
Abstract
Objective
Adolescents frequently encounter contraceptive information online. Our objective was to evaluate the feasibility and pilot outcomes of a clinician training module designed to support counseling about online contraceptive information.
Methods
We co-developed a contraceptive counseling training with community advisory boards. We recruited adolescent-serving clinicians across North Carolina to participate in the virtual 3-hour training. One of the five modules was Supporting Teens with Online Information. To assess feasibility, acceptability, appropriateness, and pilot outcomes of this module, participants completed pre-, immediate post-, and 4-month-post-intervention measures about counseling about online contraceptive information and participated in a 4-month post-intervention interview. Analysis used a convergent mixed methods approach.
Results
35 clinicians participated, with 27 (77%) completing the 4-month interview. Immediately post-intervention, the module was perceived as acceptable (mean=4.6, SD 0.5), appropriate (4.7, 0.5), and feasible (4.6, 0.5) on a 5-point scale. Participants showed immediate and 4-month increases in knowledge, beliefs, self-efficacy, and self-reported counseling behaviors (p<0.05). Qualitative results indicated that participants liked the module and many reported adapting their counseling approach and/or providing new patient-facing resources. However, they faced barriers like time constraints and difficulty remaining abreast of social media information. They recommended inclusion of specific social media posts (versus overarching themes) and a more accessible resource toolkit.
Conclusions
This module demonstrated feasibility, with clinician-reported pilot outcomes showing increases at both immediate post-intervention and 4-month follow-up. This intervention is among the first developed to support person-centered counseling about online contraceptive information and warrants further investigation in a rigorous trial.
Keywords
1. Introduction
Adolescents need accurate contraceptive information to make values-congruent reproductive health decisions. 1 Young patients today navigate a complex health information environment shaped by the internet, particularly social media.2,3 A recent national survey found that nearly half of women aged 18-25 encountered contraception content on social media in the last year, 4 and a separate study found nearly 1 in 5 adolescents aged 15-17 reported similar exposure. 5
The content and quality of contraceptive information on social media varies widely. While social media has amplified patient voices (e.g., those reporting negative experiences of intrauterine device (IUD) insertion pain), 6 it has also fueled contraception misinformation.7–10 This is especially troubling given today’s increasingly restricted reproductive policy environment, which disproportionately affects minors. 11
Importantly, adolescents identify clinicians as their most preferred source of contraceptive information, 5 underscoring the importance of clinician engagement. While other areas of medicine have prioritized discussing online information on topics such as vaccination, 12 less is known about how to support clinicians in discussing digital sexual and reproductive health information with adolescent patients. Guidance in this area is emerging, 13 but few, if any, evidence-based interventions exist to improve these skills in the context of contraception.
1.1. Purpose
Our objective was to evaluate the feasibility and pilot outcomes of a clinician training module designed to support counseling about online contraceptive information.
2. Methods
2.1. Study design
We conducted a single-arm pilot feasibility study with secondary outcomes assessing preliminary signals, using a convergent mixed methods approach. A mixed methods approach was selected to account for respective strengths and limitations of quantitative and qualitative data, and thus to enhance the rigor and usefulness of our findings. 14
2.2. Curriculum co-development with community advisors
The co-development of our training has been described in detail elsewhere. 15 Briefly, we recruited three advisory boards of teens, caregivers, and clinicians (N=20). Over 5 months, we used human-centered design techniques 16 to co-develop a synchronous, virtual, interactive training for clinicians designed to support adolescent-centered contraceptive counseling, called Contraceptive Adolescent-Centered Counseling and Empowerment Skills for Success (ACCESS). The training consisted of 5 modules; the fourth, Supporting Teens with Online Information (“Online Information” module), is the focus of this manuscript. From study inception, this module was designed to be evaluated separately from the overarching program due to its unique topical focus. It was developed within the framework of the Theory of Planned Behavior, which posits that behavioral intentions—the proximal determinant of behavior—are shaped by attitudes, subjective norms, and perceived behavioral control.17,18
2.3. Participants and recruitment
Eligible participants were adolescent-serving clinicians (MD/DOs, NPs, or PAs) across North Carolina who were not involved in training development. Physicians who had not completed residency were excluded. Clinics across North Carolina in a variety of practice settings were asked to distribute recruitment materials to clinicians through email. Interested clinicians completed an eligibility and scheduling form. Those eligible who consented were grouped into four training sessions (7-11 participants each).
