
Abstract
Introduction:
Internally displaced persons (IDPs) in Nigeria face disproportionate mental health problems, yet rigorously designed epidemiological evidence in urban camps remains limited.
Methods:
A cross-sectional survey of 264 IDPs across 2 Abuja camps (Durumi and Wassa) employing culturally adapted Hausa and English versions of the Patient Health Questionnaire-9 and Generalized Anxiety Disorder-7 to assess anxiety and depression prevalence, severity, and correlates.
Results:
Moderate-to-severe symptoms affected 18.9% of participants for depression and 17.4% for anxiety. Multivariable analysis identified older age (≥35 years; adjusted odds ratio [AOR]: depression = 4.36; anxiety = 6.64), female sex (depression AOR = 2.36; anxiety AOR = 2.86), and absence of prior psychological counseling (depression AOR = 4.28; anxiety AOR = 2.96) as significant correlates. Generalized additive models revealed increasing symptom severity with age, with adjusted mean depression and anxiety scores rising from approximately 3.6 and 3.4 among younger participants to 7.1 in those aged ≥35 years. Sensitivity analyses using a negative-control outcome (communication language) and E-values assessed the robustness of the findings to potential unmeasured confounding and selection bias.
Conclusion:
By integrating rigorous bias assessment with locally grounded data, this study demonstrated the significant rates of anxiety and depression among internally displaced persons in Nigeria utilizing a culturally tailored mental health evaluation.
Introduction
Anxiety and depression are leading contributors to the global burden of disease, closely linked to functional impairment, diminished quality of life, and increased mortality.1-3 Risk is elevated in populations exposed to armed conflict, forced displacement, and chronic insecurity. 4 By the end of 2024, an estimated 123.2 million people were forcibly displaced worldwide, including 83.4 million internally displaced persons. 5 Unlike refugees, internally displaced persons remain within their country’s borders while experiencing comparable trauma, socioeconomic disruption, and barriers to care. 6
Nigeria exemplifies this challenge. Prolonged Boko Haram insurgency and escalating communal conflicts in the Northeast and Middle Belt have contributed to one of the largest internal displacement crises in Africa.7-9 By mid-2025, approximately 8.18 million people were displaced within Nigeria, the highest in West Africa and the 10th largest globally.5,10 Nigeria also ranked in the extreme tier of the 2024 Armed Conflict Location and Event Data Project Conflict Index, reflecting persistent violence, civilian targeting, and the presence of multiple armed actors. 11
Mental health symptoms are widespread among Nigeria’s IDPs amid prolonged conflict and displacement, with nearly 17.7% IDPs reporting moderate, 7.8% moderately severe and 0.9% severe depression and 20% meeting criteria for post-traumatic stress disorder (PTSD) in a 2024 survey of 2 Abuja IDP camps (Durumi and New Kuchingoro). 12 Although a growing body of quantitative research has examined mental health outcomes in Nigerian IDP populations,12,13 studies specifically employing advanced, methodologically rigorous epidemiological approaches to assess potential sources of bias, for example, unmeasured confounding, selection effects, or misclassification within urban camps such as those in Abuja, remain notably limited. This is particularly critical in contexts where intersecting factors of service access constraints and security risks complicate both mental health burden and research validity.
To address this gap, we conducted a cross-sectional survey in 2 urban IDP camps (Durumi and Wassa) in Abuja, Federal Capital Territory (FCT). We extend prior work in 3 ways: first, by estimating the prevalence and severity of anxiety and depression with Hausa and English language validated instruments; second, by applying sensitivity analyses that are infrequently used in this literature, specifically a negative-control outcome and E-value calculations, to assess robustness to potential bias, and third, by quantifying age- and gender-related gradients in symptom severity and interpreting them within Nigeria’s evolving IDP policy context. By pairing locally grounded data with these analytic checks, the study offers policy-relevant evidence to guide the integration of mental health and psychosocial support into humanitarian and primary care responses in Nigeria and in comparable conflict-affected settings.
Methods
Study Design and Setting
We conducted a cross-sectional survey in 2 IDP camps (Durumi and Wassa) in Abuja, FCT. Using household registers (Durumi: 387; Wassa: 743), 150 households per camp (300 total) were randomly sampled. One eligible resident per household was invited. Of 300 households approached, 264 participants enrolled (88.0% response). The sampling proceeded in 2 stages:
Household selection: Using the official household registers (Durumi: 387 households; Wassa: 743 households), we performed simple random sampling to select 150 households per camp (300 households total).
Respondent selection: In each selected household, field staff listed all eligible members (i.e, participants meeting our inclusion criteria) and randomly chose 1 individual to be surveyed. This probability-based approach ensured each eligible person had an equal chance of being the respondent.
Data Completeness and Missing Data
During the study, we verified that all questionnaire items were answered. No responses were missing for any of the analyzed variables. Our dataset was complete for all 264 participants who enrolled. Thus we conducted a complete-case analysis using the full sample.
