
Abstract
Introduction:
Primary care is foundational to health, but provider shortages impact access. In the Veterans Health Administration (VHA), Clinical Resource Hubs (CRH) provide remote clinicians to alleviate short term staffing gaps.
Methods:
A longitudinal analysis of primary care clinics from October 1, 2020, through September 30, 2024, was conducted. CRH user clinics were those with ≥10 CRH visits/month in 2 consecutive months. A time-varying measure of minimal threshold CRH use (ie, ≥10 CRH visits/month) was also constructed. Outcomes were measured monthly, including established and new patient wait time, third next available appointment (ie, average time to the third open appointment in provider schedule), timely care, and an indicator that 80% of new patients were seen within 20 days. Using a within-between model framework, generalized linear mixed models with robust standard errors assessed the association between CRH use and access to care.
Results:
Overall, 37.1% of VHA primary care clinics (N = 366) were CRH users In adjusted models, clinics meeting the time-varying minimal threshold for CRH use versus not was associated with an increase in established patient wait time (β = .35 day, SE = 0.07, P < .001) and new patient wait time (β = .69 day, SE = 0.20, P < .001), and a decrease in timely care (β = −1.40%, SE = 0.21, P < .001).
Conclusions:
When CRH was engaged, clinics had marginally longer wait times. Though CRHs have provided remote staffing, additional efficiencies may be needed to close access gaps.
Introduction
The Veterans Health Administration (VHA) provides care to over 9 million veterans in the United States and its territories. 1 Primary care is a foundational service. Primary care providers play a crucial role in care coordination for complex patients and primary care access has been shown to improve health outcomes, lower mortality rates, and facilitate subspecialty access.2-4 To provide adequate and timely care, primary care providers need to be available; however, VHA faces a provider shortage.5-8 These provider shortages will likely worsen as practicing physicians retire,9-11 fewer providers choose primary care as their specialty, 12 and the general population ages increasing demand. Additionally, rural areas have difficulty recruiting and retaining providers.13,14
VHA piloted the Virtual Integrated Multisite Patient Aligned Care Teams (V-IMPACT) program from 2013 to 2018 to deliver primary care when VHA sites experienced gaps in primary care staffing, 15 with care predominantly delivered using clinic-to-clinic synchronous telemedicine. Research has shown V-IMPACT delivered high quality diabetes care similar to that delivered in-person, 16 increased telehealth primary care visits, 17 and had higher penetration rates among rural veterans and sites. 15 From this program, the national Clinical Resource Hub (CRH) program originated in 2019. 18 Like V-IMPACT, the CRH program utilizes a hub-and-spoke model; it is organized within 18 Veterans Integrated Service Networks (VISN; geographic regions that implement national policy and manage VA medical centers) to provide care to outlying clinics during staffing gaps, but covered services expanded to include mental health and specialty providers. VA medical centers or community-based outpatient clinics request coverage based on the lack of staffing or increasing veteran volumes, while CRH leaders prioritize fulfillment based on veteran need and CRH staff availability. 18 This organization allows program flexibility responsive to facility needs. The primary program goal is to increase or maintain access to care through contingency staffing (ie, provision of remote staff when existing staff are insufficient) with an emphasis on clinics that are most underserved. 19
Preliminary data prior to the COVID-19 pandemic showed no significant differences in wait times when comparing clinics implementing CRH versus not. 20 This initial analysis included 80 CRH user clinics, however the program has since engaged fourfold as many clinics. Further, the COVID-19 pandemic led to expanded telehealth options.21,22 This shift has persisted with video-based visits accounting for 11% of all VHA outpatient care.23,24
The objective of this study was to longitudinally evaluate the association between CRH utilization and primary care access through the assessment of primary care wait times.
Methods
Study Design
A time series analysis using a retrospective observational cohort of clinics using (CRH user) and not using CRH (control clinics) from October 1, 2020, through September 30, 2024, was conducted. CRH user clinics were those with ≥10 primary care CRH visits per month for 2 consecutive months. Control clinics were those not meeting this criterion. This cutoff was selected to balance meaningful engagement and variable clinic sizes based on statistical measures, graphical approaches, and team discussions. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline was followed. 25 This work was designated non-research since it was carried out as a quality improvement evaluation under the terms of a signed attestation of non-research from the University of Iowa Institutional Review Board [IRB #202002500]. The authors had full access to and take full responsibility for the integrity of the data.