2.4. Intervention
In Fall 2024, participants attended the 3-hour virtual Contraceptive ACCESS training (Appendix A). For the 25-minute Online Information module, participants were in a main Zoom room for most of the session, with 9 minutes allotted in breakout rooms for an interactive case study. A physician and non-physician co-facilitated. During the session, participants received a digital resource toolkit with content aligned with each module, and after the session, we sent monthly post-session emails with refreshers and new resources, including those addressing online contraceptive information.
2.5. Ethics and IRB
The IRB determined the study to be minimal risk (#24-1207). All participants provided informed consent electronically.
2.6. Data collection
Surveys were administered via Qualtrics at three time points: baseline, immediate post-intervention, and 4-month follow-up. Participants were invited for 4-month follow-up interviews conducted and transcribed using Zoom. Two interviewers (CS, LB) completed a standardized memo template after each interview. Transcripts were cleaned and de-identified before analysis.
2.7. Survey development
The pre-survey included demographic questions and de novo measures on pilot outcomes of the Online Information module (i.e., knowledge, beliefs, self-efficacy, and behaviors) (Appendix B). Post-surveys immediately after the training contained the same pilot outcome measures as well as validated feasibility measures about the module, 19 and at 4 months, only the pilot outcome measures were collected.
2.8. Measures
For feasibility testing, we used the Acceptability of Implementation (AIM), Intervention Appropriateness Measure (IAM), and Feasibility of Implementation Measure (FIM). 19 The definitions of these constructs are: Acceptability (that a given innovation is “agreeable, palatable, or satisfactory”), Appropriateness (“perceived fit, relevance, or compatibility of the innovation…for a given practice setting; and/or perceived fit of the innovation to address a particular issue or problem”), and Feasibility (“the extent to which a new… innovation can be successfully used or carried out within a given… setting”). 20 Of note, each of these measures is designed to test the acceptability, appropriateness, and feasibility of the intervention itself, not necessarily the real-world implementation of its recommendations in practice.
Corresponding with the Theory of Planned Behavior,17,18 pilot outcomes assessed beliefs and self-efficacy (reflecting attitudes toward the behavior and perceived behavioral control, respectively), and behavioral intentions and self-reported behaviors. Knowledge was also assessed as an antecedent to attitude formation and informed decision-making, consistent with prior applications of the Theory of Planned Behavior in health research.21–23 We were unable to find preexisting pilot outcome measures related to clinicians supporting teens with online health information, and thus, we developed novel measures. The primary knowledge item assessed whether participants could correctly identify clinicians as adolescents’ most preferred source of contraceptive information (Appendix B). 5 Beliefs assessed whether participants believed they should ask patients about online contraceptive content; self-efficacy assessed confidence discussing online contraceptive information; and behavior items asked whether clinicians inquire about patients’ sources of contraceptive knowledge, including the internet and social media. Immediate post-intervention, clinicians were asked about behavioral intentions as they did not have time to enact changes yet. Four clinicians not involved with the study underwent cognitive interviews using a “think-aloud” technique 24 to give feedback to refine the measures’ understandability (IRB Exempt #24-2225).
2.9. Semi-structured interview guide
A semi-structured interview guide (Appendix C) adapted from implementation science constructs, 25 explored perceived training impact and barriers to clinical application. Questions aligned with the feasibility and pilot outcome domains assessed in the survey but were also open-ended so that participants could share additional perspectives beyond these domains. We refined the guide with expert feedback and mock interviews.
