
Abstract
Introduction/Objectives:
Adolescents frequently encounter online health information (OHI). We aimed to synthesize clinician recommendations for engaging adolescents about OHI during clinical encounters.
Methods:
United States clinicians with expertise in adolescent sexual and reproductive health (SRH) participated in virtual semi-structured interviews. Transcripts were analyzed using rapid qualitative methods to generate descriptive themes.
Results:
Twenty-four clinicians from all U.S. regions participated. Participants emphasized the importance of addressing OHI given its accessibility, ubiquity, broad topical relevance (eg, SRH, nutrition, vaccines), and variable health impacts (ie, positive and negative). Clinicians described 4 entry points for discussion: patient initiation, screening, topic-specific conversations, and resource provision. They suggested strategies to build digital literacy (eg, assessing content creator motivations) and health literacy (eg, contextualizing population risks without dismissing personal anecdotes). Communication approaches included acknowledging partial truths before providing medical context and avoiding blanket dismissal of online content. Clinicians advised against directly labeling patients’ claims as “misinformation,” recommending instead more neutral, patient-friendly language.
Conclusions:
As clinicians increasingly navigate OHI in practice, these expert recommendations can help support digital and health literacy while fostering trust and improving adolescent–clinician communication.
Introduction
Adolescents often access health information online. Over 80% of United States (U.S.) adolescents have looked online for health information (OHI), 1 often on social media.2,3 In addition to active seeking, many also encounter OHI passively.2,4 Engagement in active search may depend on factors such as health status, marginalized identity, or sensitivity of topics like sexual and reproductive health (SRH).5-7 Despite concerns about misinformation (“unintentionally inaccurate information”), 8 disinformation (“intentionally inaccurate information”), 8 and other negative influences such as online safety risks, 9 OHI has benefits such as improving knowledge about sensitive information (eg, SRH content not taught in schools)10,11 and promoting emerging autonomy. 12 For the purposes of this study, we use the broader term OHI to encompass the range of online health content adolescents encounter, including both accurate and inaccurate information.
Navigating OHI poses challenges for adolescents, particularly assessing accuracy and relevance.5,12,13-15 Clinicians remain trusted sources, and patient-sourced OHI increasingly influences clinical care.16,17 Discussing OHI can strengthen trust and collaboration, but may also cause tension if clinicians dismiss patients’ beliefs about OHI.18,19 Currently, no synthesized guidance exists on how clinicians can best approach these conversations with adolescents. While some studies have focused on clinician-patient communication about OHI in the context of adult populations with life-threatening conditions,20,21 to our knowledge no studies have examined clinician communication strategies for discussing OHI with adolescents during routine care.
SRH represents a particularly salient context for OHI given the wide-ranging accuracy of content online22,23 and adolescents’ reliance on digital sources for information not readily available elsewhere.10,11,24,25 Communication strategies developed for value-sensitive topics are generalizable to other areas of health, especially since effective discussions about sensitive topics have positive global effects on adolescent-clinician relationships. 26 Thus our objective was to qualitatively summarize recommendations from adolescent SRH clinical experts on how clinicians can effectively discuss OHI with adolescents.
Methods
Study Design
We conducted a descriptive qualitative analysis 27 of semi-structured interview data following SQRQ reporting guidelines (Supplemental Appendix A). 28
Participants and Recruitment
Eligible clinicians (MD/DO, NP, PA) had self-identified expertise in adolescent SRH, treated patients in the U.S., and for physicians, had completed residency. A convenience sample was recruited via national listservs focused on adolescent care and SRH, an approach selected for its feasibility. Participants were compensated with a $50 gift card for their time.
Interview Guide
The guide was adapted from a prior clinician interview study on communication strategies 20 (Supplemental Appendix B). It consisted of fifteen questions and accompanying probes; domains included beliefs, practices, counseling recommendations, challenges, and considerations beyond the clinical encounter. The guide was reviewed by experts, refined through mock interviews, and iteratively adjusted. Though initially SRH-focused, the guide was iteratively broadened to encompass other health topics raised by participants.
Data Collection and Processing
Interviews were conducted virtually over Zoom by CS. Before interviews, participants completed a demographics survey that confirmed expertise in adolescent SRH clinical care and assessed self-reported skills in pediatric digital wellness and communication about OHI. Interviews averaged 47 min (range: 31-63 min). Recordings were transcribed, cleaned, and lightly edited for grammar. Transcripts were analyzed shortly after collection, continuing until saturation, defined as no new themes after 3 interviews.