Study Population
Participants were aged ≥13 years. Recruitment emphasized adults ≥18; adolescents aged 13 to 17 were enrolled when present with guardian consent and adolescent assent. No upper age limit was imposed; the oldest observed participant was 55.
Sample Size and Power Analysis
We conducted a priori power analysis assuming a 2-tailed test (α = .05) and 80% power to detect a moderate effect (Cohen’s d = 0.5) in mean PHQ-9 or GAD-7 scores between 2 groups. A minimum of 128 participants (64 per group) was required. Our final sample of 264 exceeded this, providing sufficient power for moderate effects, though smaller subgroup differences may require larger samples.
Participant and Community Engagement
Prior to the survey, we conducted qualitative engagement to adapt instruments and field procedures. Eight focus group discussions (n = 28; Durumi [4], Wassa [24]) and 18 key informant or in-depth interviews (Durumi [9], Wassa [9]) were held with IDPs, camp leaders, government officials (Federal Emergency Management Agency [FEMA] Nigeria)); National Commission for Refugees, Migrants, and Internally Displaced Persons; FCT Health Secretariat, Non-Governmental Organization (NGO) staff, health professionals, and researchers. Sessions addressed camp challenges, coping strategies, mental health needs, and delivery preferences. Transcripts were coded using conventional content analysis to thematic saturation. Findings informed Hausa translations, interviewer scripts, and logistics. Bilingual facilitators supported the process.
Psychiatric Symptom Scales
Depressive symptoms were measured with the Patient Health Questionnaire-9 (PHQ-9). Severity categories were 0 to 4, none to minimal depression; 5 to 9, mild; 10 to 14, moderate; 15 to 19, moderately severe; 20 to 27, severe. Anxiety symptoms were measured with the Generalized Anxiety Disorder-7 (GAD-7). Severity categories were 0 to 4, minimal; 5 to 9, mild; 10 to 14, moderate; and 15 to 21, severe.
Data Collection Period
Between April 1, 2024, and October 15, 2024, questionnaires were administered in either Hausa or English, according to each participant’s language preference.
Questionnaire
We recorded demographics (age, sex, education, employment status, primary communication language, state of origin), displacement characteristics (camp location and duration of stay [camp duration]), psychological counseling history, and symptom scores for anxiety and depression. Participants who preferred Hausa received adapted versions of the GAD-7 and PHQ-9 developed through forward translation, back translation, and cognitive debriefing. Participants who preferred English received the original English instruments. Item wording and scoring were the same in Hausa and English, and responses were pooled for analysis. In adjusted models, symptom scores did not differ materially by language, which supported pooling.
In Nigerian samples, the PHQ-9 and GAD-7 have demonstrated good internal consistency and acceptable construct validity (PHQ-9 Cronbach’s α approximately 0.85-0.93; GAD-7 Cronbach’s α approximately 0.71-0.82).14-17 In the present study, internal consistency was good for both scales (PHQ-9 Cronbach’s α 0.80; McDonald’s ω 0.81; GAD-7 Cronbach’s α 0.78; McDonald’s ω 0.79).
Statistical Analysis
The prevalence of moderate-to-severe anxiety (GAD-7 ≥ 10) and depression (PHQ-9 ≥ 0) was estimated as the proportion of participants meeting these thresholds. Categorical variables were summarized as counts and percentages, and continuous variables as means, medians, and interquartile ranges, stratified by age and sex. Multivariable logistic regression with robust standard errors was used to estimate odds ratios (ORs) and adjusted odds ratios (AORs). Adjusted models included camp duration, age group, sex, education level, employment status, and psychological counseling history. Generalized additive models (GAMs) were applied to quantify non-linear age-related gradients in symptom severity. 18 Sensitivity analyses, including a negative-control outcome analysis and E-value calculations, were used to assess robustness to selection bias and unmeasured confounding.19-22 A negative control outcome is a variable that is not plausibly affected by the factor of interest but is subject to similar sources of bias as the main outcome.19,20 Primary communication language (Hausa) was prespecified as a negative-control outcome. As the regional lingua franca across sociodemographic strata,23,24 it is not expected to vary systematically with key predictors, for example, age, sex, or counseling history in ways pertinent to anxiety or depression in this setting. Thus, any non-null association would indicate residual confounding, measurement error, or selection bias.19,20 E-values quantify how strong an unmeasured confounder would need to be to nullify an observed association.21,22
Analyses were conducted in Stata version 18.5 and R version 4.4.2, with statistical significance defined as P < .05. Reporting follows Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 25
Results
Sample Characteristics
Of the 300 households approached, 264 participants were enrolled (88.0% response). Ages ranged from 13 to 55 years. Women comprised over two-thirds (67.4%.) of the sample. Adolescents aged 13-19 years comprised 21.6% of the sample (57 of 264; 95% CI: 16.8 - 27.0), indicating that just under one quarter of respondents were younger participants and the remainder were adults. The mean age of participants was 26.2 years (SD 8.3; 95% CI: 25.2 - 27.2), with a median of 25 years and an interquartile range (IQR) of 20-31.5 years (Table 1).
