
Abstract
Introduction
Personality disorders (PDs) can have a significant impact on psychosocial function, and given the incidence and prevalence of comorbid mood and anxiety disorders, clinicians should be aware of the clinical combination. Comorbid personality disorder with depression was associated with a 2 times higher risk of a poor depression outcome relative to those without comorbid personality disorders—a finding that remained consistent for multiple treatment modalities besides electroconvulsive therapy. 1
General personality disorder is subdivided into 3 distinct clusters (A, B, and C), each of which is further divided into 3 or more individual disorders. 2 Cluster A includes paranoid, schizoid, and schizotypal personality disorders. Cluster B includes antisocial, histrionic, narcissistic, and borderline personality disorders. Finally, cluster C diagnoses include dependent, obsessive-compulsive, and avoidant personality disorders. In 2007, the overall prevalence of any PD among US adults was estimated to be around 9.1%. 3
Past studies have shown that the presence of any PD diagnosis has been associated with higher rates of persistent depression and/or decreased remission rates. Shea et al 4 found that patients with diagnosed PD had worse social functioning and increased residual depressive symptoms relative to enrolled patients without comorbid PD. Hardy et al 5 demonstrated that patients diagnosed with cluster C PD had more severe depressive symptomatology at baseline and showed less improvement in response to brief psychotherapy compared with individuals without a PD diagnosis. Cluster B PD have also been associated with poorer mood disorder outcomes, with some studies showing that these patients take a longer time to show reduction in Hamilton Depression Rating Scales following routine treatment with a combination of antidepressant medications and psychosocial interventions. 6 A prospective study in 2007 did demonstrate that cluster B and C PD had a negative impact on depression outcomes. 7
Though the findings above support the general conclusion that having any PD can negatively affect depression outcomes, very few studies have qualitatively or quantitatively compared outcomes among the different personality clusters within a collaborative care management (CCM) model for depression treatment. CCM is a systematic attempt to provide holistic and integrated care for patients with chronic psychiatric conditions within a primary care setting. It involves integration of support and expertise from care managers and consultant psychiatrists, with primary care physician oversight and direction.8,9 At our institution, CCM has been found to be more effective in treating depression compared to usual primary care practice, from both a clinical and economic standpoint.10,11 However, the presence of comorbid conditions has been found to negatively affect 6-month depression outcomes within CCM, including severe anxiety, abnormal screening for bipolar symptomology, posttraumatic stress disorder, and the presence of any PD.12-14
The purpose of the current study was to compare 6-month depression outcomes between cluster A, cluster B, and cluster C patients within CCM relative to CCM patients without a PD diagnosis, in order to identify specific PD groups that might confer a worse prognosis. Given that cluster B and cluster C diagnoses have traditionally been associated with the greatest level of mood instability, we specifically hypothesize that having a cluster B or cluster C personality disorder will also negatively affect 6-month depression outcomes after enrollment into CCM program.
Methods
This study retrospectively reviewed the electronic medical records (EMRs) from March 1, 2008 through June 30, 2015 of a cohort of 2826 primary care patients who were enrolled in our CCM and included in the depression registry for the presence of a clinical diagnosis PD. Adult (ages of 18 years and older) patients who previously authorized EMR research were eligible for inclusion in the study. To be included in our depression registry, the patients need to have been diagnosed with major depressive disorder and a patient of one of our primary care providers (PCPs). The PCPs were members of the Department of Family Medicine, Division of Primary Care Internal Medicine, or Division of Community Pediatrics and Adolescent Medicine of Mayo Clinic in Rochester, Minnesota USA. The practice has approximately 110 000 adult patients and is 50% community-based and 50% clinic employees and dependents population.