Qualitative Analysis
Rapid qualitative analysis, an approach appropriate applied topics
29
that has been shown to generate findings comparable to traditional thematic analysis while being less resource-intensive,
30
was used to identify themes. CS, a researcher with over 10 years of qualitative experience, led analysis using the matrix method.31,32 An Excel spreadsheet displayed major domains on separate tabs (eg, beliefs, recommendations), with columns for specific categories (eg, “concerns about OHI”). Transcript data were sorted into the most fitting column, with notations for emergent cross-column themes. Column summaries were updated after each transcript and were used to document emergent themes and subthemes. SR reviewed all recordings and verified data sorting; discrepancies were resolved by discussion. The core team (CS, SR, LF, BAA) iteratively reviewed final matrices, themes, subthemes, and illustrative quotations to support interpretation, prompting resorting of data until results were finalized. Extensive quotation tables with additional data are provided in the supplement for transparency (
Reflexivity
The research team consisted of physicians, researchers, and physicians-in-training who believe that OHI offers opportunities and challenges for patient care.
Ethics Approval
The University of North Carolina at Chapel Hill IRB designated this study as Exempt (#24-2060). All participants provided written informed consent through an electronic survey.
Results
Participant Characteristics
Characteristics for 24 participants are shown in Table 1. Most were physicians (83%) trained in pediatrics (71%). Among family medicine or pediatric physicians (n = 16), 94% had adolescent medicine fellowship training. Most identified as cisgender women (79%), white (75%), and worked in academic settings (83%). Participants represented all U.S. regions. Over 70% used social media at least daily.
Participant Characteristics.
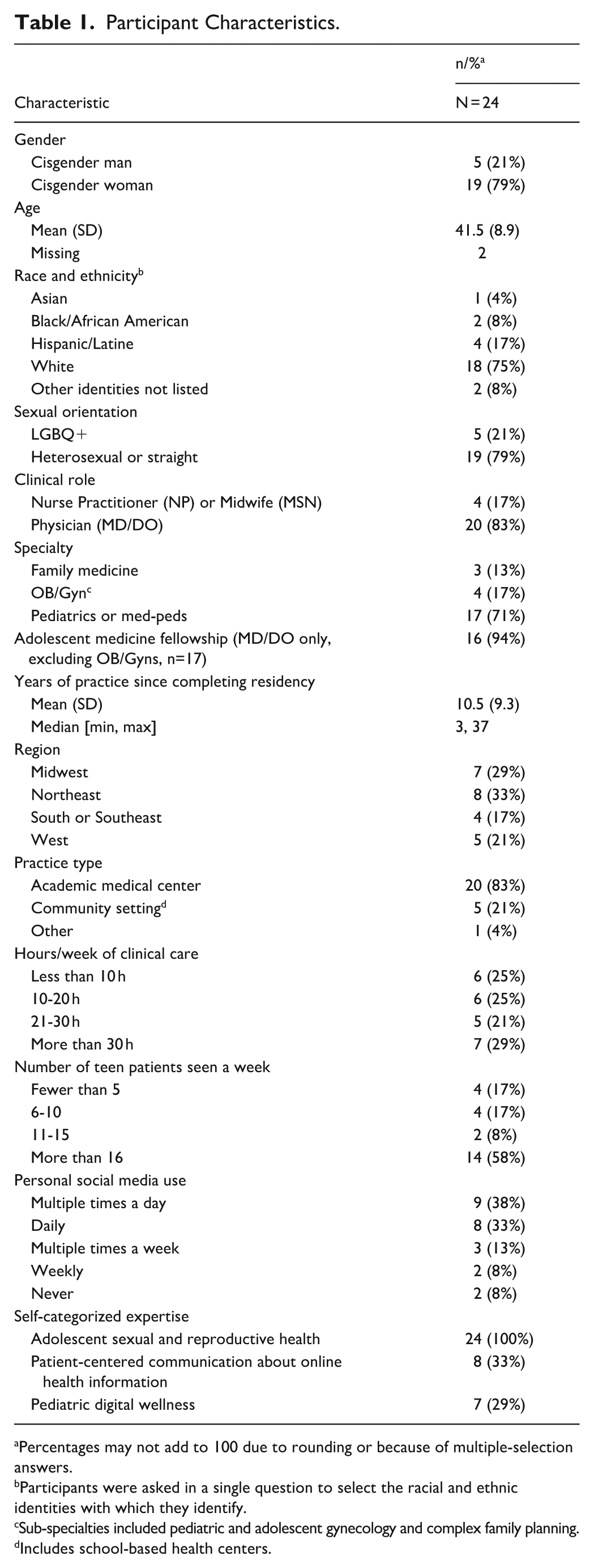
Percentages may not add to 100 due to rounding or because of multiple-selection answers.