2.10. Analysis
2.10.1. Quantitative
Survey data were analyzed using R (v4.2.2). 26 Frequencies and means summarized demographics from the baseline survey. Acceptability, appropriateness, and feasibility scores 19 were summarized with means and standard deviations from the immediate post-intervention survey. For pilot outcome measures, we compared baseline data to immediate-post and baseline to 4-month follow-up data. For knowledge testing we evaluated changes in percentage correct using McNemar’s Chi-squared test to assess paired dichotomous data. 27 To examine differences in Likert scale means, we used paired Wilcoxon signed-rank test with a continuity correction. 28 To quantify the magnitude of change in Likert-scale outcomes, we calculated Cohen’s d z as the effect size for within-subjects comparisons, computed as the mean difference divided by the standard deviation of the difference scores. 29 Effect sizes were interpreted using Cohen’s conventions: small (d z =0.2), medium (d z =0.5), and large (d z =0.8). 29 Effect sizes are reported descriptively given the pilot nature of this study and use of single-item measures, which may restrict variance and should be interpreted with caution. Missing data were handled using complete case analysis. To assess potential attrition bias, we compared completers to non-completers on baseline demographic characteristics and outcome measures using Fisher’s exact test for categorical variables and t-tests for continuous variables.
2.10.2. Qualitative
Three research team members (CS, LB, BAA) reviewed recordings and memos to identify emerging themes. Using deductive categories from the interview guide and inductive emerging themes, a matrix was created, consistent with rapid qualitative thematic analysis.30,31 A primarily descriptive approach was used given the highly applied nature of the research question. 32 Transcript data were iteratively sorted by CS with review by BAA. Quotes were lightly edited for clarity.
2.10.3. Mixed methods
Quantitative and qualitative data were collected in parallel, then compared for convergence and divergence. 14 Joint displays of quantitative and qualitative findings were reviewed and interpreted by the research team to identify areas where findings mutually confirmed, expanded upon, or contradicted one another.
2.10.4. Reflexivity
The research team consisted of physicians, researchers, and trainees who believe that online health information presents both opportunities and challenges for adolescent reproductive health decision-making.
2.10.5. Reporting guidelines
We adhered to Standards for Reporting Qualitative Research (SRQR) 33 and Good Reporting of a Mixed Methods Study (GRAMMS) 34 available in Appendices D and E.
3. Results
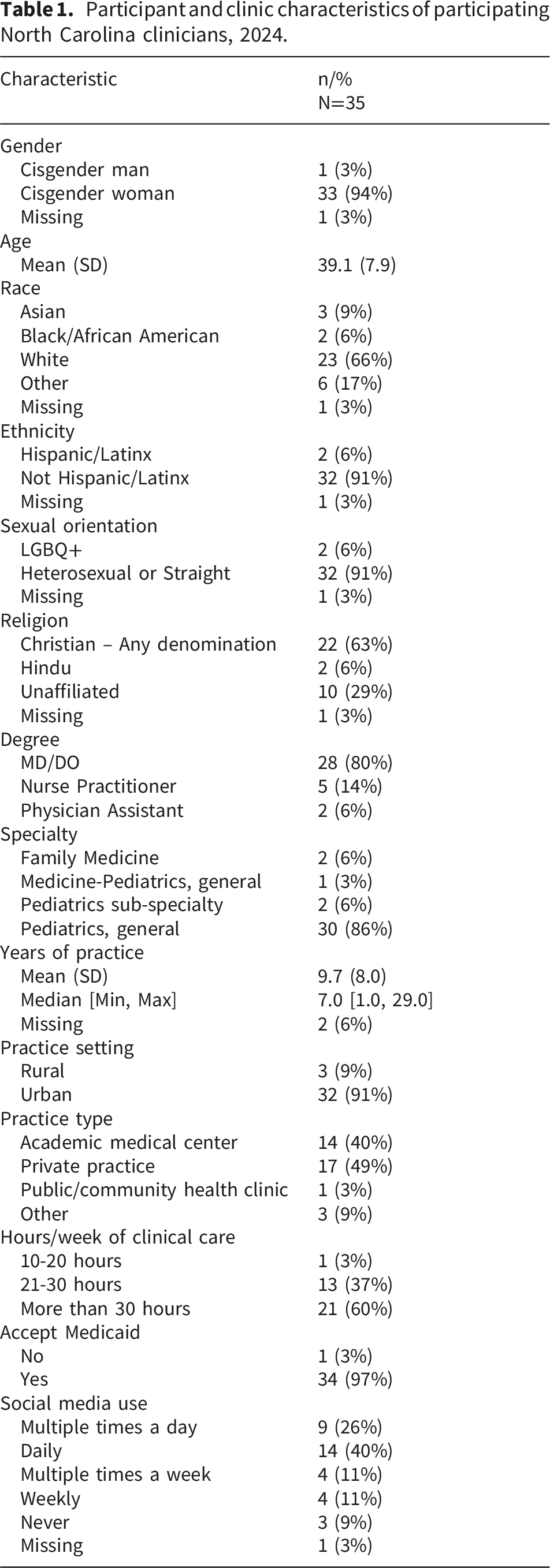
3.1. Demographics
Participant and clinic characteristics of participating North Carolina clinicians, 2024.
3.2. Pilot implementation outcomes
3.2.1. Acceptability