Variables included in the study included age, gender, marital status (married or not), race (white or not), initial Patient Health Questionnaire–9 (PHQ-9), 15 Generalized Anxiety Disorder 7-item Questionnaire (GAD-7), 16 Mood Disorders Questionnaire (MDQ), 17 and the clinical depression diagnosis (first episode or recurrent major depressive disorder or dysthymia). The MDQ was scored as negative (less than 7 positives for question 1 and both questions 2 and 3 with a negative response) or as abnormal (any combination, including all, of positive criteria were coded). The independent variable was the presence or absence of a diagnosis of a PD. The diagnosis of PD was determined by reviewing for the presence of a clinical diagnosis using the ICD-9 (International Classification of Diseases, Ninth Revision) code 301.X, identified either before or during the study period. Some patients came in with a previous diagnosis of a personality disorder while others were diagnosed within our CCM framework. If present, the PD was categorized into the appropriate cluster (A, B, or C), with the diagnosis of “other PD” placed in the “A” cluster. The outcome variable was the 6-month follow-up PHQ-9 score. Six-month outcomes of remission and persistent depressive symptoms (PDS) were defined by a PHQ-9 score of <5 and ≥10, respectively. 18
MedCalc Software (www.medcalc.org, version 17.11.5) was used for statistical analysis with 2-tailed P values <.05 considered significant. For comparison between groups of continuous variables, Mann-Whitney testing was used due to nonnormal distributions. Categorical variables were evaluated with chi-square testing. Multiple logistic regression modeling, while controlling for all the other study variables, was performed for the association between predictor variables and outcomes. The study was reviewed and approved by our institutional review board.
Results
Of the 2826 patients in the study cohort, 216 (7.6%) had a documented diagnosis of a PD. A majority of these patients (N = 122) were cluster B PD (antisocial, histrionic, narcissistic, or borderline PD). Cluster B PD patients were noted to be significantly younger (33.6 vs 42.5 years, P < .001) than patients without a PD diagnosis; as well as the cluster A/other and cluster C PD patients (Table 1). PD patients were more likely to have a diagnosis of recurrent