide the peace and quiet needed to be able to establish oneself in Swedish society.
Learning Swedish is the first step in the establishment programme, and speaking the language is usually a prerequisite for getting a job. The educational background of the new arrivals varies; at the same time, the stakeholders state that they encounter a significant proportion of people with a very low level of education. Some of them also lack basic computer skills and driving licences. Some stakeholders say that simpler work without requirements for Swedish language skills would be of great benefit to many newly arrived immigrants. At the same time, they confirm that it is difficult to find employers who will employ newly arrived immigrants without Swedish language skills. One option that is proposed is workplaces with multilingual supervisors.
The stakeholders also state that they meet newly arrived immigrants who do not enter the labour market, and who have expressed stress and anxiety about their own and their family members’ livelihood. Work is often perceived as a prerequisite for a permanent residence permit and family reunification. One stakeholder describes it this way: Many of the obstacles I can see in my encounters with new arrivals are about the daily mental pressure that many people live under. The stress of quickly learning Swedish, getting housing and work to be able to support your family, the worry about family members who are ill or that you yourself are ill and the worry about family members that you are struggling to get here. And all problems are linked to the issue of permanent residence.
Some stakeholders describe that the state of unemployment makes it difficult to dispel anxious thoughts and maintain routines in daily life, which has negative consequences for newly arrived immigrants’ already fragile health: The most important thing to feel well is probably that you are seen for who you are, and for the knowledge you have and can contribute. Being able to support oneself is extremely important. If you get opportunities, you also want to give back.
According to this quotation, a prerequisite for feeling included and involved in the Swedish society is to be seen for who you are and what you can bring as a person.
Deficiencies in responding to health challenges in organisations and society
The stakeholders describe limited resources, but above all shortcomings in the coordination and cooperation between different actors, such as authorities, the healthcare sector, and the municipalities. Sometimes conditions, sustainable structures and mandates are also lacking. These shortcomings cause newly arrived immigrants not to receive the necessary help and support. Rather, they end up in the ‘gap’ between different administrative authorities or are continuously being sent from one to another. The stakeholders argue that more and better cooperation would be the solution to many problems. The following quotation illustrates this: Collaboration feels like the ‘solution’ to a lot − those authorities and organisations coordinate more than they do today. Many times, I feel that we work twice as much.
Regarding their own organisation, reduced personnel resources are described despite the heavy workload. Due to lack of time, meetings with new arrivals ideally take place by telephone, despite language barriers. In addition, stakeholders describe a frustration that what they have to offer can be adapted only to a small extent to suit the needs of the individual.
In the first theme, the stakeholders state that they meet newly arrived immigrants with mental health problems. They also say that they lack sufficient knowledge to encounter these persons in a professional way, and that skills and resources within their own organisation and in society in general are limited or non-existent. They have requested knowledge development and professional guidance in their work. Likewise, there is a demand for greater cooperation with healthcare professionals such as nurses and psychologists, as well as qualified interpreters. One stakeholder described it as follows: The own organisation has no training, no skills development to offer its employees regarding new arrivals, their feelings, PTSD and or mental illness /…/
I believe that the need is greater than what healthcare today can handle in a good way and within a reasonable time. There are long waiting times and poor information about support and treatment for mental illness.
At the same time, the stakeholders describe limited resources in the education sector such as a waiting period of up to one year for SFI. During this waiting period the newly arrived immigrants have limited opportunities to move forward in the integration process, which creates stress and anxiety that can negatively affect their mental health. But above all, they describe the problem that SFI, and the school, have not adapted their activities to accommodate persons with different needs; instead, everyone is referred to the same system, regardless of educational background, functionality, cognitive ability, or illiteracy. The following quotation illustrates this: One problem is illiteracy and to adapt the teaching accordingly, as well as visual and hearing impairments that are not noticed or that are hidden and SFI does not take this into account in their teaching.
Some stakeholders explain that the issue of persons with low levels of education, illiteracy, or impaired cognitive ability, is not publicly discussed, with the explanation that the subject is something of a taboo. This might be because it could be used by xenophobic forces. Unfortunately, the consequence is that newly arrived immigrants do not get the help and support they need.