Descriptive and Baseline Characteristics of the Study Sample.
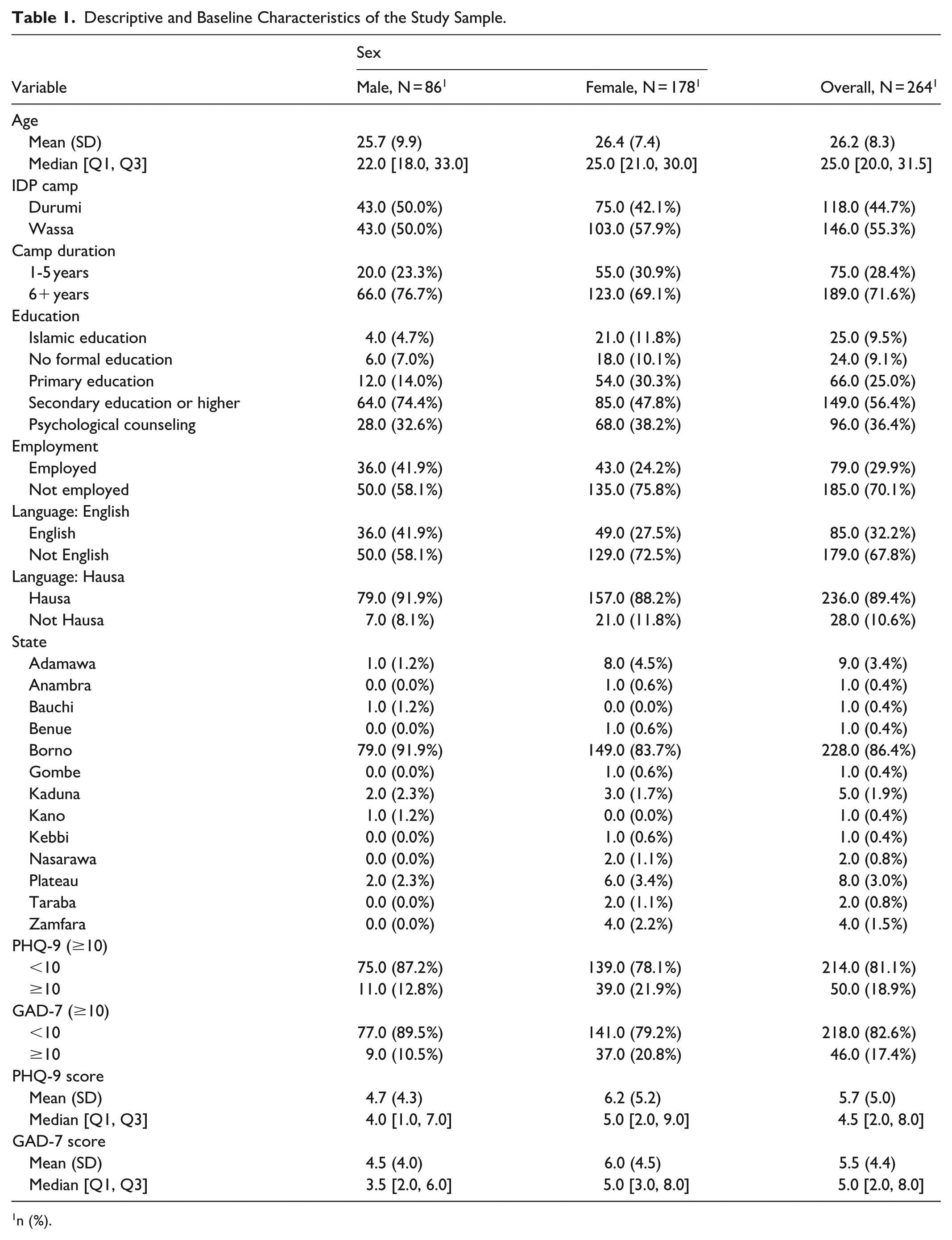
n (%).
More than a quarter of (28.8%, 76/264) the respondents had resided in the camps for 1 to 5 years, and 71.2% (188/264) reported residing for 6 years or longer (Table 1).
Prevalence and Severity of Anxiety and Depression
Symptom scores were mostly in the minimal to mild range. The mean PHQ-9 score was 5.72 (SD 4.99; 95% CI: 5.12-6.32), with a median of 4.5 and an IQR of 2 to 8. The mean GAD-7 score was 5.48 (SD 4.36; 95% CI: 4.95-6.01), with a median of 5.0 and an IQR of 2 to 8. Despite these relatively low averages, 18.9% of participants met the threshold for moderate to severe depression (50 of 264 with PHQ-9 ≥ 10; 95% CI: 14.4-24.2), and 17.4% met the threshold for moderate-to-severe anxiety (46 of 264 with GAD-7 ≥ 10; 95% CI: 13.0-22.5; Table 1).