major depression than the non-PD group (56.6% to 65.7% vs 41.3%, P < .001). Cluster B patients were much less likely to be married than the cluster A/other, cluster C, or non-PD patients (29.5% vs 42.4%, 48.6%, and 55.6%, respectively, P < .001). All PD cluster groups had an increased initial PHQ-9 compared with the non-PD group (17, 18, and 17 vs 15, respectively, P < .01 to P < .001). Initial GAD-7 scores in the PD cluster groups were also increased at a rate for severe anxiety symptoms (at approximately 48%) compared to the non-PD group of 30.9% (P < .001). Abnormal baseline MDQ scores were noted increased in the PD cluster groups at 28.6% to 39.3% compared with 17.5% in the non-PD group (P < .001). There were no statistical differences between the cluster PD groups and non-PD group with regard to gender or race.
Comparison of Depressed Primary Care Patients Enrolled in Collaborative Care Management by Personality Disorder (PD) Cluster or No Personality Disorder, by Study Variable (N = 2826).
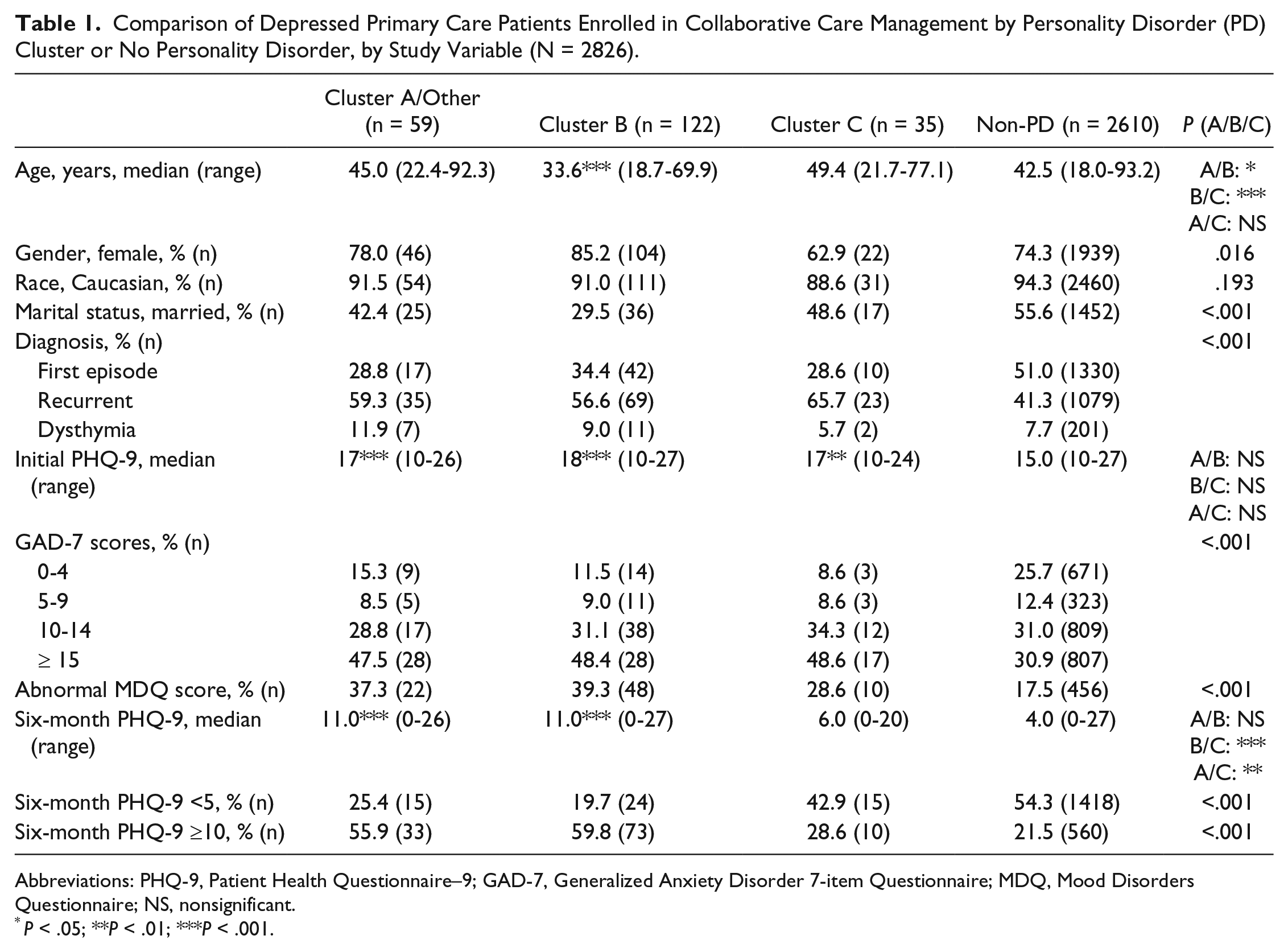
Abbreviations: PHQ-9, Patient Health Questionnaire–9; GAD-7, Generalized Anxiety Disorder 7-item Questionnaire; MDQ, Mood Disorders Questionnaire; NS, nonsignificant.
P < .05; **P < .01; ***P < .001.
Outcomes at 6 months, as measured by PHQ-9 scores, demonstrated no significant difference in mean score between the cluster C patients and non-PD patients (6 vs 4). However, both cluster A and cluster B PD groups had a mean 6-month PHQ-9 score of 11 (P < .001 compared with non-PD group). The percentage of patients who has achieved remission at 6 months (PHQ-9 score <5) was 54.3% in the non-PD group but 25.4% in the cluster A/other group and 19.7% in the cluster B group, P < .001). The percentage of patients who remained with PDS at 6 months (PHQ-9 ≥10) was 21.5% in the non-PD group and 55.9% in the cluster A/other group and 59.8% in the cluster B group, P < .001.
With the non-PD group of patients in CCM as the referent group, the cluster A/other group (adjusted odds ratio [AOR] = 0.383, 95% CI 0.209-0.702, P = .002) and cluster B group (AOR = 0.295, 95% CI 0.185-0.470, P < .001) were less likely to be in remission at 6 months, while controlling for all other study variables (Table 2). Cluster C patients were not statistically different in odds ratio from the non-PD group for remission at 6 months.