Data Sources
VHA administrative data and electronic health records were accessed using the Corporate Data Warehouse (CDW) to obtain clinic- and patient-level data. Clinic-level data, including facility type, was obtained from the VHA Site Tracking System. Clinic size was obtained from the Primary Care Management Module, a quarterly census of active primary care patients. The number of primary care full-time equivalents (FTEs) in VHA clinics or by CRH providers and the 4 outcomes (ie, established and new patient wait time, time to third next available26,27 appointment, proportion of new patients seen within 20 days) were obtained from the VHA Support Services Center and aggregated to the clinic-month. Lastly, the timely care success rate was calculated using outpatient and appointment tables from CDW. 28
Patient-level data, including demographics (ie, age, sex, race, rural residency, and VHA Nosos risk adjustment score, which uses a scoring algorithm based on patient diagnoses, age, sex, pharmacy records, VA priority status, and VA-computed costs 29 ), and the date, location, and delivery method of outpatient primary care visits were obtained from the CDW. The Area Deprivation Index, a measure of neighborhood socioeconomic disadvantage, 30 was spatially merged to the fiscal year-specific latitude and longitude of each veteran’s home address using 2020 Census Bureau census block TIGER/Line shapefiles.
Outcomes
Five measures of access to care were used: (1) established patient wait time; (2) new patient wait time; (3) third next available appointment,26,27 (4) timely care, 28 and (5) a binary indicator ≥80% of new patients were seen in 0 to 20 days. Established patients are those with a VHA primary care appointment in the past 3 years. Established patient wait time was measured from the date the patient and provider agree is clinically indicated for care to appointment completion date. New patient wait time was measured from the date the appointment was created to appointment completion date. Third next available and timely care are measures of clinic capacity. Third next available was the average time to the third open appointment in a provider’s clinic schedule.26,27 Timely care was defined as the provision of an appointment within 48 h of any patient requesting the clinic’s next available appointment or walking in to receive care. 28 These measures were averaged at the clinic level by month.
Covariates
Patient access is affected by a clinic’s patient mix and its physical environment. In addition to our exposure of interest, a time-varying measure of minimal threshold CRH use (ie, ≥10 CRH visits/month) was constructed; it was measured monthly and matched in time to each outcome. Clinic variables included facility type and size, categorized gap metric, 31 and VISN (VHA designation of region). Clinic size, as determined by the number of primary care patients assigned per year in the primary care management module, was categorized as small (450-2399), medium (2400-9999), and large (10 000+). The categorized gap metric, the ratio of the CRH-corrected expected number of primary care patients to the observed number of primary care patients, was calculated monthly and categorized as understaffed (<1.0), marginally staffed (1.0-1.2), and adequately staffed (≥1.2).
Patient variables were aggregated to the clinic-month and included average patient age, proportion male, proportion white, proportion rural, 32 and average Nosos score 29 anchored to October 1, 2022 (ie, the midpoint of the study period), and average Area Deprivation Index. 30
Statistical Analyses
We describe the clinic and patient mix characteristics, as well as study outcomes stratified by clinic-level CRH user status. Group comparisons were 2-sided with a .05 significance level using a t-test or chi-square test, as appropriate. We summarize the proportion of understaffed clinic-months in which the clinic met the minimum threshold for CRH use (ie, ≥10 CRH visits/month) by VISN.
The primary analysis used a within-between model framework, which partitions estimates into within-group and between-group effects. Each outcome was modeled separately using a generalized linear mixed model with a random intercept for clinics and adjusted using the covariates previously described. Model estimates, standard errors, and an indicator of significance are reported. The Hausman specification test assessed whether between and within effects were the same. Models were assessed for multicollinearity using the adjusted generalized standard error inflation factor (aGISF), which can accommodate categorical variables with more than 2 levels. 33
A sensitivity analysis considering only the most recent 2 years of data (eg, October 1, 2022, through September 30, 2024) was performed, as the program’s ability to provide primary care when a clinic was understaffed improved over time.
All analyses were conducted using R (version 4.4.0) via the panelr package.34,35 The study was approved by the University of Iowa Institutional Review Board [IRB # 202002500] and the Iowa City VA Healthcare System Research and Development Committee. We conducted this work without direct patient contact using routinely collected data deemed of minimal risk. A waiver of informed consent was obtained.