Females (n = 178) reported higher symptom levels than males (n = 86). Median GAD-7 scores were 5.0 in females versus 3.5 in males, and median PHQ-9 scores were 5.0 versus 4.0, respectively. Mean scores also increased with age, particularly among females. Among adolescents aged 13 to 19 years, females had a mean GAD-7 score of 4.4 (SD 3.3) compared with 3.5 (SD 3.8) in males, and a mean PHQ-9 score of 4.9 (SD 4.7) versus 3.5 (SD 4.1). In the 20 to 24-year group, females averaged a GAD-7 score of 5.7 (SD 4.1) compared with 2.8 (SD 2.0) in males, and a PHQ-9 score of 6.0 (SD 5.1) versus 3.7 (SD 3.2). For participants aged 25 to 29 years, mean scores were GAD-7 5.5 (SD 4.2) in females versus 4.5 (SD 4.2) in males and PHQ-9 6.0 (SD 5.1) versus 4.4 (SD 4.1). Among those aged 30 to 34 years, females averaged GAD-7 6.8 (SD 5.2) compared with 8.1 (SD 6.3) in males and PHQ-9 6.5 (SD 5.2) versus 6.9 (SD 4.6). In participants aged 35 years and older, females reported a mean GAD-7 score of 7.9 (SD 4.9) compared with 6.3 (SD 3.6) in males and a mean PHQ-9 score of 7.9 (SD 6.0) versus 6.8 (SD 5.2). Overall, females bore a somewhat higher symptom burden than males, and both anxiety and depression scores increased with age, reaching their highest levels in the oldest group (Figures 1 and 2; Supplementary Tables S1-S4).

Density plots of median GAD-7 and PHQ-9 scores by sex.
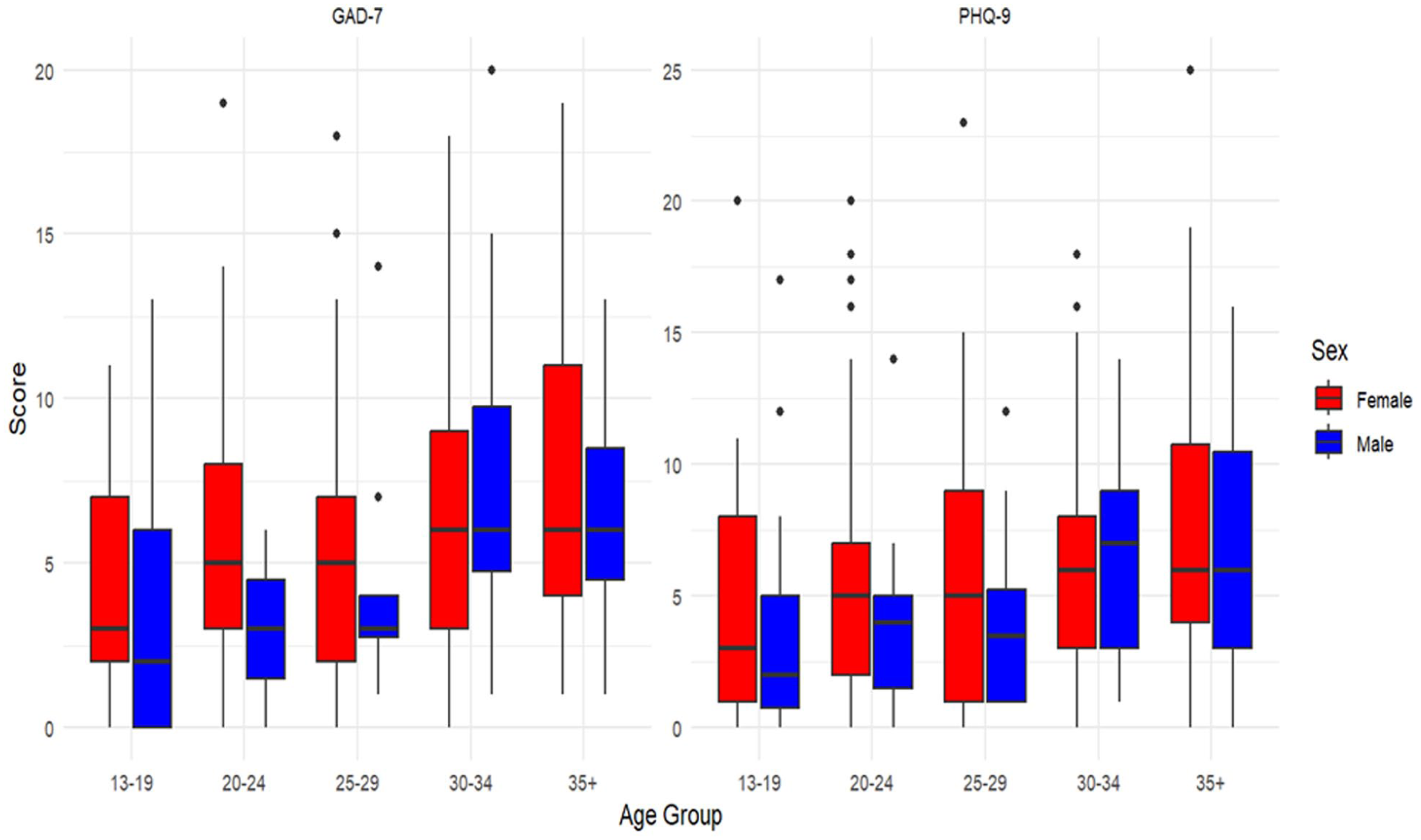
GAD-7 and PHQ-9 score distributions by age group and sex.