Our results show that the stakeholders address a range of mental health problems, disabilities, anxiety, and loneliness in their everyday interactions with newly arrived immigrants. Traumas experienced due to pre- and post-migration burdens and involuntary separation from family members are described as common in the stakeholders’ everyday encounters. The stakeholders describe limited resources and lack of knowledge in relation to various health problems they must deal with. At the same time, the lack of coordination and cooperation between different actors appears to be a key issue.
Discussion
To summarise, we emphasise that stakeholders deal with a complex situation concerning newly arrived immigrants and their health. In their work with the establishment, they face health problems they do not have the training and skills to deal with. It also appears that newly arrived immigrants with health problems risk ending up in a ‘gap’ due to lack of coordination between different actors in the establishment. Based on this we believe that the stakeholders need the competence and support of nurses in their daily work in order to be able to better assess newly arrived immigrants’ health problems and care needs, and to mediate the right care contact.
Our results show examples of the complexity of problems that stakeholders meet in encounters with newly arrived immigrants. In general, working with health and integration of newly arrived immigrants is regarded to be a broad institutional challenge for the receiving country. Tinghög et al. 9 show, in a Swedish study, that one in three newly resettled refugees from Syria had marked symptoms of depression and anxiety. In the same group, 30% showed symptoms consistent with a post-traumatic stress disorder (PTSD) diagnosis and over 60% of newly resettled Syrians indicated that they had poor social support. Another study by Sigvardsdotter et al. 25 shows that people who have fled their country have often experienced acute trauma and are vulnerable to different health issues. A population-based Swedish and Finnish study of Iranian and Iraqi refugees who have been subjected to torture, shows that their health and social conditions are negatively affected to a great extent. 26 These results support our conclusions that there is a need for screening and early follow-up of new arrivals’ health conditions, where nurses have an important role to play.
Further studies also shows that the most prevalent type of mental health problem among newly arrived immigrants and refugees are depression, PTSD and anxiety.8,27 One Swedish report shows that challenges for entry into the labour market are lack of social network, no contacts with employers and lack of language skills. 28 According to different studies, social participation plays a key role for physical and mental health and protection against poor psychological health outcomes.29,30 Concerns addressed by the stakeholders presented in this study show that they are worried about how newly arrived immigrants’ health, more specifically mental health and other disabilities, affects their opportunities to be integrated into society. As the stakeholders point out, there are various types of disabilities, sometimes occurring in combination with mental health problems. Visual and hearing impairments are widespread, and aids are lacking. Furthermore, ‘cognitive difficulties’ and ‘intellectual disability’ are also common. Stakeholders also state that newly arrived immigrants suffer from a great feeling of loneliness and lack of appropriate environment to be in, , which has a negative impact on their health, and they emphasise the importance of work, but state that the requirement for language skills is often an obstacle to moving forward in the establishment process. One current study shows that loss of and separation from loved ones, as well as forfeit of the homeland, were cited as sources of psychological distress that create a sense of sadness. 31 Sengoelge et al. 32 stress the importance of family reunification for social support. Living with this situation of overwhelming uncertainty affects the newly arrived immigrants and has an impact on their everyday lives.
Using Penrod's 33 concept of uncertainty, we can argue that the situation for the newly arrived immigrants and the stakeholders creates a situation of ‘overwhelming uncertainty’, with low control and low confidence for everyone involved. Even if we acknowledge that this situation primarily relates to the newly arrived immigrants, our results show that the stakeholders, due to lack of knowledge, resources, and difficulties in the coordination between different actors, are also drawn into this situation of uncertainty.
Our findings indicate that the presented range of mental problems, disabilities, anxiety and loneliness, uncertain life situation in relation to limited resources, shortcomings in the coordination between different actors and the overwhelming uncertainty that these problems create, can be addressed, and sometimes also resolved with the right competence. Stakeholders also address the fact that an important prerequisite for being able to provide the right support and to empower newly arrived immigrants is to see and listen to each person and their story.