Participants were asked in a single question to select the racial and ethnic identities with which they identify.
Sub-specialties included pediatric and adolescent gynecology and complex family planning.
Includes school-based health centers.
All participants identified as experts in adolescent SRH. One-third also reported expertise in communication about OHI, and 29% in pediatric digital wellness. While all were highly comfortable discussing SRH with teens, they were slightly less comfortable discussing online SRH content, with a few outliers at both extremes. Comfort was shaped by personal social media use, parenting teens, familiarity with common OHI, and knowledge of trustworthy alternative health resources.
No participants had formal training in discussing OHI with patients. However, many cited related experience, including media training, health literacy research, academic talks, or instruction in screen time and digital mental health. A few had training in digital content creation. Several—mostly senior fellows or recent graduates—had led didactic sessions on adolescent-relevant social media content.
Why It Is Important to Discuss OHI With Adolescents
Participants discussed the importance of OHI, its unique nature, concerns and benefits, and the consequences of not addressing it (Figure 1). They widely viewed understanding adolescent OHI exposure as essential to modern care.

Common clinician beliefs about online health information.a This figure demonstrates common clinician beliefs related to the importance of online information, its unique characteristics relative to other forms of health information, its broad topical relevance, concerns and benefits, and the consequences of not discussing it in clinical encounters. Additional context for each category of beliefs and illustrative quotes are also included in the figure.
They also reflected on how digital media is reshaping the world in medicine and in their personal lives. All recognized the internet as distinct from traditional information sources, citing its accessibility, low posting barriers, lack of verification, rapid dissemination, algorithmic amplification of extreme content, mixed creator motivations, constant and often passive exposure, and vast individualized content. Participant 3 explained: Phones are really just becoming an extension of who we are, and even more so with AI . . . Opinions are being stated as facts quite regularly . . . I think [that] is something that even adults struggle with, to discern that objective truth. An adolescent is . . . ripe to see misinformation and to consider it to be truthful, and I think it’s up to us as healthcare providers to be one step ahead.
Although clinicians expressed concerns about misinformation, some noted this is not exclusive to the internet and emphasized that OHI can be accurate. They also raised concerns about lack of context (eg, other sources of medical knowledge) and exposure to explicit or harmful material.
Potential benefits included convenience, privacy, engaging formats, and availability of sensitive health information, which increased equity for adolescents without easy access to clinicians. Participants highlighted opportunities for youth to find representation, community, and empowerment, such as Participant 10: It may give them the confidence or the vocabulary to come and have a discussion . . . [and] help them understand what other people are experiencing around them . . . I mean, there was no place to go except . . . the public library when I was growing up . . . And now it’s much more accessible.
The main SRH topics that clinicians believed were influenced by OHI included contraception, human papillomavirus vaccination, polycystic ovary syndrome, relationship/sexual safety, sexually transmitted infections, and vaginal/vulvar health. Other frequently mentioned topics included nutrition, gender-affirming care, body image, eating disorders, dermatologic concerns, mental health, substance use, and vaccines. Participant 11 explained: This has the ability to impact every patient encounter I have . . . it comes up with substance use, and it comes up with mental health, and it comes up with everything that a teenager is going through.
Not asking about OHI was often seen as a “missed opportunity.” Participants noted potential harm to the patient-clinician relationship due to not recognizing the power of the digital world on adolescents, missed chances to correct misinformation or offer alternative credible sources, and risks of negative clinical outcomes if teens felt uncomfortable disclosing influential online content, as described by Participant 8: If we’re not discussing it, we’re missing a huge elephant in the room of what’s shaping behaviors and decisions. By asking about it, you’re normalizing it. You’re inviting the teen into the conversation, and they might otherwise feel like you might judge them for something that they heard on TikTok.
Recommendations for When to Integrate Discussion During a Visit
Clinicians recommended multiple ways to integrate discussions about OHI into clinical encounters. One noted it could happen “a little bit everywhere” (Figure 2; Supplemental Appendix C), with other clinicians recommending integration during (1) patient-initiated conversations, (2) routine screening, (3) responses to specific concerns, and/or (4) provision of outside health resources.