Associations With Demographic and Psychosocial Factors
In multivariable models, older age, being female, and no history of psychological counseling were associated with worse outcomes. Compared with 13 to 19-year-olds, participants aged ≥ 35 years had higher odds of both depression (AOR: 4.36, 95% CI: 1.48-14.32) and anxiety (AOR: 6.64, 95% CI: 2.11-24.12). Females had more than twice the odds of depression (AOR: 2.36, 95% CI: 1.05-5.63) and nearly 3 times the odds of anxiety (AOR: 2.86, 95% CI: 1.22-7.35) compared to males. Those without a history of counseling also had higher odds of depression (AOR: 4.28, 95% CI: 1.91-10.61) and anxiety (AOR: 2.96, 95% CI: 1.32-7.21). Estimates were imprecise with no statistically significant associations for camp duration, camp location, education, and employment status (Table 2; Figure 3).
Factors Associated with Anxiety and Depression in North-Central Nigeria IDPs (N = 264).


Forest plot showing factors associated with anxiety and depression in North-Central Nigeria IDPs (N = 264).
The events-per-variable (EPV) ratio was 4.2 for depression (PHQ-9 ≥ 10) and 3.8 for anxiety (GAD-7 ≥ 10).
Age Gradients in Symptom Severity
GAMs confirmed increasing symptom severity with age. Adjusted mean anxiety scores ranged from 3.38 (95% CI: 2.05-4.71) in the youngest age group to 7.05 (95% CI: 5.72-8.38) among those ≥35 years. Corresponding depression scores rose from 3.59 (95% CI 2.04-5.15) to 7.12 (95% CI 5.57-8.67) across the same age gradient (Figure 4).

Adjusted mean anxiety and depression scores by age group.
Sensitivity Analyses
Negative-control analyses indicated no strong evidence of residual confounding. Communication language (Hausa use) showed no statistically significant association with most predictors, besides counseling history and employment (Table 3). E-value calculations further suggested that substantial unmeasured confounding would be required to fully explain the observed associations of age, sex, and counseling history with mental health outcomes (Table 4).
Sensitivity Analysis: Hausa.
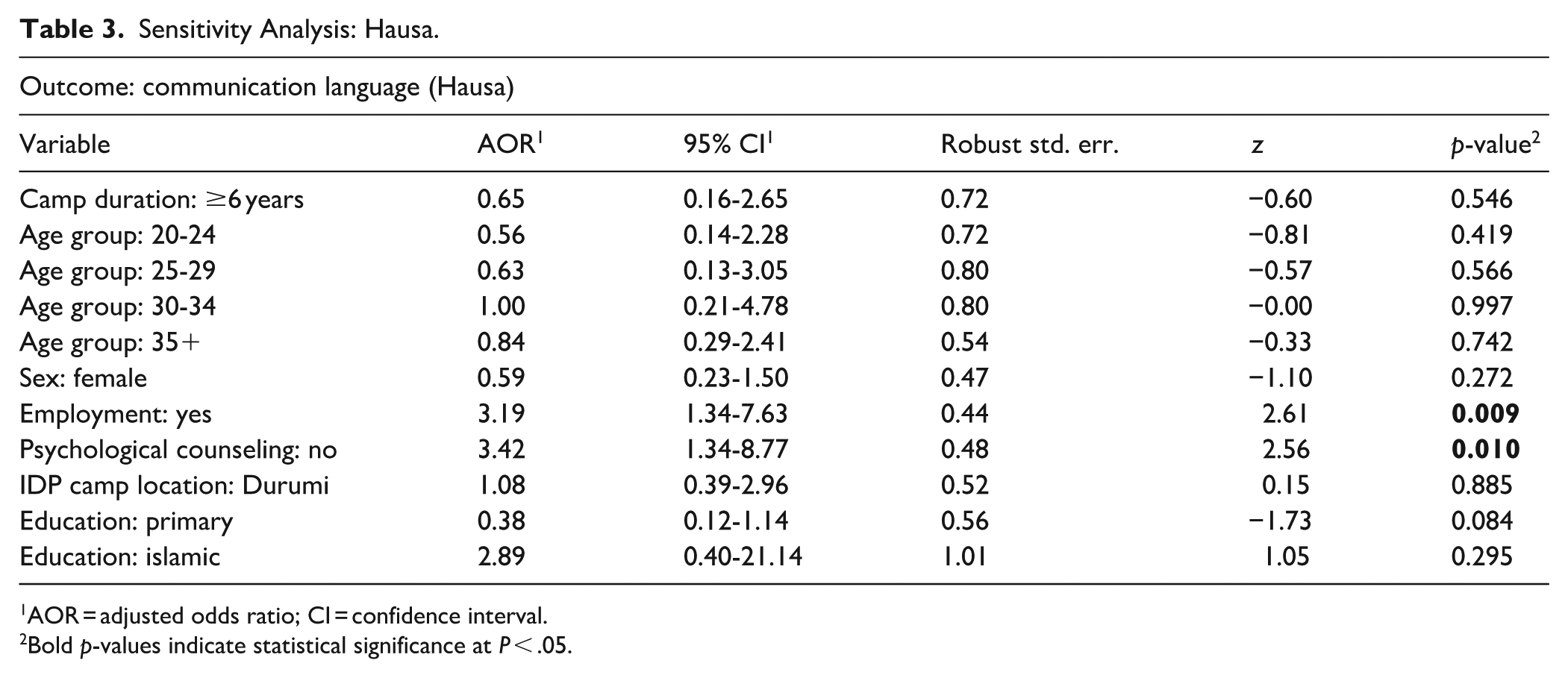
AOR = adjusted odds ratio; CI = confidence interval.
Bold p-values indicate statistical significance at P < .05.
Sensitivity Analysis: E-Values.

Discussion
This survey of 264 IDPs in Abuja’s Durumi and Wassa camps found moderate-to-severe anxiety in 17.4% of participants and moderate-to-severe depression in 18.9%, based on standard PHQ-9 and GAD-7 cut-offs. In a separate cross-sectional survey of youth aged 10 to 24 years in 2 Abuja camps (Durumi and New Kuchingoro; n = 637), 26.4% met the criteria for moderate-to-severe depression and 36.3% for PTSD. 12 Although differences in age composition limit direct comparison, both cross-sectional studies indicate substantial mental health needs in urban camps and underscore the importance of age-responsive psychosocial support.
