
Abstract
Background:
Hypertension remains a leading cause of cardiovascular disease in Latin America and the Caribbean (LAC), where control rates are persistently low. Community-based strategies are promising approaches to overcome barriers to care.
Objective:
To evaluate the effectiveness of community-based interventions for hypertension prevention and control among adults in LAC.
Methods:
A systematic review was conducted according to the PRISMA 2020 guidelines. PubMed, LILACS, Scopus, and SciELO were searched for randomized controlled trials (RCTs) published between January 2010 and October 2025.
Results:
Eighteen RCTs (n = 12 134 participants) were included. Interventions comprised community health worker (CHW) programs, lifestyle counseling, mobile health messaging, and salt substitution. Multicomponent CHW-led interventions demonstrated the greatest impact, with systolic blood pressure (SBP) reductions of 5 to 13 mmHg and significantly improved control rates. Digital messaging interventions consistently enhanced medication adherence. Educational and lifestyle programs showed variable but often positive effects on SBP.
Conclusions:
Community-based interventions, particularly integrated CHW-led models supported by digital tools, are effective for improving hypertension control in LAC. Scaling these evidence-based strategies within primary healthcare systems can help reduce the regional cardiovascular disease burden.
Keywords
Introduction
Hypertension (HTN), defined as a persistent elevation in arterial pressure, is a leading global chronic condition and a primary contributor to cardiovascular and renal morbidity, including stroke, myocardial infarction, heart failure, and kidney disease.1,2 While diagnostic thresholds continue to evolve, current guidelines recognize sustained blood pressure readings of ≥130/80 mmHg as hypertensive, with a treatment goal often set below this threshold. For this review, and to maintain consistency with the outcome measures used across the included studies conducted in Latin America and the Caribbean (LAC), we apply the widely used operational definition of hypertension as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg. This pragmatic threshold aligns with regional clinical practices and allows for direct interpretation of the intervention outcomes reported in the literature. Hypertension remains a leading global risk factor for cardiovascular disease, stroke, and kidney failure, contributing to nearly 10 million deaths annually and earning its reputation as a “silent killer” due to its frequently asymptomatic progression.3,4 In Latin America and the Caribbean (LAC)—a region encompassing Mexico, Central America, South America, and the Caribbean island nations - this condition represents a growing public health crisis, affecting 20% to 40% of the adult population and standing as the primary risk factor for cardiovascular morbidity and mortality. 5
Despite the availability of effective treatments, only about one-third of patients in the region achieve adequate blood pressure control, a gap exacerbated by low awareness, clinical inertia, limited health literacy, reliance on traditional remedies, and strained health systems.6-9 In this context, community-based interventions have emerged globally as a promising and sustainable approach to bridge the divide between clinical care and patient needs, with evidence showing that programs integrating education, follow-up, and self-management support can significantly improve adherence, reduce blood pressure, and promote healthier lifestyles. 10
Such strategies, often spearheaded by well-trained Community Health Workers (CHWs), emphasize local empowerment, cultural relevance, and trust, effectively connecting communities with formal health systems and offering an equitable pathway to address cardiovascular disparities.11,12 However, despite compelling international examples—such as the community-driven hypertension treatment group in rural Honduras shown to be feasible and effective 13 —rigorous, region-specific evidence on scalable models remains fragmented and limited across LAC. Most existing studies are small-scale or country-specific, lacking the generalizability needed to inform broad policy and practice.
This systematic review, therefore, seeks to consolidate and evaluate the highest-quality evidence from randomized controlled trials (RCTs) to answer a central question: Among adults in Latin America and the Caribbean with hypertension, how effective are community-based interventions compared with usual care in achieving blood pressure control and related outcomes? By synthesizing RCT findings from across the region, this review aims to identify effective, scalable, and context-appropriate strategies to can strengthen primary care and reduce the cardiovascular burden in LAC.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The methodology was designed a priori to ensure transparency, reproducibility, and minimization of bias.
Protocol and Registration
The review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) to enhance transparency, reduce reporting bias, and prevent duplication of effort (Registration ID: CRD420251235689). Any deviations from the registered protocol are noted in the relevant sections below.