Acceptability was rated at a mean of 4.6/5 (SD 0.5). Qualitatively, nearly all participants liked the module, [e.g. “I really enjoyed it” [Participant 1 (P1)] and “I thought it was a great module” (P3)]. One participant described the emphasis on social media throughout the overall training as “a bit heavy” (P10) but also felt that it was an important topic to discuss. All respondents said that they would recommend the module to other clinicians [e.g. “Definitely. If you’re seeing adolescents in your clinic, I feel like you should be required to take this” (P5)].
3.2.2. Appropriateness
The module mean appropriateness score was 4.7/5 (SD 0.5). Many clinicians described the training as relevant to their patient population: “Oh, I feel like it hit it head on… I think the training was spot on for the needs of my patients” (P1). Several clinicians mentioned that the module was one of their main takeaways from the overall training, explaining “I thought that [module] was one of the more valuable parts… of the course. Because it applies not just to contraception, but to a myriad of other teen-based issues” (P20).
On the other hand, a few described it as less applicable than some of the other material in the overall training: “I think that [module] was out of everything one of the areas where… I was less likely to take that information and change the way that I do anything in the clinic. Good information, but maybe a little bit less applicable” (P25).
Some mentioned that it may be particularly helpful for clinicians who have been out of training for many years and/or don’t use social media, although several mentioned that it was also helpful for younger clinicians too.
3.2.3. Feasibility
Feasibility was rated at a mean of 4.6/5 (SD 0.5). Participants qualitatively described that participating in the module was feasible, but noted challenges implementing the recommendations in actual practice: “I think it was helpful, having the conversation about… social media, where they’re getting their information from, and that was very useful. Have I been able to incorporate [sharing] the good websites? Not as much as I would like” (P22).
3.2.4. Suggestions for future training
Participants suggested several improvements to the module. The first was incorporating specific existing social media content, as opposed to broad themes that cut across platforms: “[I’d like] examples of what they’re actually seeing...so maybe more… specific media examples of myths. Or even with the list of social media physicians…. like [an actual] clip of them” (P5).
About a third of participants asked for vetted social media accounts and other resources that they could share with adolescents, [e.g. “I apologize if I’ve missed any of this, but I think that would be super useful as a pediatrician who doesn’t do this all the time, having good… patient-accessible resources” (P11)]. These requested resources were included as part of the digital toolkit but participants appeared not to recall receiving them.
Participants who did utilize the training’s resource toolkit requested resources in formats that clinicians could more easily share with teens: “Maybe incorporating [trusted sources] into their visit packet, or having it posted somewhere in the clinic... Maybe like QR Codes [which] are really easy for kids to use if they’re already on their phones” (P7).