Our camp prevalence estimates for moderate-to-severe anxiety and depression exceed the World Health Organization (WHO) threshold of 9.1% of conflict-affected individuals experiencing moderate to severe mental disorder (schizophrenia, bipolar disorder, moderate-to-severe anxiety, moderate to severe PTSD, and moderate-to-severe depression) at any point in time. 26 It is, however, lower than the rates often reported in protracted refugee settlements, where pooled prevalence of depression and PTSD often exceed 30%. 27 Studies from East African and Middle Eastern refugee camps have documented depression rates ranging from 30% to 50% and anxiety rates as high as 33% to 73%.28-30 Nonetheless, the substantial prevalence of moderate-to-severe anxiety and depression symptoms in Abuja camps reflects a significant mental health burden, indicating that urban proximity does not necessarily translate into improved psychosocial outcomes.31,32 Instead, factors such as overcrowding, insecure shelter, and economic precarity appear sufficient to sustain persistent distress among camp residents.9,33 This challenges the prevailing assumption that urban IDPs are better protected by access to health and social services. 34 While urban settings do offer meaningful advantages in terms of service availability and employment opportunities, substantial health disparities and persistent barriers to care continue to undermine the wellbeing of displaced persons in cities.35,36
Symptom burden was disproportionately prevalent among older adults and females. Severity rose sharply after age 35, consistent with evidence that cumulative livelihood disruption and prolonged uncertainty amplify distress over time. 37 Older IDPs in Nigeria often face sustained caregiving responsibilities without stable income, compounding psychosocial vulnerability. 38 Females experienced more than twice the odds of depression and nearly 3 times the odds of anxiety compared with males. This is consistent with WHO findings that depression is more common in females in humanitarian settings and with reports emphasizing the distinct socioeconomic hardships and displacement-related stressors faced by displaced Nigerian women.39,40 For instance, females in humanitarian contexts frequently face greater financial insecurity, caregiving burdens, and reduced access to education and employment opportunities compared to males, which contribute to increased psychological distress.39,40 These demographic gradients underscore the importance of tailoring mental health and psychosocial support (MHPSS) interventions to the specific risks faced by older adults and females, rather than adopting generic approaches.