Eligibility Criteria
Studies were selected based on the following PICOS (Population, Intervention, Comparator, Outcomes, Study Design) framework:
Information Sources and Search Strategy
A comprehensive and systematic literature search was performed across 4 electronic databases from their inception to October 2025: PubMed/MEDLINE, LILACS (Latin American and Caribbean Health Sciences Literature), Scopus, SciELO (Scientific Electronic Library Online). The search strategy was developed iteratively by the research team with input from a health sciences librarian. It combined controlled vocabulary (eg, MeSH terms in PubMed) and free-text keywords related to 3 core concepts: (1) Hypertension, (2) Community-Based Interventions, and (3) Latin America and the Caribbean. Boolean operators (AND, OR) and proximity operators were used appropriately for each database. The search was limited to human studies and the publication date range (2010-2025). No language filters were applied during the search, but only studies in English, Spanish, or Portuguese were ultimately included. The reference lists of all included studies and relevant review articles were manually screened (backward snowballing) to identify additional eligible records. The complete search strategy for each database is documented in Table 1.
Detailed Search Strategy by Database (2010-2025).

Study Selection Process
All records identified through database searching were imported into Rayyan QCRI, a web-based systematic review management tool. After automated and manual deduplication, a 2-phase screening process was conducted independently by 2 reviewers (initials SB and LD). In the first phase, reviewers screened titles and abstracts against the eligibility criteria. In the second phase, the full texts of potentially eligible studies were retrieved and thoroughly assessed. At both stages, any disagreements between reviewers were resolved through discussion and consensus; if necessary, a third reviewer (RC) was consulted. The study selection process, including the number of records identified, excluded, and included, is presented in a PRISMA 2020 flow diagram (Figure 1).
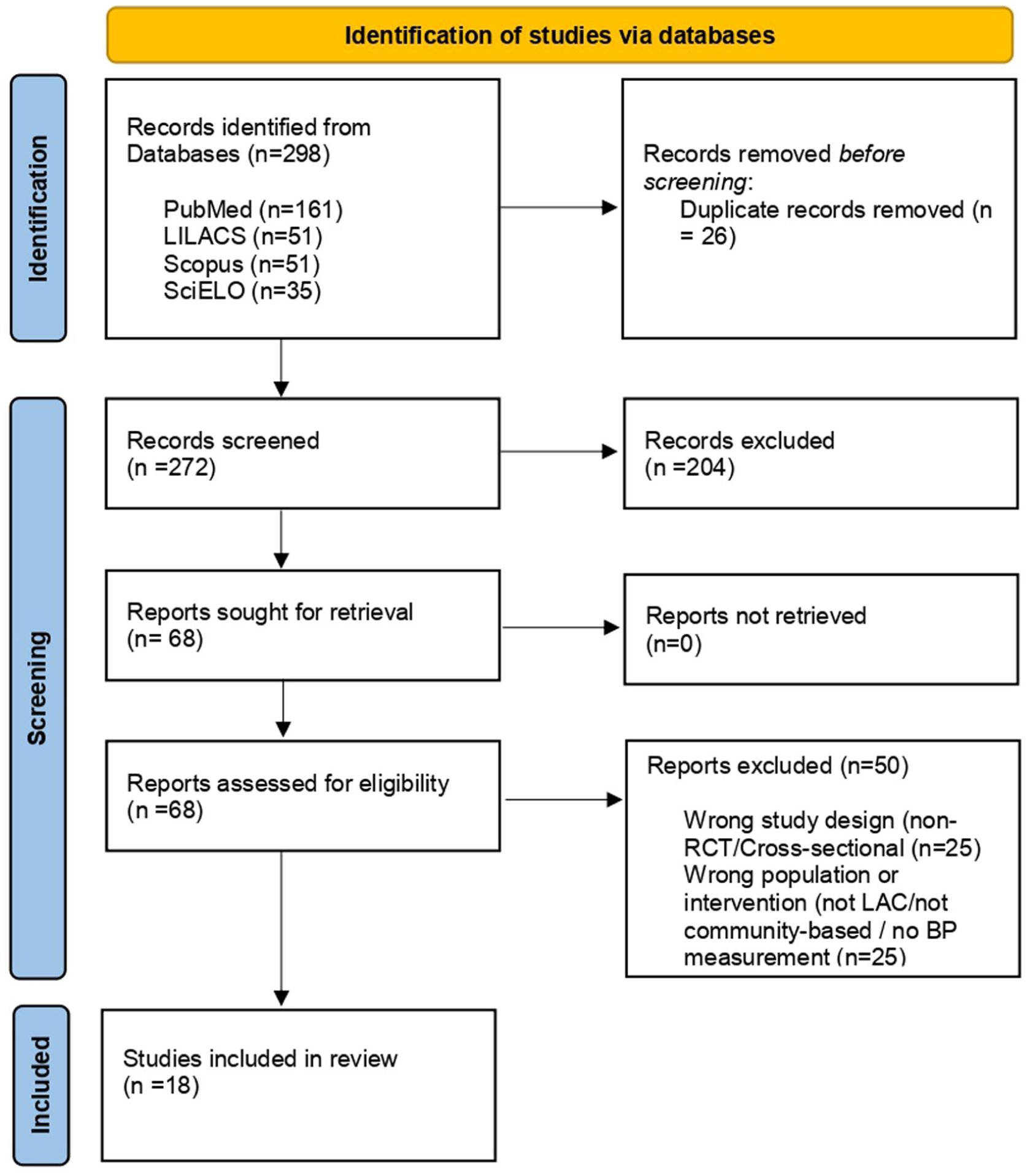
PRISMA 2020 flow diagram of the study selection process.
