
Abstract
Anxiety and depression are common yet often underdiagnosed, particularly in underserved populations. In Ecuador, limited access to mental health care heightens this concern. This study assessed the utility of the Patient Health Questionnaire-4 (PHQ-4), a brief screening tool for anxiety and depression, among individuals aged 12 and older during a medical brigade in Santo Domingo, Ecuador in August 2020. A total of 380 participants completed the PHQ-4. Results were analyzed by age, sex, and symptom severity. Pediatric females reported significantly higher anxiety rates than males (35.8% vs 12.5%, P < .05), while depression was more common in females but not statistically significant. Anxiety increased with age, while depression showed no clear trend. Overall, anxiety and depression rates exceeded national estimates for Ecuador. The PHQ-4 effectively identified at-risk individuals, supporting its use in global health settings to screen mental health conditions and guide care in underserved populations.
Keywords
Background
Depression and anxiety are significant global health concerns, particularly in low- and middle-income countries (LMICs), including South America. 1 In Ecuador, the prevalence of depression is estimated at 4.6%, contributing to 9.2% of the country’s disability-adjusted life years (DALYs). 2 The prevalence of anxiety in Ecuador is 5.6%, accounting for 5.8% of years lived with disability (YLDs; WHO, 2017). Despite this high burden, the diagnosis and treatment of depression and anxiety in Ecuador remain limited. Studies suggest that just 4.7% of the population in LMICs receive appropriate care for depression (Pan American health organization, 2018). Similarly, anxiety disorders are common across all age groups, including adolescents, with significant underdiagnosis and undertreatment in many regions.3-7
Although the recent increases in the reported rates of depression suggest that there is an increasing awareness to this disease. However, the rates are still substantially lower than elsewhere. 8 Cultural factors may contribute to this discrepancy, as individuals in Latin American contexts often express psychological distress through somatic symptoms rather than explicitly reporting mood or anxiety-related concerns. 9 Limited mental health literacy, social stigma, and barriers to accessing care further exacerbate under recognition of mental health conditions within public health systems.
Given these challenges, brief and feasible screening tools may support early identification of individuals at risk for anxiety and depression in underserved settings. The Patient Health Questionnaire-4 (PHQ-4) has been developed to provide a brief and effective screening method for both depression and anxiety.10,11 This is a brief, validated screening tool designed to identify both depression and anxiety. It combines the 2-item PHQ-2 for depression and the 2-item Generalized Anxiety Disorder (GAD-2) scale for anxiety.11,15 The PHQ-4 has been validated in various populations, including Hispanic Americans, Colombians, and others,10-17 but has not been used in Ecuador.
This study aimed to describe the prevalence of anxiety and depressive symptoms, as identified through PHQ-4 screening, among pediatric and adult patients seen during a medical brigade in Santo Domingo, Ecuador. Secondary aims included identifying demographic patterns associated with screening-positive results and evaluating the feasibility and utility of implementing brief mental health screening in an underserved clinical context.
Method
Study Design and Ethical Considerations
This initiative was originally part of a broader medical brigade that integrated medicine, physical therapy, pharmacy, and nursing. A psychology team was included to triage patients for anxiety and depression, assess the feasibility of mental health screening in this setting, and provide on-site intervention as needed.
The Institutional Review Board (IRB) approved the retrospective analysis of de-identified data, allowing for post-hoc evaluation of screening outcomes.
Screening Procedure
The PHQ-4 was administered at the time of patient registration, and verbal consent was obtained with Spanish interpreter. No additional translation or cultural adaptation procedures were undertaken. Medical providers reviewed the PHQ-4 results with each patient. If a patient had moderate to severe symptoms, they were asked if they wanted to speak with a psychologist. Patients who accepted were further assessed and received interventions on-site, with referrals provided as needed.
Although patients appeared receptive to mental health screening, no formal data were collected on acceptance rates due to the non-research nature of the initial initiative.