Recommendations for when to integrate discussion of online health information into clinical encounters.a
While some participants supported screening for OHI exposure, others considered asking about this as a “next-level question” (Participant 22) that may not be feasible in routine visits, expanded upon by Participant 21: Thinking of the busy pediatrician . . . screening for depression and anxiety, and then eating disorders and substance use and sexual activity . . . and sleep hygiene. They’re probably talking about social media, not specifically how it relates to information . . . There’s so many things we need to screen for but there’s not enough time.
If not initiated by the patient, most participants found it easiest to discuss OHI in response to specific health topics. Once a topic was identified, some asked broadly about knowledge and information sources without probing about OHI, whereas others recommended directly asking. Participant 9 shared a strategy to normalize the topic: Instead of asking, “Do you use social media . . . to get information?” I just say, “What are the social media people or websites that you get information from?” . . . It makes them feel it’s pretty normal to do that, and they can feel open about sharing what it is that they’re seeing.
Responding to patient hesitation was another common prompt. For example, if a patient hesitated about a treatment and the clinician was aware of popular online content (eg, concerns about medroxyprogesterone acetate and meningiomas), they would ask how that OHI influenced their thinking and decision-making.
Clinicians used resource provision to facilitate discussion about OHI quality, and some described pulling up materials to review together. Resource provision was used by almost all clinicians, even if they did not have time to address digital and media literacy more broadly, as explained by Participant 19: I don’t always talk about sources and the quality. I try to refer like, “These are really good sources . . .” But I don’t know that I spend a ton of time explaining, “Here’s how you know that this is evidence-based.”
Barriers included time constraints, potential discomfort with social media, gaps in knowledge of OHI, and lack of engaging, teen-friendly alternatives. Participants shared that discussing their role as a parent or social media user helped facilitate this conversation, as represented by Participant 12: I sometimes . . . use my kids as like a way to bring it up like, “Hey, my son showed me this. Have you seen this video?” . . . Or “Did you know about this fad or this concern or things that are being talked about on TikTok?”
Recommendations for How to Communicate About OHI With Adolescents
Educational Strategies: “Drama Is What Spreads”
Participants shared recommended educational strategies for either anticipatory guidance or responding to specific OHI (Table 2). Many emphasized digital media literacy, which included (1) Encouraging scrutiny about content creators’ motives or qualifications, (2) Describing characteristics of content most likely to spread online (eg, “drama is what spreads;” Participant 5), (3) Educating about lack of fact checking, and (4) Highlighting additional medical context not shared online. Several recommended asking patients about trust in the information before providing education, noting that some adolescents are already skeptical, as described by Participant 18:
Overview of Clinician-recommended Educational Strategies for Discussing Online Health Information With Adolescents.

I’ve found it’s really helpful to ask . . . how valid they think the information is. Sometimes they’ll watch stuff on TikTok, and you’ll ask, “What do you think of that?” And they’re like, “Oh . . . I think it’s fake. I don’t believe it.” Then you have other people who are like “Oh, my God! All these people are having a terrible experience . . .I would never want that. . .” So finding out, “How valid do you think it is? How reliable do you think it is?”
Clinicians also recommended health literacy approaches, including (1) Explaining broad risks versus anecdotes, (2) Emphasizing individual variability (eg, “the right option for you”), (3) Describing how scientific evidence is generated, and (4) Clarifying health concepts.
Finally, they also provided several forms of guidance for future information searches, including (1) “Pre-bunking” (ie, preemptive warnings about variable quality), (2) Offering verification resources, and (3) Sharing general media literacy tips. Some noted challenges with these tips due to increasing mistrust in traditional sources, like Participant 4: I talk about how websites that end in “edu” or “org” tend to be from institutions that are more trustworthy . . . What’s hard is that there are people [providing inaccurate information] that are using those .org [and .gov] websites too.
Participants also noted that some parents have low health or media literacy, and these strategies could help improve parental discernment as well.
General Recommendations for Adolescent-Friendly Communication
Participants described effective and ineffective ways of communicating with adolescents—and occasionally parents—especially during disagreement about OHI (Table 3). Approaches often varied based on the level of concern, with more serious claims prompting more directive responses.
Clinician Recommendations for Effective Communication About Online Health Information, Especially When Disagreeing With Claims.

Clinicians recommended foundational principles, which included: (1) Centering trust and respect, (2) Remaining humble, and (3) Being curious and asking questions (Supplemental Appendix D). Many stressed that correcting misinformation was secondary to building trust, noting that negative encounters could have lasting effects on adolescents’ willingness to seek care as emphasized by Participant 13: We as clinicians . . . are a stand-in for the healthcare system . . . For many young people, this may be their first time seeing a clinician on their own . . . Setting a tone of being patronizing or dismissive risks that person’s long-term trust in the healthcare system and willingness to seek care. The risks are so immense to me that I would much rather someone leave believing that hormones cause cancer than believing that doctors will never listen to them.