Results
From October 1, 2020, through September 30, 2024, 37.1% of primary care clinics (N = 366) were defined as a CRH user (ie, used ≥10 primary care CRH visits for 2 consecutive months; Table 1). CRH user clinics compared to controls were more likely to serve 10 000+ patients (28.4% vs 10.0%; P < .001), and slightly more likely to be understaffed (15.8% vs 14.8%; P < .001). CRH users had, on average, longer mean [SD] wait times compared to controls for both established (5.8 [4.0] vs 5.1 [5.1] days) and new patients (21.6 [14.2] vs 20.1 [13.5] days). CRH users also experienced longer mean [SD] times for the third next available visit (13.7 [7.2] vs 11.4 [6.8] days) compared to control clinics, with 67.6% vs 71.1% of requests for timely care being fulfilled.
Characteristics of Clinical Resource Hub (CRH) User and Control Clinics.
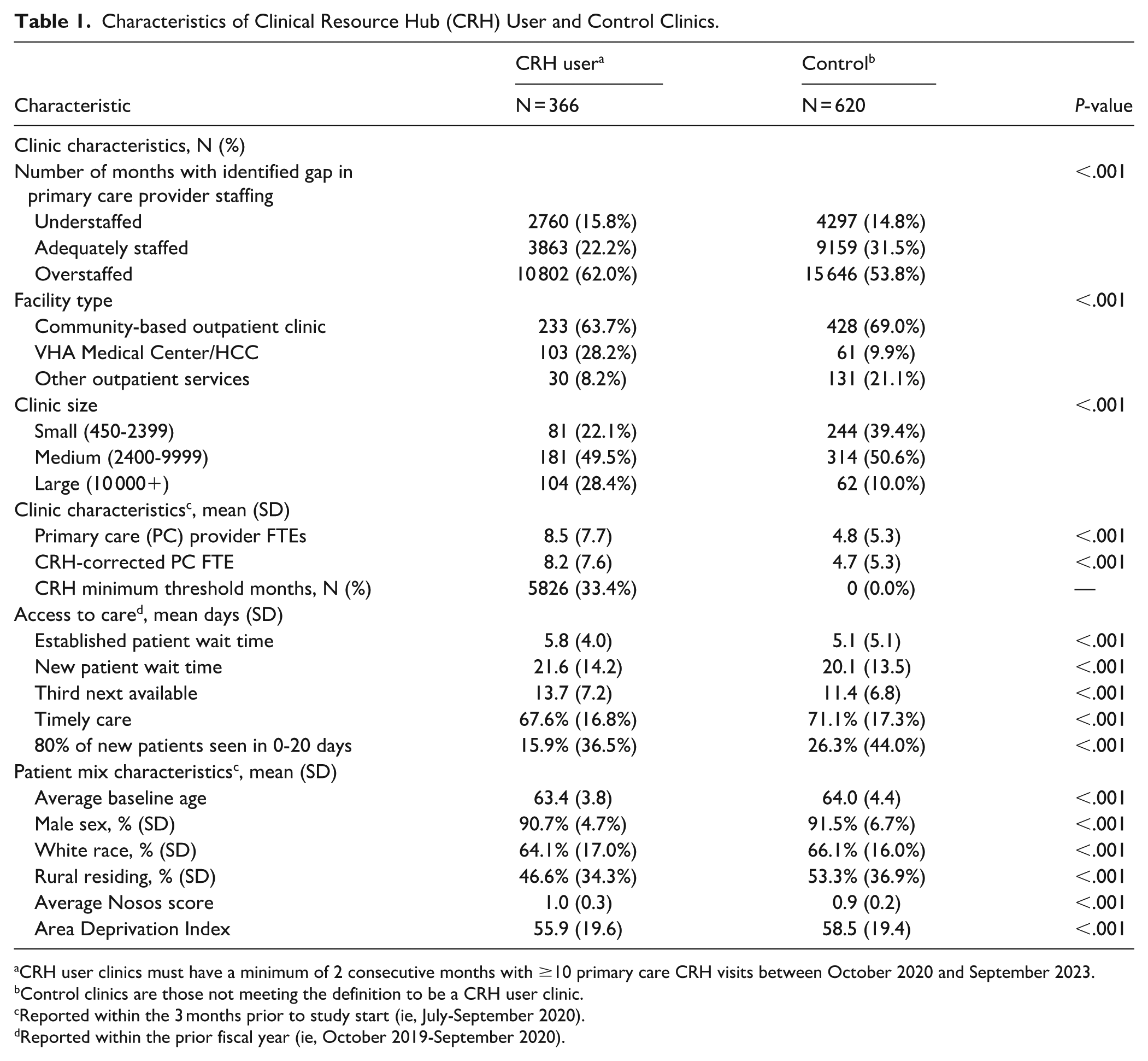
CRH user clinics must have a minimum of 2 consecutive months with ≥10 primary care CRH visits between October 2020 and September 2023.