The screenings were conducted during a medical brigade in August 2020, where psychologists administered the PHQ-4 to patients aged 12 and older seen in the clinic. Patient ages were classified into the following categories: 10 to 21 years (pediatric group), 22 to 40 years, 41 to 60 years, 61 to 80 years, and greater than 80 years of age.
The PHQ-4 includes 4 questions: 2 assessing anxiety symptoms and 2 assessing depression symptoms. Each question is rated on a scale from 0 to 3, with a score of 3 or higher indicating a positive result for anxiety or depression. Total scores range from 0 to 12, with 0 to 5 indicating mild symptoms, 6 to 8 indicating moderate symptoms, and 9 to 12 indicating severe symptoms. Psychologists were available to follow up with patients who screened positive.
Anxiety and depression outcomes were analyzed as dichotomous screening variables (yes/no). Categorical variables were examined using Pearson’s chi-square or Fisher’s exact tests, as appropriate. Multivariable logistic regression models were constructed for anxiety and depression outcomes, including age category, gender, and an age × gender interaction term. Backward elimination (α = .05) was used to derive final models. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) are reported. Analyses were conducted using IBM SPSS Statistics version 30.
Results
The PHQ-4 was used to assess both anxiety (via the Generalized Anxiety Disorder-2 scale) and depression (via the Patient Health Questionnaire-2). Each question is rated on a scale from 0 to 3, with a score of 3 or higher indicating a positive result for anxiety or depression. Total scores range from 0 to 12, with 0 to 5 indicating mild symptoms, 6 to 8 indicating moderate symptoms, and 9 to 12 indicating severe symptoms.
There was no significant association between gender and age (Table 1, P = .062), suggesting that the distribution of participants across age groups was similar between genders.
Association of Age with Gender, Anxiety and Depression Scores.

There was no significant association between gender and age (P = .062), suggesting that the distribution of participants across age groups was similar between genders. A significant association between age and anxiety status (P = .007), with higher anxiety symptoms among older participants. In contrast, no significant relationship was found between age and depression status (P = .195).
Chi-square analysis indicated a significant relationship between age and anxiety status (Table 1, P = .007), indicating that older patients were more likely to report anxiety. In contrast, no significant relationship was found between age and depression status (Table 1, P = .195). Multivariable logistic models showed that age category 22 to 40 was 1.44 (95% CI [0.77, 2.70]) times more likely to experience anxiety compared to the <22 age category. Age category 41 to 60 was 2.34 (95% CI [1.32, 4.13]) times more likely to experience anxiety compared to the <22 age category. Age category 61 to 80 was 3.38 (95% CI [1.78, 6.45]) times more likely to experience anxiety compared to the <22 age category. Age category >80 was 4.63 (95% CI [1.44, 14.85]) times more likely to experience anxiety compared to the <22 age category.
Significant gender differences were observed in both anxiety and depression. A significant relationship between gender and anxiety status was found (Table 2, P < .001), with females more likely to report anxiety than males. The interaction variable was removed from the model. Females were 3.48 (95% CI [1.99, 6.08]) times more likely to experience anxiety compared to males. Additionally, anxiety severity differed significantly by gender (Table 2, P < .001), with females reporting more severe anxiety symptoms.
Gender Differences in Anxiety Symptoms and Severity.