Specific recommended steps for effective conversations included (1) Create a welcoming space, (2) Explore trust in information and foundational concerns, (3) Validate and empathize, (4) Give and receive information, (5) Provide options while avoiding absolutes, and (6) Reassure and empower (Table 3). Understanding the patient’s core concern was often seen as critical to effective conversations, as illustrated by Participant 3: I typically will dig deep, like “Oh, you know, that’s something that I haven’t heard before. Can you tell me more about it, where you heard it or . . . why that resonated with you?” . . . Sometimes they say, “Well, because I don’t want a brain tumor, I don’t want to bleed forever. I want to have fertility.” I say, “Great, I want all those things as well. Let’s talk about the safest ways to get those things to happen.”
In contrast, participants strongly recommended against telling adolescents to avoid social media and/or to dismiss all OHI. They described this not only as ineffective, but also potentially inaccurate, as described by Participant 14: The Internet is not going anywhere, so people just need to know that [teens are] going to be on it. You can’t tell them to just stay off it. You need to understand that there are both positive and harmful effects of being online.
They also recommended against dismissing personal experiences (even if highly unlikely) and lecturing or talking down to patients.
Some strategies—like humor, direct debunking, or labeling claims “misinformation”—were seen as needing more discernment, especially related to preexisting rapport (Supplemental Appendix E). Views on the term “misinformation” varied: some found it educational, while others felt it was stigmatizing or confusing. Those who used it emphasized applying it broadly, not targeting the patient, as explained by Participant 21: I don’t think I have any strong opposition to the word. [My concern would be] pointing it at them versus keeping it broad like, “It’s not your fault. It’s the world’s fault, and we’re helping you navigate it.”
Discussion
We synthesized recommendations from 24 adolescent SRH experts for effective communication about OHI. Participants described integration points in clinical encounters, shared strategies to improve digital and health literacy, and offered guidance for navigating disagreements with patient-identified information. They also discussed patient-friendly language, including how to approach the term “misinformation.”
Although developed from the perspective of adolescent SRH experts, many recommendations—including the use of relational counseling strategies, trust-building approaches, leveraging preexisting skepticism, and providing tailored resources—are likely applicable to general pediatric and primary care settings. SRH-specific recommendations may be less immediately relevant to general practitioners given well-documented gaps in SRH counseling in primary care34,35; however, efforts to increase clinician confidence in SRH content and promote confidential time with adolescents could improve SRH counseling rates36,37 and open additional avenues for discussing OHI given adolescents’ hesitancy to share some forms of online information-seeking with parents.38,39
Participating clinicians frequently recommended relational counseling strategies (eg, aligning with shared goals). Prior research shows many clinicians rely on informational approaches when counseling about patient-identified information, but only some combine these with relational techniques. 20 A recent randomized trial with cancer patients found that combining both approaches resulted in positive patient-reported outcomes, while informational-only approaches were perceived just as negatively as outright dismissal. 21 These findings underscore the importance of combining relational and informational approaches.
Clinicians advised against dismissing all OHI and/or telling adolescents to completely avoid social media. Such approaches were seen as unrealistic and potentially damaging to trust, especially given the central role of digital media in teens’ lives. Consistent with existing literature, respect, empathy, and honesty were emphasized.16,40 Dismissing patients’ views may increase reliance on non-clinical sources, potentially leading to harm.41,42 Thus, grounding conversations in trust and respect while acknowledging the complexity of OHI—even if beliefs remain unchanged—is important for strong therapeutic relationships.