Control clinics are those not meeting the definition to be a CRH user clinic.
Reported within the 3 months prior to study start (ie, July-September 2020).
Reported within the prior fiscal year (ie, October 2019-September 2020).
Within clinic, on average, the models estimated an increase of 0.36-day (SE = 0.07; P < .001) and 0.76 day (SE = 0.20; P < .001), respectively, for established and new patient wait times when a clinic delivered ≥10 CRH primary care visits in a month versus not (Table 2).
Within-Between Models Estimates (Standard Errors) for Wait Time Outcomes.

Abbreviation: ADI, Area Deprivation Index.
The generalized linear mixed model was estimated using a normal distribution with identity link function and random intercept at the clinic-level; the between model also adjusted for VISN, but results for these fixed effects are not reported in the table.
P < .05. †P < .01. ‡P < .001.
No significant associations with meeting the minimum threshold for CRH use per month were noted for the third next available appointment or when a clinic saw at least 80% of new patients within 20 days. (Table 3). However, an average decrease in timely care of 1.41% (SE = 0.21; P < .001) is noted within clinics, when ≥10 CRH primary care visits are provided in a month versus not.
Association of Months When CRH Engaged With Access Within and Between Clinics in National Sample of VA Clinics From October 2020 Through September 2024.

Abbreviation: ADI, Area Deprivation Index.
The generalized linear mixed model was estimated using a normal distribution with identity link function and random intercept at the clinic-level; the between model also adjusted for VISN, but results for these fixed effects are not reported in the table.
P < .05. †P < .01. ‡P < .001.
Sensitivity Analysis
Overall, the CRH program’s ability to provide primary care gap coverage at clinics with identified staffing gaps improved over time (Supplemental eTable 1). Clinical characteristics of CRH users and control clinics were similar in the 2-year period (eg, October 1, 2022, thru September 30, 2024) as in the full study (Supplemental eTable 2). Estimates of the within clinic effects of the time-varying minimum threshold for CRH use were similar, though slightly greater in magnitude for established patient time (β = .46 day, SE = 0.11, P < .001; Supplemental eTable 3) and timely care (β = −1.55 day, SE = 0.34, P < .001; Supplemental eTable 4), while no significant association was identified for new patient time.
Conclusions
VHA has a long history of providing care to America’s veterans.36-41 The expanded role of telehealth in clinical settings, influenced heavily by the COVID-19 pandemic, will likely persist. CRH fulfills the need for short- and long-term provider coverage by delivering remote providers to areas with provider shortages to ensure access to care remains available. 18 In this longitudinal evaluation of the CRH program, we found (1) measures of access were, on average, worse at CRH user clinics compared to control clinics, and (2) CRH users had marginally longer wait times. Ultimately, though the CRH program has provided remote staffing to avoid interruptions in care, these findings suggest additional efficiencies may be needed.
Provider shortages in rural and underserved areas are projected to grow.6,42,43 The Health Professional Shortage Area (HPSA) program has attempted to improve health outcomes for rural and underserved communities through loan repayment assistance, increased Medicare reimbursement, J-1 visa waivers, and more, 42 but with no significant impact on mortality or physician density. 44 Despite programs offering financial incentives for primary care providers to move to underserved areas, few physicians relocated after establishing their practice and for those that did, more moved from HPSA to non-HPSA areas. 45 Importantly, the CRH program is not the only innovative telehealth program to address geographic disparities in provider availability and patient need. Like the CRH, these programs are conducted with remotely located medical doctors who work alongside in-person support (eg, nursing staff and physician assistant).46-50 However, they are typically implemented for specific specialties (eg, hospitalist, pediatric gastroenterology, and mental health)46-50 rather than offering a tableau of services.18,51 This paper addresses an important way rural and underserved areas could facilitate increased access to care – through providers living in non-HPSA areas, but who provide telehealth when staffing gaps exist.