3.3. Intermediate outcomes
Across all outcome categories of knowledge, beliefs, self-efficacy, and behaviors, there were immediate and 4-month increases (Table 3; Appendix G).
3.3.1. Awareness, knowledge, and stated skills
The percentage of participants correctly identifying clinicians as adolescents’ most preferred contraceptive information source increased from 29% to 68% (p=0.003) immediate post-intervention with increases also observed at 4 months (48%, p=0.035).
Qualitatively, participants described greater awareness about what teens may be seeing online, as well as knowledge of new resources to share with patients. A few mentioned being surprised at clinicians being teens’ preferred knowledge source. I learned about how teenagers use social media to build their knowledge, but that they still rely on clinicians’ recommendations… I always felt like they would rely on social media more than us… but that was nice to know that they actually would listen to us. (P24)
Several described learning new counseling skills [e.g. “learning how to say the right words” to connect with teens about online information (P14)], but others described not being able to recall the details of the training beyond general encouragement to bring this up with teens, such as P5: “Oh, goodness! I don’t know if I remember specifically what strategies were included in that module.”
3.3.2. Beliefs
While baseline belief in the importance of discussing online contraceptive information with patients was high, participants still demonstrated increases in their ratings at both time points (4.1 to 4.8 post-intervention, p<0.001; d z =0.84, 4.5 at follow-up, p=0.012; dz=0.52), reflecting large and medium effect sizes, respectively.
Qualitatively, participants described believing that educating patients about online health information is increasingly important for pediatric clinical care broadly. I definitely think social media education in general is incredibly important… There are these really cool QR code signs that you can scan and it gives parents and physicians information about each type of social media and what type of information… it gets, is it videos, is it posts, is it tweets... We’ve made handouts that go into our after-visit summaries. Again... social media and healthcare education is very important. (P6)
Additionally, many clinicians described discussing online health information as a mechanism to connect with teens and as increasingly essential to adolescent-friendly care. I think this is a fact, if you’re going to take care of adolescents that they’re going to get information from online, so the better we are informed in knowing that that’s where they’re going to get information the better we can do it… making sure that they are well informed. (P18)
Participants differed regarding whether they believed it mattered clinically if patients obtained information online or elsewhere, with a few describing the source (e.g. social media) as less important than the content, [e.g. “I usually try to just ask them… what they know about something, because I find that that’s more effective than asking them where they get their information” (P13)]. This contrasted with other clinicians: It is interesting to ask where their information came from. If it’s from personal experience that’s going to lead you in one direction, if it’s from a family member…, that’s going lead you in another direction. If it’s from an online source… that’s going lead you in another direction. (P20)
Finally, a few clinicians said that this was not yet a priority for their clinic but anticipated it might be in the future: “I don’t think it’s top priority right now, but I do think it will be because we’re starting to see… different viewpoints emerging right now. So it probably will be” (P15).
3.3.3. Self-efficacy
At baseline, confidence discussing contraceptive information seen on social media was 2.9 and increased to 4.2 post intervention (p<0.001, d z =1.51, very large effect), with a large effect observed at 4-month follow-up (4.0, p<0.001, d z =0.89).
While a few participants qualitatively described themselves as having high or low confidence, most described themselves as moderately confident when discussing online information about contraception. Participants described low confidence as stemming from the wide array of online information available to patients, including content that clinicians may not feel prepared to counsel about. I still think it can be pretty intimidating, because there’s a million different resources, and even they mostly go to TikTok, what you're seeing on TikTok could be anywhere from another physician to a Kardashian giving their input on things so I still get a little bit intimidated, because there is just such a wide variety of things that you can find on there. (P16)
Participants described a mixed relationship between personal social media use and confidence (i.e. some thought it might help with confidence, others did not). Those who were on social media, however, described feeling empathy for patients and families who may be confused and overwhelmed by online information: “I can see how overwhelming it is for parents to see this, or read that, or see this TikTok on how this is bad for your kid… I get it on my feeds too. If I had no medical background, I’m sure I’d be overwhelmed” (P23).