Data Extraction
Data from each included study were extracted independently by 2 reviewers (SB and RC) using a standardized, piloted data extraction form in Microsoft Excel. The form captured the following information:
Quality Assessment (Risk of Bias)
The risk of bias in each included RCT was assessed independently by 2 reviewers (LD and SB) using the revised Cochrane Risk of Bias tool for randomized trials (RoB 2), taking into account each trial’s design (individual or cluster). The tool evaluates 5 domains: Bias arising from the randomization process. Bias due to deviations from intended interventions. Bias due to missing outcome data. Bias in the measurement of the outcome. Bias in the selection of the reported result.
Judgments for each domain were made as “Low risk,” “Some concerns,” or “High risk.” An overall risk-of-bias judgment was then derived for each study. Disagreements were resolved through discussion. The results of the risk-of-bias assessment are presented narratively and graphically using the robvis visualization tool.
Data Synthesis
Given the substantial clinical and methodological heterogeneity observed among the included studies—including diverse intervention types (CHW-led, digital, educational), varying comparator groups, different follow-up durations, and differences in outcome measurement—a quantitative meta-analysis was deemed inappropriate. Therefore, findings are synthesized narratively. Studies are grouped and described by primary intervention category (eg, CHW-led multicomponent programs, digital/mHealth interventions, educational/lifestyle counseling). For each category, we summarize the intervention characteristics, consistency of effects on primary outcomes (SBP/DBP reduction, BP control), and effects on secondary outcomes (adherence, knowledge). Results are presented in summary tables (eg, Table 2 for study characteristics, Table 3 for main outcomes) to facilitate comparison. All analyses and syntheses were conducted using standard software (Microsoft Excel, Word).
Characteristics of Included Randomized Controlled Trials.

Abbreviations: CHW, community health worker; DM, diabetes mellitus; HBPM, home blood pressure monitoring; HTN, hypertension; SBP/DBP, systolic/diastolic blood pressure.
Main Outcomes of Included Randomized Controlled Trials.

Results
Study Selection
The database search yielded 298 records for screening. After removing 26 duplicates, 272 unique titles and abstracts were assessed for eligibility. Of these, 204 records were excluded based on title and abstract screening because they clearly did not meet the eligibility criteria (eg, wrong study design, population, or intervention). The remaining 68 full-text articles were retrieved and evaluated in detail. Ultimately, 18 randomized controlled trials published between 2009 and 2025 met all inclusion criteria and were included in this systematic review. The study selection process is illustrated in the PRISMA 2020 flow diagram (Figure 1). The most common reasons for exclusion at the full-text stage were non-randomized study design, the absence of a community-based component, or the study being conducted outside the LAC region.
General Characteristics of Included Studies
The 18 RCTs included a cumulative sample of 12 134 participants from 8 LAC countries: Argentina, Brazil, Chile, Colombia, Haiti, Mexico, and Peru, plus one study on the U.S.-Mexico border. 15 Settings ranged from urban primary care clinics and community centers to rural villages and vulnerable favelas. Sample sizes varied widely, from 28 participants in a small behavioral 19 to 2376 in a population-level salt substitution study. 30 Follow-up durations spanned from 45 days to 24 months, with most trials reporting outcomes at 6 or 12 months. The key characteristics of all included trials are summarized in Table 2.