Despite this potential, established and new patient wait times increased, albeit by less than a day, when a clinic met the minimum threshold for monthly CRH use. This could be a consequence of a clinic’s existing staffing gaps and subsequent need to engage with the CRH. A lack of primary care providers may lead to longer wait times, which further creates a backlog of appointments that must be addressed before wait times can improve. This increase in wait times may also be related to previous attempts to increase primary care access through the provision of VHA-purchased community care, which reduces the need to maintain appointment availability for veterans receiving care outside VHA facilities. Notably, previous research has found wait time for VHA-purchased primary care in the community was longer compared to that provided by VHA facilities, often exceeding the modest half-day differences we detected when CRH is engaged.52,53
We note further that some control clinics also experienced understaffed months but did not sufficiently engage with the CRH to be considered a CRH user. Some of these clinics may have experienced short-term needs prohibitive to using the CRH program, which requires the time to coordinate CRH providers with VHA staff at spoke locations. Additionally, the choice not to engage with the program could be due to difficulties staffing non-provider (eg, nurse, pharmacist, and medical assistant) clinic roles. 54 Finally, decreased use may be due to lack of awareness or resources (eg, training, infrastructure, staffing, etc.) needed to implement the program.
The study’s strengths include its large national study population, but it does have some limitations. While our study population was diverse regarding rurality, race, and socioeconomic status, the majority were older men reducing generalizability. Additionally, because clinics choose to engage with the CRH program based on their need for support, selection bias may have impacted our results. Though the longitudinal nature of the data is a strength, this retrospective observational study can only illustrate associations, not causation, and it is constrained by the accuracy of the retrospective data reported in the electronic medical record. Additionally, the results were not broken down based on the geographic location of the clinic though previous studies have shown geography can play a significant role in access to care. 55 Lastly, patient outcomes were not tracked to determine if the care delivered remotely was adequate for patient need.
In conclusion, we assessed access in primary care clinics stratified by meaningful CRH engagement. CRH user clinics were more likely to have reduced access and marginally longer wait times. Findings suggest CRH has provided care in the presence of staffing shortages. However, further research into implementation barriers in smaller and more rural clinics should be considered.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261424758 – Supplemental material for A Longitudinal Evaluation of a Novel Short-Term Staffing and Telehealth Program: A Retrospective Observational Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319261424758 for A Longitudinal Evaluation of a Novel Short-Term Staffing and Telehealth Program: A Retrospective Observational Study by Paige Carlson, Bjarni Haraldsson, Matthew R. Augustine, Peter J. Kaboli and Amy M. J. O’Shea in Journal of Primary Care & Community Health
Footnotes
Author Note
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the United States Government.
Ethical Considerations
The study was approved by the University of Iowa Institutional Review Board [IRB # 202002500] and the Iowa City VA Healthcare System Research and Development Committee.
Consent to Participate
We conducted this work without direct patient contact using routinely collected data deemed of minimal risk. A waiver of informed consent was obtained.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported (or supported in part) by the VHA Primary Care Analytics Team (PCAT), funded by the VHA Office of Primary Care, as well as the Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, Veterans Rural Health Resource Center – Iowa City, and the Office of Research and Development, Health Services Research and Development (HSR&D) Service through the Comprehensive Access and Delivery Research and Evaluation (CADRE) Center (CIN 13-412). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. This manuscript is not under review elsewhere and there is no prior publication of manuscript contents. The preliminary results of this manuscript were presented at the Society of General Internal Medicine Meeting; Boston, Massachusetts in May 2024 and the Annual Meeting of Academy Health; Baltimore Maryland in June 2024.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to US Department of Veterans Affairs (VA) regulations and our ethics agreements, the analytic data sets used for this study are not permitted to leave the VA firewall without a Data Use Agreement. This limitation is consistent with other studies based on VA data. However, VA data are made freely available to researchers with an approved VA study protocol. For more information, please visit ![]() or contact the VA Information Resource Center at
or contact the VA Information Resource Center at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.