3.3.4. Intentions and behaviors
In immediate post-testing, participants’ intention to ask about adolescent contraceptive information sources and the role of social media in patients’ contraceptive decision-making increased from baseline (3.1 to 4.8, p<0.001, d z =1.27, and 2.7 to 4.6, p<0.001, d z =1.68, respectively), both with very large effects. Compared to baseline, at 4-month follow-up, participants reported higher levels of enacting these counseling behaviors (3.1 to 3.9, p<0.001, d z =0.77, and 2.7 to 3.6, p=0.001, d z =0.75, respectively), both reflecting medium-large effects.
Qualitatively, participants described two main areas of reported behavior change following the training. The first was more consistently asking patients about their information sources, including specific probes about social media: “[The training] definitely has contributed. I definitely talk more about social media in general… A few years ago it was more like, oh what are your friends saying, now it’s like, okay what’s TikTok saying” (P6).
The second was provision of new patient-facing resources, which most often were based off the online resource toolkit provided as part of the intervention: “[Now] I bring in that binder [that my colleagues and I made from the toolkit] and say, ‘Hey, you mentioned that… some of your information comes from social media. These are really good accounts that have information that is accurate’” (P3).
Several clinicians stated that they already routinely discussed online information with patients so did not change behaviors in response to the module. Others who did not report changing behaviors following the module shared that they had thought about and were open to discussing it more but would only prioritize discussing online health information if the conversation were patient-initiated.
3.4. Barriers and facilitators to implementation of training recommendations
Clinicians described several barriers and facilitators to applying the training’s suggestions (Table 4). Time constraints were the main barrier: “The nature is there’s always so much to talk about, and not enough time” (P15). Staying up-to-date on online information was also a challenge: “It’s hard for us to do all our own research, not only on what’s medically relevant, but also now socially, medically relevant” (P19).
Facilitators included receiving specific resources [“Oh, [it was helpful] that they gave us specific Instagram handles, like they weren’t like, oh, there’s some really good doctors out there” (P2)], as well as integration into routine counseling topics (e.g. screentime, asking about peer behaviors). I think [this conversation] fits in perfectly [in my workflow], because we always talk about social media usage… we might talk about how much they are on social media and then I can follow up and be like, what sites are you on, we might talk about inappropriate texts or sexting and things like that, so it segues pretty easily. (P8)
3.5. Mixed methods integration
Mixed methods synthesis of pilot implementation findings among North Carolina clinicians, 2024-2025.

aEvaluated immediately post-intervention with N=35 clinicians.
bCollected 4-months post-intervention in interviews with 27 clinicians. Initial data collection before and immediately after the intervention took place in Fall 2024 and follow-up data collection was completed in Spring 2025.
cAcceptability of Implementation Measure (Weiner et al. 2017).
dIntervention Appropriateness Measure (Weiner et al. 2017).
eFeasibility of Implementation Measure (Weiner et al. 2017).
fA list of social media accounts similar to what the participant described here was included as part of the online resource toolkit.
Mixed methods synthesis of preliminary efficacy outcomes among North Carolina clinicians, 2024-2025.

*P-value <0.05.
aStandard deviations included in main text and in Appendix G.
bCollected 4-months post-intervention in interviews with 27 clinicians. The intervention took place in Fall 2024 and follow-up data were collected in Spring 2025.
cParticipants were asked about intended behaviors immediate post-training, as they did not have time to enact relevant behavioral changes.
However, two areas of divergence warrant attention. First, while knowledge scores improved significantly post-intervention (29% to 68%), qualitative data revealed that several participants could not recall specific recommended strategies from the module at the follow-up interview, despite quantitative gains observed at 4-month follow-up (48%). This suggests that knowledge gains related to a specific fact (i.e., a multiple-choice question about preferred contraceptive information sources) may differ from broader multi-step skill-based knowledge which requires more challenging recall and integration of multiple concepts.