Intervention Categories and Critical Analysis of Effects
The interventions were categorized into 4 main types, revealing distinct patterns in their implementation and impact. Interventions were categorized through an inductive, iterative process by 2 reviewers (SB and LD) based on the primary mode of delivery, the principal delivery agent, and the core intervention components. Discrepancies were resolved through discussion and consensus with a third reviewer (RC). This analytic process yielded 4 distinct categories.
CHW-Led Multicomponent Programs (6 trials)
This category, which included the largest trials (He et al. 16 and Schwalm, et al. 27 in Argentina, St Sauveur et al. 28 in Haiti), demonstrated the most substantial and consistent effects. Interventions involved CHWs in home visits, patient education, BP monitoring, and, in some cases, protocol-guided treatment titration. A key characteristic of the most effective programs in this category was the formal integration of CHW support with the healthcare system, evidenced by the use of structured treatment protocols, scheduled physician consultations, and systems for providing free or subsidized medications.16,27 The Haiti study, which added physician supervision to CHW follow-up, achieved a remarkable 12.8 mmHg SBP reduction. 28 The programs that formally integrated CHW support with physician collaboration and systematic treatment protocols demonstrated the largest improvements in blood pressure outcomes.
Digital and mHealth Interventions (4 trials)
Trials using SMS (Varleta et al., 2017; Cangucu et al.18,33) or WhatsApp (Sartori et al., 2020; Sudré et al.23,26) primarily targeted medication adherence and self-management education. While SBP reductions were more modest (3.9-9 mmHg), these interventions showed a strong, consistent positive effect on adherence. For example, the WhatsApp trial increased adherence from 55% to 75%, and the Chilean SMS trial reported a 1.3 fold increase in adherence.18,23 Digital messaging interventions consistently improved medication adherence, whereas their associated reductions in systolic blood pressure were more modest than those achieved by multicomponent programs.
Educational and Lifestyle Counseling Programs (5 trials)
These interventions, delivered by nurses, nutritionists, or other health professionals19,20,22 showed variable but often significant reductions in SBP (4-13 mmHg). The intensity and modality were key determinants of effect size. The most impactful was an intensive Brazilian program for hypertensive women that combined group workshops with personalized home visits, achieving a 13 mmHg SBP drop. 19 In contrast, less intensive counseling showed smaller effects. The effect size of educational and lifestyle programs correlated with intervention intensity and modality, with the greatest systolic blood pressure reductions observed in programs that incorporated personalized, direct support such as home visits.
Other Targeted Interventions (2 trials)
These studies evaluated specific, novel strategies. The population-level salt substitution trial in Peru 30 demonstrated that a structural, environmental intervention could yield a significant public health impact, with a 1.29 mmHg mean SBP reduction at the community level and a 51% reduction in hypertension incidence. The pharmacist-led collaborative management trial in Brazil 31 successfully focused on medication safety in older adults, increasing appropriate deprescribing. Trials evaluating structural and pharmacotherapy-focused strategies, such as salt substitution and collaborative drug therapy management, demonstrated significant public health and clinical impacts, including reduced hypertension incidence and improved medication safety.
Risk of Bias Assessment
The methodological quality of the 18 included RCTs was assessed using the Cochrane RoB 2 tool. 34 See Figure 2 for a domain-level summary of risk of bias judgments across all included studies.