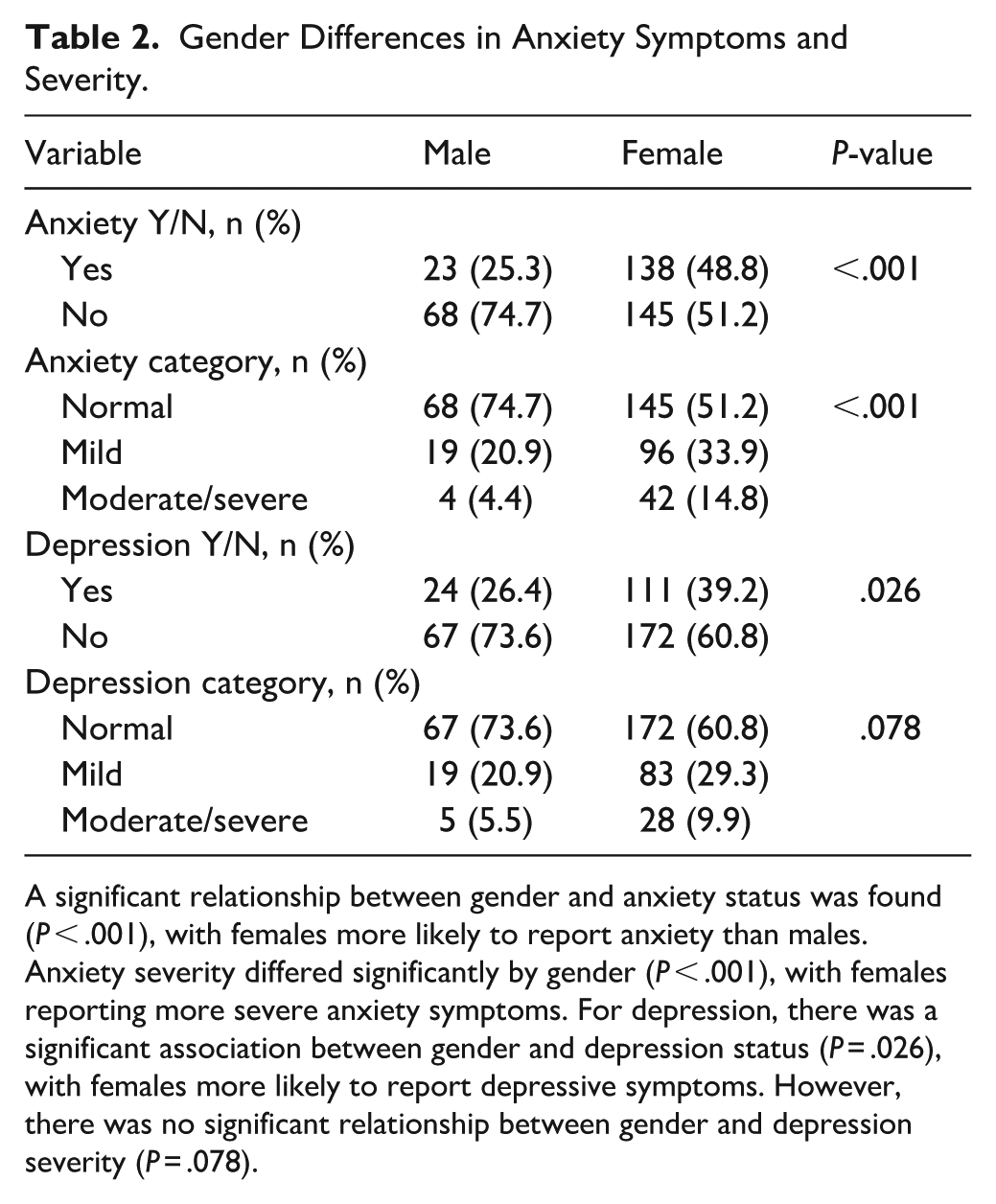
A significant relationship between gender and anxiety status was found (P < .001), with females more likely to report anxiety than males. Anxiety severity differed significantly by gender (P < .001), with females reporting more severe anxiety symptoms. For depression, there was a significant association between gender and depression status (P = .026), with females more likely to report depressive symptoms. However, there was no significant relationship between gender and depression severity (P = .078).
For depression, there was a significant association between gender and depression status (Table 2 P = .026), with females more likely to report depressive symptoms. The interaction variable and the age category variable were removed from the model. Females were 1.80 (95% CI [1.07, 3.04]) times more likely to experience depression compared to males in our study. However, there was no significant relationship between gender and depression severity (Table 2, P = .078).