Adjusted Odds Ratios for Remission at 6 Months (PHQ-9 <5) in Collaborative Care Management by Variable (N = 2825).

Abbreviations: PHQ-9, Patient Health Questionnaire–9; GAD-7, Generalized Anxiety Disorder 7-item Questionnaire; MDQ, Mood Disorders Questionnaire; ROC, receiver operating characteristic.
Similarly, for PDS at 6 months, cluster A/other (AOR = 3.347, 95% CI 1.932-5.798, P < .001) and B (AOR = 3.638, 95% CI 2.447-5.408, P < .001) had worse outcomes than the non-PD group (Table 3). Again, the cluster C group was not seen as statistically different from the referent group.
Adjusted Odds Ratio for Persistent Depressive Symptoms (PHQ-9 ≥10) at 6 Months in Collaborative Care Management by Variable (N = 2825).

Abbreviations: PHQ-9, Patient Health Questionnaire–9; GAD-7: Generalized Anxiety Disorder 7-item Questionnaire; MDQ, Mood Disorders Questionnaire; ROC, receiver operating characteristic.
Discussion
Our study revealed that patients with comorbid Cluster B personality disorders had the lowest likelihood of remission at 6 months within the CCM model and the highest odds of having PDS. Several important characteristics and traits of this subpopulation may contribute to these poor outcomes. Cluster B patients (including antisocial, borderline, histrionic, and narcissistic PD patients) are more likely to report a greater degree of psychosocial distress and previous traumatic or life-threatening events than the general population.19,20 Indeed, the association between childhood or multiple traumatic events and chronic depression has been well established in the literature.21,22
Cluster B patients might also have genetic distinctions that play a significant role in altering mood disorder outcomes. Jacob et al 23 found that allelic variation in the polymorphic region of the monoamine oxidase A gene was significantly associated with the presence of cluster B personality disorders but not with cluster C disorders. These genetic variants can impact levels of anxiety, aggression, and addiction-related behavior, all of which can subsequently impact mood stability. Also, cluster B PD, based on self-report questionnaires and interview data for 2800 twins from the Norwegian Institute of Public Health Twin Panel, Torgersen et al 24 found that the heritability of Cluster B PD was in the upper range for mental disorders. Also, depressed patients who have a comorbid cluster B PD may respond differently to some of the common antidepressant medications prescribed. 25 Thus, for cluster B patents, the power of genetically driven personality traits and their effects on mood might overwhelm the capacity of interventions in CCM to effect long-term, lasting change. Ultimately, all these biological factors suggest a potential fundamental difference in the way cluster B patients physiologically process stressors and respond to interventions, both of which can translate to the poorer mood outcomes seen in this cohort.
Interestingly, in our study, having a cluster C diagnosis was not associated with a significantly lower likelihood of remission at 6 months (AOR = 0.83; 95% CI 0.42-1.65). Cluster C patents also did not have significantly increased odds of experiencing PDS at 6-month follow-up (AOR = 0.95; 95% CI 0.45-2.00). This was in contrast to individual studies in the literature that have showed an opposite trend.5,7,26
The presence of a cluster A/nonspecified PD diagnosis was associated with a 62% lower likelihood of remission at 6 months (AOR = 0.38; 95% CI 0.20-0.70). Increased odds of having PDS at 6-month follow-up were also seen with cluster A/nonspecified PD patients (AOR = 3.35; 95% CI 1.92-5.84). Interestingly, this is one of the first studies to indicate that non–cluster B and C patients might also be at higher risk for poorer mood outcomes. However, it is important to consider 2 potential explanations for these findings. First, the poorer outcomes of this group might be artificially produced by inclusion of patients with nonspecific PD diagnoses. Misdiagnosis of not otherwise specified (NOS) patients who really belong in a higher risk group such as cluster B is a potential risk for this cohort, especially because of their unclear and mixed presentations with regard to DSM-5 PD criteria. However, another plausible explanation is that cluster A or NOS patients have specific features that actually do make them more prone to poorer mood outcomes. Candrian et al 27 found that depressed patients with comorbid cluster A PD had a greater tendency to perceive stress after antidepressant treatment, even after controlling for baseline depression severity and demographic variables.