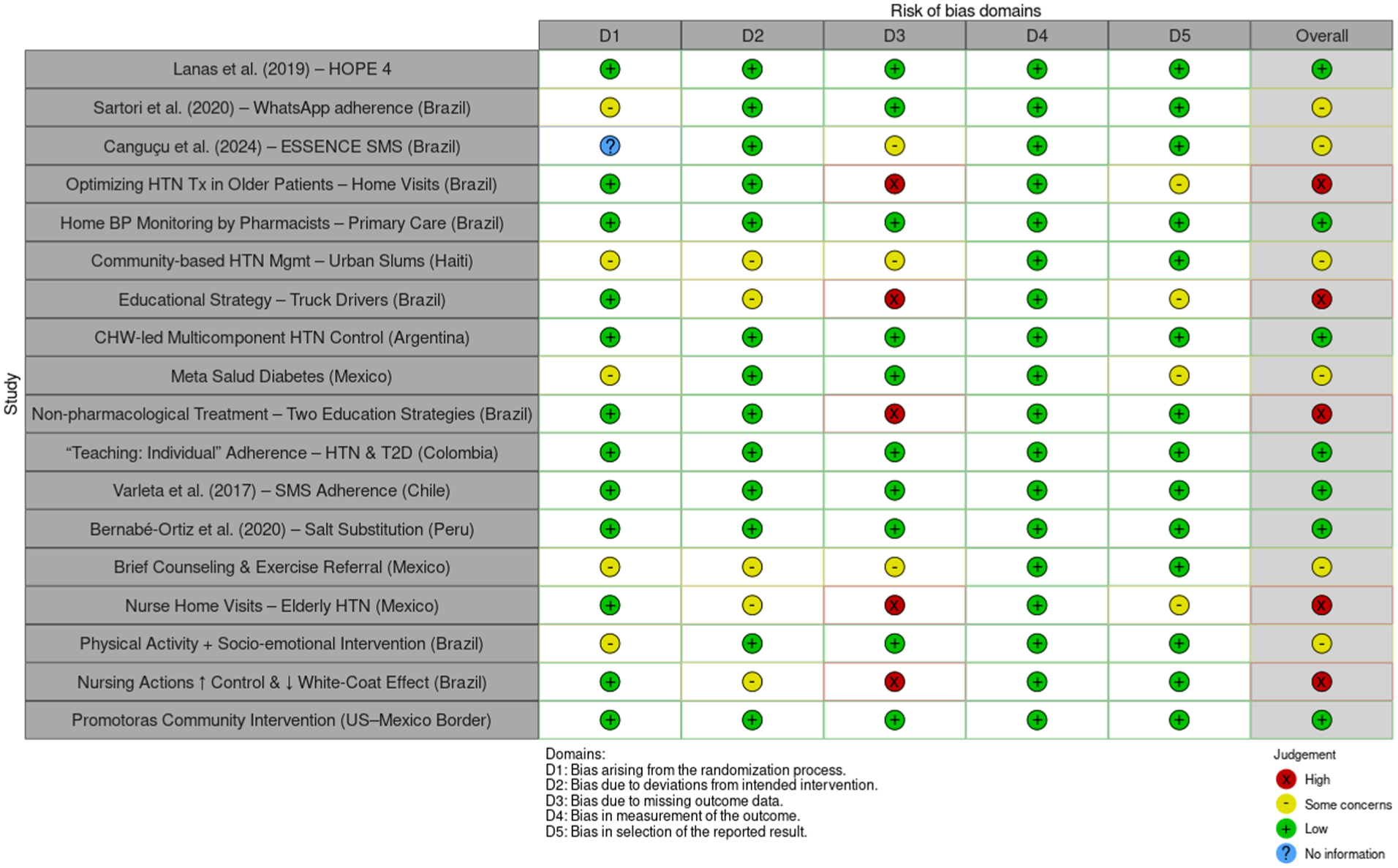
Risk of bias assessment summary.
Most large, cluster-randomized trials were judged to have a low risk of bias across domains.16,25,27 Common issues raising “some concerns” or “high risk” in smaller trials arose in 2 domains: (1) Bias due to missing outcome data (D3), often from high or differential loss to follow-up in community-based lifestyle studies; and (2) Bias in measurement of the outcome (D4), primarily in studies relying on self-reported adherence or unblinded BP measurement. For example, several digital and education-based trials (eg, the WhatsApp trial by Sartori et al. 23 and the educational video trial by Sudré et al. 26 ) had concerns in D4 due to the use of self-reported outcomes. A few studies with home-visit designs had a higher risk due to incomplete follow-up data. This pattern indicates that while the overall evidence is robust, findings from smaller, unblinded trials with high attrition should be interpreted with greater caution.
Synthesis of Main Outcomes
A narrative synthesis of the primary outcomes from all 18 trials is presented in Table 3. The data consistently show that community-based interventions positively impact hypertension management in LAC.
The collective evidence demonstrates a gradient of effect based on intervention complexity. Multicomponent CHW-led models achieved the greatest clinical impact (SBP reductions >10 mmHg, large increases in control rates). Digital and focused educational interventions showed significant but smaller effects on BP (3-9 mmHg reductions), with a strong, consistent benefit for improving medication adherence. Notably, even the structurally-oriented salt substitution trial, while showing a small mean population SBP shift, demonstrated a powerful effect in reducing new cases of hypertension. This synthesis confirms that community-based strategies are effective across the prevention-control continuum, but their design must align with the intended outcome: complex, integrated care models to achieve clinical control in hypertensive populations, and scalable digital or public health tools to improve adherence or primary prevention.