Larsen et al. 13 show that bureaucratic procedures and high ‘hassle’ factors that the stakeholders address, with lack of empowerment and self-sufficiency among refugees in relation to health, are a global problem, and must therefore be addressed globally. Global nursing is about developing knowledge of health and care in a local and global context. 34 Nurses have been identified as a professional group that is crucial to achieving the global goals set by the United Nations in the 2030 agenda. 35 Achieving these global goals is based on work that takes place locally. A global perspective also includes the demographic and organisational changes that are taking place locally, where care and nursing as an activity will become even more complex. 4 However, in the local context we need to put more focus on global mobility that allows nurses to address global issues. Nurses are the key profession that is expected to lead the work of these emerging health challenges, locally as well as globally. 36 Therefore, there is a need to develop global nursing in the curriculum of nursing education.
The presence of nurses in organisations that work with newly arrived immigrants can help to increase competence among stakeholders and capture the newly arrived immigrants’ needs. 37 We strongly argue for a global call for nurses to step up and become coordinators for the care of newly arrived immigrants. Wilson et al. 36 argue that nurses with global competence are equipped to conduct an ethical activity with respect for human dignity based on knowledge of human rights and cultural diversity. They can participate in decision-making and nursing processes with reflective considerations in mutual partnership with other care providers and actors. We also want to address stakeholders’ needs for competence development when working in such complex areas. This was something that stakeholders clearly expressed.
Finally, nurses could fill the role of being the ‘spider in the web’, providing healthcare and ensuring universal access to healthcare. Nurses have the potential to make significant contributions to global health and to sustainable development. Nurses should play an important part in any national or international establishment programmes for newly arrived immigrants.
Limitations and strengths
The choice of method used for the analysis will be critically described, based on aspects related to trustworthiness and credibility. The credibility of a study involves aspects such as how to select key findings and how well the interpreted themes illuminate the phenomenon.22,38 Particular considerations have been taken when working with each phase of the analysis process. The data were taken from a survey in a Delphi study, and this ruled out the possibility of asking follow-up questions and thereby gaining a further in-depth and nuanced understanding of the stakeholders’ experiences. However, the results provided an overview of what may be relevant to study further. A strength of the present study was that the various stakeholders came from different organisations which gave a breadth in the data. This, combined with the fact that the thematic analysis followed an accurate structure 22 (Appendix 1) increased the credibility and transferability of the results. Trustworthiness of the data analysis was ensured by applying the procedure of the method and formulating the interpreted themes. In this study, the two authors who conducted the analysis reflected on and discussed the content and the thematisation with each other and within the research team. 38 The research team have extensive experience as researchers and of working with qualitative analysis. The process of analysing data benefited from a gender perspective that the research team consisted of both women and men with different experiences. Another strength is that none of the researchers had experience of work as stakeholders, which means that data were analysed without preconceived notions.
Conclusions
Research shows that many newly arrived immigrants suffer from different serious mental health problems. Our findings show that stakeholders address a range of mental health problems, disabilities, anxiety, and loneliness in their everyday interactions with newly arrived immigrants. In the conclusions we want to highlight the following:
Stakeholders face health problems among newly arrived they do not have the training and skills to deal with. The situation for newly arrived immigrants and the stakeholders is one of ‘overwhelming uncertainty’ with little control and low confidence. We argue for the presence of nurses in organisations that work with newly arrived immigrants. Nurses would increase the competence of these organisations, which would promote the establishment process for newly arrived immigrants, based on a more sustainable structure.
Supplemental Material
sj-docx-1-njn-10.1177_20571585221083525 - Supplemental material for The meaning of health among newly arrived immigrants: A qualitative study from stakeholders’ perspectives
Supplemental material, sj-docx-1-njn-10.1177_20571585221083525 for The meaning of health among newly arrived immigrants: A qualitative study from stakeholders’ perspectives by Per Ekstrand, Charlotta Tegnestedt, Marja Schuster, Henrik Eriksson, Ann Hägg-Martinell and Joacim Larsen in Nordic Journal of Nursing Research
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Forskningsrådet om Hälsa, Arbetsliv och Välfärd, (grant number 2016-07194).
Conflict of interest
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.