Barriers and facilitators of incorporating discussion of online contraceptive information into counseling among North Carolina clinicians, 2025.

aData were collected 4 months post-intervention during interviews with 27 clinicians.
4. Discussion
4.1. Summary
This mixed methods pilot tested the Supporting Teens with Online Information module designed to support clinician counseling about online contraceptive information. The training demonstrated acceptability, appropriateness, and feasibility, with pilot outcomes showing increases at both immediate post-intervention and 4-month follow-up. To our knowledge, this is one of the first interventions aimed at supporting clinical dialogue on this topic. Participants also suggested areas for improvement (e.g., more specificity in the curriculum, more accessible patient-facing resources) in follow-up interviews. At 4-month follow-up, many participants did not recall receiving the patient-facing resources during the training, underscoring a need for more explicit integration of these resources into the training.
4.2. Integration with literature
Clinician trainings with practical components (i.e. opportunities to practice skills) yield better outcomes than didactic-only approaches. 35 Our training’s use of a case study during breakout rooms offered participants an opportunity to apply the suggested communication skills in real time and is recommended as a standard component in future trainings. Although this pilot did not assess direct patient-level outcomes, previous research shows that trainings that change clinician knowledge and skills can result in small but significant improvements in patient health behaviors, 35 suggesting this module may have downstream potential to positively influence patient health behaviors, though this remains to be tested. More robust simulation-based clinician trainings can be another high-impact way of improving counseling skills; however, these can be resource-intensive. 36 Emerging uses of artificial intelligence as simulated patients may offer scalable, cost-effective practice opportunities. 36 The divergence between quantitative knowledge gains and qualitative reports of difficulty recalling specific strategies at follow-up further underscores the importance of reinforcement mechanisms, such as the monthly follow-up emails provided in the study, and suggests that future iterations should incorporate repeated practice opportunities to support skill development and retention. 37 Multi-item measurement of knowledge will also provide better insight as to the degree to which information is being retained.38,39
Although the module demonstrated high feasibility as assessed by the FIM—which is designed to evaluate the ease of direct participate in an intervention 19 —it is important to distinguish between the feasibility of participating in a brief training and the feasibility of implementing recommendations in busy clinical practice. While most participants found discussions of online health information to be an increasingly important aspect of their clinical counseling, some emphasized the challenge of keeping pace with a rapidly changing online landscape. Given adolescents’ complex relationship with online health information—including sexual health information 40 —they need better guidance to successfully navigate online information and make values-aligned decisions about their health.2,41 Our participants noted that sharing specific vetted resources or social media accounts was valuable (e.g. Bedsider, Planned Parenthood).42,43 Professional organizations could support clinicians by curating a list of credible, accurate social media accounts or producing their own social media content to engage patients directly.
4.3. Limitations and strengths
This pilot study is limited by being a single-arm design that was not designed to assess changes in clinical behavior or patient-reported outcomes. This study was further limited by the use of novel single-item self-reported measures of knowledge, beliefs, self-efficacy, and behaviors; as single-item measures preclude calculation of internal consistency (e.g., Cronbach’s alpha), psychometric evaluation was not possible and findings should be interpreted with caution. Attrition analyses revealed that non-completers had significantly fewer years of practice (mean 5.7 vs. 10.6 years), suggesting findings may be more generalizable to more experienced clinicians who are further removed from formal training. Clinicians who agreed to participate in this training may systematically differ from those who did not participate regarding beliefs, motivation, or self-efficacy. Additionally, our sample was homogenous and not demographically representative of national pediatrician trends; for example, women clinicians were over-represented, 44 which may influence our results. Finally, social desirability bias may affect our findings. 45
Strengths of our statewide study include community-engaged co-development of the training, collection of longitudinal outcomes, and a mixed methods approach. This is a novel intervention focused on clinician-patient conversations about online contraceptive information, and it was feasible, acceptable, and appropriate.