Discussion
This systematic review synthesizes findings from 18 randomized controlled trials evaluating community-based interventions for hypertension control in Latin America and the Caribbean. The collective evidence robustly demonstrates that such interventions are effective, yet a critical analysis reveals a clear gradient in their impact, largely dictated by design complexity, integration with the formal health system, and the specificity of their target outcomes. The most substantial improvements in systolic blood pressure (SBP) and control rates were achieved not by any single activity, but by multicomponent, CHW-led models that formally bridged the community and clinic. Programs like HOPE 4, and those in Argentina and Haiti, which combined CHW home visits, structured treatment protocols (sometimes including medication titration), physician collaboration, and free access to medicine, consistently produced SBP reductions exceeding 10 mmHg and near-doubling of control rates.16,27,28 This success underscores a critical principle: CHWs function most powerfully as extensions of a supported healthcare team rather than as isolated advocates. Their effectiveness is magnified when they are equipped with clear guidelines, clinical backup, and the resources to address structural barriers such as medication costs, thereby mitigating the “clinical inertia”—the failure of healthcare providers to intensify therapy when treatment goals are not met in the region. 7 In contrast, digital and focused educational interventions demonstrated more modest, though still valuable, effects. Trials using SMS or WhatsApp primarily improved medication adherence—a crucial intermediate outcome—with associated SBP reductions typically in the 4-9 mmHg range.18,23,33 This pattern suggests that these tools are exceptionally effective for patient engagement, reminder functions, and knowledge dissemination, acting as a scalable “digital glue” for chronic disease management. However, their standalone capacity to achieve full clinical control may be limited without embedded mechanisms for treatment intensification. Similarly, lifestyle education programs yielded variable results; their success was directly proportional to their intensity and personalization, as seen in the 13 mmHg SBP reduction achieved with a program combining group workshops and home visits. 19 This highlights that knowledge translation requires sustained, tailored support to overcome entrenched behavioral and environmental barriers.
The findings align with and strengthen the global evidence base for community-based strategies. The magnitude of effect in the most successful LAC-based CHW programs is comparable to that of landmark trials in South Asia, such as the COBRA-BPS study, which also reported SBP reductions around 11 mmHg through a similar model of trained health worker-led care. 35 Furthermore, the effectiveness of digital adherence support mirrors meta-analytic findings from underserved populations in the United States. 36 This convergence across diverse contexts reinforces the generalizability of 2 core tenets: first, that task-sharing to trained lay workers is a viable strategy for hypertension control in resource-constrained settings, and second, that digital tools can effectively support self-management globally. The success of the Peruvian salt substitution trial further broadens the paradigm, demonstrating that environmental, population-level modifications can complement individual-level interventions for primary prevention, significantly reducing hypertension incidence at a community scale. 30
Theoretically, the superiority of multicomponent interventions can be explained by their ability to simultaneously target multiple points in the care cascade. They address lack of awareness through education, poor adherence through consistent follow-up and reminders, and clinical inertia through protocolized management and facilitated linkage to care. This layered approach resonates with models of chronic care that emphasize prepared, proactive teams and informed, activated patients. Digital tools fit into this model not as replacements, but as force multipliers that enhance the efficiency and reach of human-delivered care, a synergy hinted at in trials like ESSENCE. 22
For the LAC region specifically, these results provide a timely and actionable evidence base. They move beyond demonstrating feasibility to outlining a hierarchy of effectiveness. Policymakers and health system planners can interpret this gradient to match interventions to local needs and capacities: well-integrated CHW programs for high-burden areas with poor control rates, digital adherence support to strengthen existing primary care, and public health regulations (such as salt substitution) to reduce population-wide risk. The consistent positive signal across all categories confirms that community-based strategies are a critical and effective component of a comprehensive response to the region’s hypertension crisis, offering a pathway to strengthen primary healthcare and advance equitable cardiovascular health outcomes. 37
Limitations
While this review provides a robust synthesis of RCT evidence, several limitations must be acknowledged. First, the review process itself had constraints. The search was limited to 4 databases, excluding others such as Embase and Scopus, which may have led to the omission of relevant studies. While inclusive of major regional databases (LILACS, SciELO), the restriction to English, Spanish, and Portuguese publications likely excluded research in French or Creole from parts of the Caribbean. Furthermore, gray literature and unpublished trials were not systematically searched, potentially introducing publication bias.