Given that patients with comorbid cluster B PD have poorer outcomes within CCM, it is important to consider specific interventions and therapeutic strategies that can be targeted to this specific group. Furthermore, conscious attention to the way practitioners interact with PD patients both within CCM and in these additional PD-centered programs is warranted. Of prime importance in preserving the patient-provider relationship is the recommendation that motivational interviewing and solution-based problem-solving techniques be used to help cope with problematic patient behaviors and attitudes that are driven by an underlying PD.
This study has some limitations to note. In our study, the diagnosis of a PD was established by the prevalence of a diagnostic code in the EMR. Traditionally, a structured clinical interview by a skilled clinician is used to diagnose a personality disorder, but no “gold standard” exists, and there is often little agreement between assessment instruments on the criteria for a specific personality disorder. 28 This makes classification of the exact personality disorder difficult. Additionally, EMR coding has often shown inaccuracies in specific subcategories29,30 and is regarded as less sensitive than structured clinical interviews. 31 These facts may explain the lower prevalence of PD in our sample (7.6% vs 9.1%). It is important to note that the CCM framework includes regular psychiatrist oversight, and thus any diagnoses of PD that were made by our CCM practice were well supported clinically. However, it was not necessarily possible or feasible for us to determine how a PD diagnosis was made if patients entered our program with the diagnosis. Thus, the current study must assume that the original PD diagnoses were made using clinically appropriate criteria for the different PD subtypes, regardless of the specific type of practitioner making the diagnosis. Given that PDs are diagnosed in practice with highly personalized clinical interviews and since the current study is retrospective in nature, the use of specific ICD codes was the most reasonable way for us to objectively identify a personality disorder within the constructs of our study.
Additionally, there may be pollution of the cluster A/Other group with patients who actually have a cluster B or C personality disorder. The low number of actual cluster A patients and this pollution of their sample with NOS coded PD may explain why the cluster A/Other group has outcomes similar to the cluster B group. Of note, the current DSM-based classification of PD serves as a limitation given that cluster A, cluster B, and cluster C designations are not well substantiated and persist in practice through habitual usage, indistinct boundaries between categories, and feasibility for research (ie, analyzing 3 clusters as opposed to numerous disorders). 32 Future studies should explore dimensional models of psychopathological syndrome classification, which address categorical blending and diagnostic instability, 33 to provide a comprehensive and empirical understanding of the comorbidity of PD and major depression.
Sample size for the cluster A/other group was low, which prevented meaningful statistical analysis of cluster A patients alone. Future research should include prospective trials evaluating the effectiveness of formalized psychosocial programs in improving mood outcomes in depressed patients with comorbid cluster B PDs. Additional treatment studies examining the comparative effectiveness of different pharmacological and nonpharmacological regimens in patients with comorbid depression and PD are also warranted to further individualize our therapeutic approaches for these patients.
Additional future research could be applied to diagnosing PD in the primary care setting. Our studied population had a lower percentage of diagnosed PD (7.6% vs 9.1%) than estimated prevalence. Previously authors have described the lack of recognition of PDs among PCPs in their patient population. 34 As treatment of comorbid mood disorders is complicated by PDs, it is expected that recognition of PDs and disclosure of diagnosis to consulting psychiatrists in the CCM setting could lead to improved treatment and remission.
Conclusions
Out of the 3 clusters, the presence of a cluster B PD diagnosis was most significantly associated with poorer depression outcomes at 6-month follow-up, including reduced remission rates and increased risk for PDS. The cluster A/nonspecified PD group also showed poor outcomes; however, the heterogeneity of this subgroup with regard to PD features must be noted. The development of novel targeted interventions for at-risk clusters may be warranted to improve outcomes of these patients within the CCM model of care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.