Participants recommended leveraging adolescents’ preexisting skepticism of OHI, a strategy incorporated into digital media initiatives such as Common Sense’s Digital Citizenship Curriculum. 43 Recent data demonstrate low trust in OHI among 18 to 25 year olds (no data were collected for minors), with TikTok and YouTube being most trusted (47%-54%) and Reddit, Instagram, Facebook, and X/Twitter less so (<42%). 44 Adolescent trust is shaped not only by platforms but also by other users (eg, friends vs influencers) and the health content itself. 13
While many of these findings are relevant to individual clinicians, efforts at the educational and policy levels are also needed to promote these skillsets across the pediatric workforce. The American Academy of Pediatrics (AAP) has been focused on promoting social media wellness for patients and families, and their 5 Cs framework for discussing social media includes: Child (how the child interacts with social media), Content (how the content makes the child feel/act), Calm (whether devices are being used for managing emotions or impacting sleep), Crowding out (whether media interfere with other daily activities), and Communication (continuous conversation about media within the family). 42 While all domains are important, our findings align most with Content, offering new strategies for clinicians to support adolescents and families in navigating OHI. 42 As more evidence is generated related to effective communication about OHI, AAP, and other bodies such as the Society for Adolescent Health and Medicine (SAHM) can create guidelines and disseminate continuing medical education content, while medical schools also work to incorporate effective OHI communication skillsets into training. 45
Finally, clinicians emphasized the importance of having trusted alternative resources to provide to patients. In a separate publication, we describe these 24 clinicians’ perspectives on specific commonly used SRH online resources, including key considerations for adolescent populations and recommended improvements to future resources (in press). 46
Limitations and Strengths
This small qualitative study is not fully generalizable, especially as it was a convenience sample. Participants were adolescent SRH experts, so recommendations may be most applicable to SRH. However, the sensitive nature of SRH is also a strength. Most clinicians were sub-specialists, indicating generalists may need to adapt the strategies; still, the “mix and match” format offers flexibility for busy workflows. Finally, while clinicians endorsed these strategies, whether they use them in practice and their actual efficacy was not assessed.
Future Research
Future research should include direct observation of clinician communication and adolescent perceptions of recommended approaches. Trials of interventions aimed at improving clinician communication are also needed to determine the best ways of integrating these skills into medical training and continuing education curricula, ideally assessed with adolescent trust- and health-related outcomes.
Conclusions
As OHI increasingly shapes adolescent health beliefs and decision-making, clinicians need evidence-informed, trust-centered strategies to engage meaningfully with patient-identified information. These strategies are likely adaptable to broader pediatric and primary care settings, though clinicians in non-SRH settings may need to tailor approaches to their specific patient populations. Beyond individual practice, these findings highlight the need to integrate OHI communication skills into medical training and continuing education curricula. AAP and SAHM should consider developing formal guidance to support clinicians in navigating patient-identified OHI. Future efforts should evaluate whether these strategies improve adolescent trust and health outcomes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261437319 – Supplemental material for Clinician Recommendations for Discussing Online Health Information With Adolescents: A Qualitative Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319261437319 for Clinician Recommendations for Discussing Online Health Information With Adolescents: A Qualitative Study by Cambray Smith, Sarah Rebbeor, Melissa B. Gilkey, Betsy Sleath, Christopher M. Shea, Leah Frerichs and Bianca A. Allison in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We thank our participants for their insight shared during these interviews.
Abbreviations
AI: artificial intelligence
OHI: online health information
SRH: sexual and reproductive health
Ethical Considerations
The University of North Carolina at Chapel Hill IRB designated this study as Exempt (#24-2060).
Consent to Participate
All participants provided written informed consent through an electronic survey.
Author Contributions
Dr. Cambray Smith conceptualized and designed the study; curated the data; led the investigation, formal analyses, visualization, and validation processes; oversaw resources, software, supervision, and administration; secured funding; and drafted the initial manuscript and critically revised in response to coauthor feedback. Sarah Rebbeor contributed to investigation, formal analysis, validation, visualization, and provided critical review of the manuscript for important intellectual content. Drs. Melissa B. Gilkey, Betsy Sleath, and Christopher M. Shea contributed to conceptualization, methodology, validation, and critical review of the manuscript for important intellectual content. Drs. Leah Frerich and Bianca A. Allison contributed to conceptualization, formal analysis, funding acquisition, methodology, supervision, validation, visualization, and critical review of the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development under Award Number F30HD11645 (CS) and the National Center for Advancing Translational Science Award Number 1K12TR004416 (BAA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. CS is a recipient of the Gertrude B. Elion Mentored Medical Student Research Award of Triangle Community Foundation which provided support for this project. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders or the authors’ institutions. The funders had no role in the design or conduct of this project nor in decisions about reporting or publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Deidentified transcripts will be made available upon reasonable request after our final set of analyses (in development) is published. Requests should be submitted to
Related Publications
A research letter about perspectives toward online SRH resources for adolescents shared by these 24 participants is in press with by JMIR Pediatrics and Parenting titled:
During the preparation of this work the authors used Microsoft CoPilot based on GPT-4 architecture to decrease the word count after the full manuscript had been drafted and reviewed by multiple coauthors. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.