Participants without a history of counseling reported greater symptom burden than those who had previously accessed services. While this might suggest protective benefits of counseling, the cross-sectional design prevents causal inference. It is equally plausible that individuals experiencing greater distress were more likely to seek services, a form of reverse causation. 41 Regardless of interpretation, the finding indicates that many vulnerable IDPs remain unreached by any form of psychosocial support. Given Nigeria’s severe workforce shortage, with fewer than 200 psychiatrists for a population of over 230 million, 42 scaling up task-shifted and peer-delivered interventions is essential to address unmet mental health needs.
A central innovation of this study was the application of bias sensitivity analyses rarely used in psychiatric research on forced displacement. We employed communication language (Hausa use) as a negative-control outcome, on the rationale that it was not plausibly affected by sociodemographic predictors in this context. Mostly weak associations with Hausa use suggest that unmeasured confounding is unlikely to fully explain our primary findings. We also calculated E-values, which quantify how strong an unmeasured confounder would need to be to nullify an observed association. The large E-values for age and gender indicate that only a very strong unmeasured confounder could negate these effects. While these diagnostics cannot fully eliminate potential bias, they offer a transparent and rigorous assessment of robustness that advances beyond purely descriptive surveys. Applying such methods brings greater epidemiological rigor to humanitarian mental health research and can serve as a model for future studies conducted in fragile settings.
This study’s findings underscore an urgent need to strengthen MHPSS for IDPs in Nigeria, particularly within urban camp settings such as Abuja’s Durumi and Wassa. Despite lower prevalence estimates compared to protracted refugee settlements, the substantial mental health burden identified calls for integrating MHPSS comprehensively into Nigeria’s National IDP Policy. 43 Such integration must emphasize not only clinical mental health care but also targeted interventions addressing social determinants of health, including shelter, water, sanitation, and security, that profoundly affect psychosocial wellbeing. 44
The severe shortage of mental health professionals in Nigeria necessitates pragmatic and scalable strategies. Evidence from Nigeria shows that task shifting is already feasible: contextualization and pilot implementation of the WHO Mental Health Gap Action (mhGAP) Program Intervention Guide 45 have enabled non-specialist primary care workers in Osun State to recognize and manage priority mental, neurological and substance use conditions, 46 large scale mhGAP training under the Mental Health in Primary Care (MeHPriC) program in Lagos State improved primary care workers’ knowledge, attitudes and reported clinical practice, 47 and qualitative work with community health volunteers in conflict affected North Central communities found generally positive views of task sharing, while also highlighting barriers such as financial and logistical limitations, timing of task allocation, and supply system hindrance. 48 Building on these experiences, expanding supervised task shifting, peer led group interventions and culturally adapted psychosocial programs in IDP camps represents a realistic approach to integrating mental health care into routine services in similarly resource constrained humanitarian settings.
In addition, digital health platforms offer promising avenues to overcome logistical barriers, with ongoing studies such as the RESETTLE-IDPs: Life-Skills Education and Psychosocial Resilience Building for Displaced Nigerians (RESETTLE-IDPs) trial investigating life-skills education delivered via mobile and in-person formats. 49 Community engagement and participatory approaches are vital. Actively involving IDPs in mental health program design and implementation can enhance cultural relevance, improve acceptability, and build sustainable capacity. Addressing stigma, promoting awareness, and ensuring the inclusion of vulnerable subgroups such as older adults and people with disabilities who experience disproportionate socioeconomic hardships and mental health risks are essential for delivering equitable and effective care.
Given the complexity of displacement-related vulnerabilities, multisectoral responses that integrate MHPSS with broader humanitarian and development interventions are critical to meeting evolving needs. Leveraging locally generated evidence, including findings from this and similar studies, can guide policymakers and humanitarian actors to prioritize comprehensive, context-sensitive mental health strategies that enhance resilience and wellbeing among Nigeria’s displaced populations.
Beyond policy relevance, this study contributes to how mental health in displacement is conceptualized. Much of the literature treats IDPs as a subset of conflict-affected populations. Our findings indicate that urban IDPs, even within a capital city, bear anxiety and depression burdens that exceed common emergency estimates yet remain below those reported in some protracted refugee settings, suggesting a profile distinct from both general conflict-affected populations and long settled refugee camps. Relative to WHO estimates for conflict settings of approximately 9% with moderate-to-severe common mental disorders and 22.1% with any mental disorder, 26 our camp prevalence of moderate-to-severe depression at 18.9% and anxiety at 17.4% is lower, perhaps due to differences in disorder aggregation and screening versus diagnostic definitions. Nonetheless, this supports a conceptual view in which urban displacement influences mental health not only through direct exposure to violence, but also via enduring disruptions to social, economic, and environmental stability.
Methodologically, we show how bias sensitivity tools can strengthen inference in cross sectional humanitarian surveys. We used a negative control outcome and E-values to gage the potential impact of unmeasured confounding and selection, clarifying whether demographic and psychosocial associations are likely to be robust without asserting causality.