Second, while we prioritized searches in regional databases (LILACS, SciELO) most relevant to the LAC context, we did not search major global databases such as Embase and Scopus, which may have limited the comprehensiveness of the review. Third, methodological limitations exist within the body of included studies. There was significant clinical and methodological heterogeneity in intervention designs, comparators, and outcome measurements, precluding a meta-analysis and necessitating a narrative synthesis. The quality assessment revealed that several studies, particularly smaller-scale trials, had “some concerns” or “high risk” of bias, most notably due to missing outcome data and bias in outcome measurement from self-reporting or lack of blinding. Many trials had follow-up periods of 12 months or less, limiting conclusions about the long-term sustainability of intervention effects. The generalizability of findings from specific sub-populations (eg, pregnant women, truck drivers) to the broader hypertensive population is also uncertain.
Fourth, the synthesis has limitations in its scope. The review focused on efficacy as measured by RCTs, which provides limited insight into real-world implementation challenges, cost-effectiveness, or the contextual facilitators and barriers to scaling these interventions across diverse LAC health systems. The equitable reach of these interventions across different socioeconomic, ethnic, and rural groups also requires deeper exploration. Finally, as with any systematic review, there is a risk of publication bias, where studies with null or negative results are less likely to be published. This may lead to an overestimation of the true effectiveness of the interventions reviewed.
Recommendations
Based on the findings of this review, the following recommendations are proposed for policy, practice, and future research.
For Policy and Practice
Scale Integrated CHW Models
National and regional health ministries should prioritize integrating of trained, supported, and remunerated CHWs into primary care teams for hypertension management. Protocols should empower CHWs with clear guidelines for patient education, follow-up, and—where appropriate and with supervision—treatment monitoring and titration, ensuring formal linkages to prescribing clinicians.
Adopt and Adapt Digital Tools
Healthcare systems should leverage low-cost, high-reach digital tools (e. g., SMS, WhatsApp) as standard adjuncts to care to send medication reminders, reinforce education, and facilitate patient-provider communication. These should be integrated into existing patient management systems.
Invest in Structural & Public Health Interventions
Policymakers should evaluate population-level strategies, such as salt-substitution programs, given their significant preventive potential. Supportive regulations and fiscal policies to promote healthier food environments are crucial complementary actions.
Build Sustainable Support Systems for Community Health
To sustain the effective CHW-led models identified in this review, investment is needed in formal training, supportive supervision, and sustainable financing mechanisms within public health budgets to integrate these roles into primary healthcare systems.
For Future Research
Conduct Implementation & Scale-Up Research
Future studies should employ hybrid effectiveness-implementation designs to identify the key barriers and facilitators to scaling successful models like HOPE 4 in different LAC contexts. Research on cost-effectiveness and budget impact is urgently needed to inform investment decisions.
Focus on Long-term Outcomes and Equity
Studies with longer follow-up periods (>2 years) are required to assess the durability of BP control and cardiovascular outcomes. Research must explicitly analyze intervention effectiveness and access across social determinants such as gender, ethnicity, income, and geography to ensure equitable benefits.
Strengthen Methodological Rigor
Future RCTs should prioritize allocation concealment, blinded outcome assessment (where feasible), and strategies to minimize attrition to strengthen the validity of findings.
Explore Synergistic Strategies
Research should investigate the optimal combination and sequencing of multi-level strategies, such as CHW programs augmented by digital tools and supportive food policies, to create a comprehensive ecosystem for hypertension prevention and control.
Conclusion
This systematic review demonstrates that community-based interventions are a viable and effective strategy for improving hypertension control in Latin America and the Caribbean. Evidence from 18 randomized controlled trials reveals a spectrum of impact: multicomponent programs led by community health workers working within supported healthcare systems yield the most significant clinical improvements, while digital and focused educational interventions effectively enhance medication adherence and self-management. The collective findings underscore that moving hypertension care beyond clinic walls into communities is not only feasible but essential for addressing persistent gaps in awareness, treatment, and control. The evidence indicates a gradient of effectiveness, with the greatest clinical impact arising from multicomponent programs that integrate community health workers into the formal healthcare system. To translate this evidence into widespread public health gain, a concerted effort is required to strategically integrate these proven, low-cost approaches into strengthened primary healthcare systems across the region, fostering a more equitable and sustainable path toward cardiovascular health.
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data generated and associated with this research have been provided in this article.