4.4. Future research
These pilot data set the groundwork for a future randomized controlled trial. An appropriate comparator would be either a waitlist control or an active comparator, such as a contraceptive counseling training without the Online Information module, which would allow isolation of the module’s specific contribution to clinician outcomes. A future trial should incorporate multi-item validated outcome measures, a larger and more representative clinician sample, and patient-reported outcomes such as adolescent perceptions of clinician communication and contraceptive decision-making autonomy. The observed changes in beliefs, self-efficacy, and behavioral intentions align with the Theory of Planned Behavior’s posited pathway toward behavior change,17,18 providing a theoretically grounded mechanism for further investigation in future trials.
4.5. Future adaptations
While the Online Information module is currently embedded in a 3-hour, synchronous training, it could be adapted into a standalone training that could be delivered asynchronously to a larger number of clinicians, thus expanding the reach of this intervention. Future adaptations might also target broader populations (e.g. adult contraceptive users) or different clinical topics, such as discussing social media content related to disordered eating.4,46 Finally, helping patients navigate online content—especially amidst vast amounts of misinformation—requires not just clinician action, but coordinated efforts from professional societies and public health agencies.47,48
5. Conclusion
This training module pilot test demonstrated feasibility, with clinician-reported outcomes of knowledge, beliefs, self-efficacy, and self-reported behaviors showing increases at both immediate post-intervention and 4-month follow up. Supporting patients in navigating complex online health information environments is an emerging clinical and public health priority, and this intervention offers a feasible model worthy of further investigation.
Supplemental material
Supplemental material - Feasibility and pilot outcomes of a novel training to help clinicians counsel adolescents about online contraceptive information
Supplemental material for Feasibility and pilot outcomes of a novel training to help clinicians counsel adolescents about online contraceptive information by Cambray Smith, PhD, Leah Frerichs, PhD, Hailey Leiva, MSW, Lucy Burwell, Melissa Gilkey, PhD, Christopher M. Shea, PhD, Betsy Sleath, PhD, Carol Golin, MD, Samantha Schilling, MD, MSHP, Bianca Allison, MD, MPH in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank their teen, caregiver, and clinician advisory boards for co-developing this training. They also thank the Odum Institute, Yumei Yang, and Feng-Chang Lin, PhD for support with statistical analyses, Marcella Boynton, PhD for supporting development of the de novo preliminary efficacy measures and Anahita Gupta and Emma Brockman for assistance with transcript cleaning.
Ethical considerations
The IRB determined the study to be minimal risk (#24-1207). All participants provided informed consent electronically.
Author contributions
All authors meet criteria for authorship. Contributions are described below.
Conceptualization: CS, LF, BAA.
Methodology: CS, LF, MBG, CMS, BS, CG, SS, BAA.
Validation: all authors.
Formal analysis: CS, LF, BAA.
Investigation: CS, HL, LB, BAA.
Resources: CS, BAA.
Data curation: CS, HL, LB.
Writing – original draft: CS.
Writing – review & editing: all authors.
Visualization: CS, LF, BAA.
Supervision: LF, BAA.
Project administration: CS, HL, LB, BAA.
Funding acquisition: CS, LF, BAA.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cambray Smith is supported by 1F30HD116454 from the National Institutes of Child Health and Human Development and is a recipient of the Gertrude B. Elion Mentored Medical Student Research Award of Triangle Community Foundation. Bianca A. Allison was partially supported by the Doris Duke Charitable Foundation [grant number 2020143], and the National Center for Advancing Translational Science (NCATS), National Institutes of Health [1K12TR004416-01]. Carol Golin was partially supported by the University of North Carolina at Chapel Hill Center for AIDS Research [P30 AI50410]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funders had no role in data collection, interpretation, or reporting.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized transcripts and analytical memos are available upon request to the corresponding author.
Prior presentations
This project has been presented as works-in-progress at the 2025 Society of Adolescent Health and Medicine meeting and the 2025 Psychosocial Workshop prior to the Population Association of America meeting.
Preprints
This manuscript has not been posted on any preprint server.
Prior publication
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.