Anxiety and depression were strongly associated with each other, with 64.2% of participants reporting symptoms of both depression and anxiety (Table 3, P = < .001).
Gender Differences in Depression Status and Severity.

Anxiety and depression were strongly associated with each other, with 64.2% of participants reporting symptoms of both depression and anxiety (P = < .001).
In the young and pediatric group, there was a significant relationship between gender and anxiety status (Table 4, P = .028), with females having more anxiety than males in this age group. However, no significant relationship was found between gender and depression status in this group (Table 4, P = .415).
Gender Differences in Anxiety and Depression Among Young and Pediatric Participants.

Note. Relationship between gender and anxiety status in the young and pediatric population, with females showing higher anxiety prevalence (P = .028). Relationship between gender and depression status in the pediatric population, showing no significant difference (P = .415).
Discussion
This study identified a high proportion of patients screening positive for anxiety and depressive symptoms during a medical brigade in Santo Domingo, Ecuador. While these screening-positive rates appear higher than nationally reported prevalence estimates, they should not be interpreted as diagnostic prevalence and are not generalizable beyond this convenience sample.
Our study found that females, particularly in the pediatric age group, exhibited significantly higher rates of anxiety compared to males. Depression rates were also higher in females, although this difference did not reach statistical significance. Additionally, anxiety rates increased with age, while depression did not show a clear age-related trend. These findings are consistent with broader epidemiological trends, where anxiety and depression are more prevalent in females, especially after puberty.18,19
Cultural context is critical when interpreting self-reported mental health screening results in Latin America. Somatic expression of psychological distress, gender norms surrounding emotional disclosure, and stigma related to mental illness may influence how symptoms are perceived and reported. 9 Additionally, literacy barriers and variations in symptom interpretation may affect responses to ultra-brief screening tools such as the PHQ-4. These factors may contribute to both under- and over-identification of symptoms and should be considered when interpreting screening outcomes.
Importantly, this study does not establish the psychometric validity of the PHQ-4 in Ecuador. Although the instrument has demonstrated acceptable reliability and validity in other Spanish-speaking populations,13-17 psychometric characteristics may vary across cultural contexts. Studies have shown that effective screening tools, such as the Spanish version of the PHQ-9, have been useful in identifying depression in Ecuadorian public health settings. 20 The absence of local validation introduces the possibility of misclassification and false positives, which is acknowledged as a limitation.
The medical brigade context also introduces limitations, including convenience sampling, limited data control, and potential confounding related to non-systematic participation. These factors restrict generalizability and warrant cautious interpretation.
Conclusion
This study demonstrates the practical utility and feasibility of the PHQ-4 as a brief screening tool for anxiety and depressive symptoms in an underserved primary care setting in Ecuador. The PHQ-4 allowed rapid identification of individuals screening positive for mental health symptoms during a medical brigade, particularly among female and pediatric patients.
Future studies should focus on validating screening instruments within Ecuadorian populations, establishing normative data, and evaluating implementation in larger and more representative samples. Integrating routine mental health screening into primary care may support earlier identification and referral, particularly in settings with limited access to specialized mental health services.
Footnotes
List of abbreviations
PHQ-4 patient health questionnaire-4
GAD-2 generalized anxiety disorders
LMICs low- and middle- income countries
Author Note
This study was conducted in accordance with the ethical standards of the University of Kentucky and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Ethical Considerations
Ethical approval for the study was obtained from Institutional Review Board (IRB; IRB Exception #74994).
Consent to Participate
Informed consent was obtained from all individual participants (for pediatric participants, we obtained from their parent or legal guardian) included in the study.
Author Contributions
M.I. and T.Y. prepared and wrote the manuscript. M.J., R.A., P.B., and R.M have collected the data. A.S have analyzed the data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Availability of data and materials: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.*