Collectively, these results support a theoretical account that locates IDP mental health at the intersection of conflict dynamics and urban social and environmental determinants. This framing is consistent with evidence of Nigeria’s persistent, fragmented conflict landscape and clarifies why mental-health needs remain high despite proximity to services in urban settings.
Future Research Directions
Enhancing mental health research among IDPs in Nigeria requires closing key evidence gaps, with lessons that are relevant to similar constraints in other low-and-middle-income country (LMIC) settings. Future studies should prioritize longitudinal and pragmatic designs to clarify temporal patterns, for example whether symptoms change with prolonged displacement or after specific interventions. Stepped-wedge trials of low-cost therapies such as group interpersonal psychotherapy or problem-solving groups can provide clearer evidence of effectiveness. When randomization is not feasible, quasi-experimental approaches that leverage phased program rollouts can improve causal inference.
Measurement should extend beyond depression and anxiety to include PTSD, substance use, functional impairment, suicidality, and quality of life. PTSD commonly co-occurs with depression among displaced Nigerians, 12 so adding PTSD screening will yield a more complete picture. Standardized data on camp stressors, including crowding, water and sanitation quality, and security incidents, are needed so that individual symptoms can be linked to modifiable environmental conditions.
Improving tools and analytics is essential. Screening instruments should be culturally validated in Hausa and English, with testing for measurement invariance and differential item functioning across sex and age groups. Studies should pre-specify analytic plans, allow flexible functional forms for continuous predictors such as age, and report bias sensitivity analyses. In particular, the routine use of negative control outcomes and E-values can help quantify the plausibility that unmeasured confounding or selection would overturn observed associations.
The scope of research should expand beyond urban Abuja camps. Comparative sampling across Nigeria’s geopolitical zones, including rural and insurgency affected areas, will test whether the age and sex gradients observed here generalize. Out of camp and informal settlement IDPs should be included, with planned analyses for adolescents, older adults, and female headed households. Mixed methods designs can situate quantitative findings in lived experience by documenting local idioms of distress, stigma, coping, and help seeking.
Taken together, these directions move IDP mental health research beyond isolated prevalence snapshots toward a cumulative and comparable evidence base that supports program design and course correction. Prioritizing longitudinal cohorts, quasi-experimental and pragmatic designs, harmonized outcome measures, and routine bias sensitivity analyses will produce reproducible findings on what works, for whom, and under which camp conditions.
Living conditions in Nigerian IDP camps often involve crowding, insecure shelter, and limited water and sanitation. These stressors plausibly elevate anxiety and depression, which underscores the importance of linking individual symptom data to camp level indicators such as water reliability, sanitation quality, and population density. Given the severe shortage of mental health specialists, task shifting with trained lay counselors and peer supporters offers a practical path to expand care, especially when delivered in local languages and community settings. Existing studies, including ours, remain constrained by cross sectional design, reliance on self report, restricted geographic scope, and omission of PTSD and substance use. Brief screening instruments may also misclassify some cases. Notwithstanding, our findings provide a credible baseline. Studies that integrate camp environment metrics, longitudinal follow-up, and standardized bias sensitivity analyses can generate cumulative, comparable evidence to guide targeted improvements in services for displaced populations.
Limitations
This study has several limitations. First, the cross-sectional design precludes inferences about temporal order or causality. To mitigate bias, we incorporated prespecified bias-sensitivity analyses using a negative control outcome and E-values, which strengthen inference but cannot fully rule out unmeasured confounding or selection. Although the overall sample exceeded our a priori power target for detecting moderate effects, the number of outcome events was smaller, resulting in lower Events Per Variable (EPV) ratios in the logistic models; consequently, some subgroup estimates may be less precise. Second, outcomes were assessed using brief self-report screeners (PHQ-9, GAD-7) rather than diagnostic interviews. Despite strong internal consistency and careful translation, misclassification and social-desirability bias remain possible, and formal clinical validation in this population was not undertaken. Third, we did not assess other common comorbidities or consequences such as PTSD, substance use, suicidality, disability, or functional impairment. Fourth, the sampling frame was limited to 2 urban camps in Abuja, which may reduce generalizability to IDPs in informal settlements, rural areas, host communities, or conflict-affected regions. We also lacked standardized camp-level environmental measures, preventing direct linkage between individual symptoms and water, sanitation, shelter, or security conditions. Although the response rate was 88%, nonresponse could bias estimates if nonparticipants differed meaningfully. These constraints warrant caution in interpretation but also underscore the usefulness of the bias-sensitivity checks applied.
Conclusion
In a survey of 2 Abuja IDP camps, about 1 in 5 participants met thresholds for moderate-to-severe depression or anxiety, with higher burden among adults aged 35 years or older, among females, and among those without prior counseling. By pairing validated screeners with prespecified robustness checks, including a negative control outcome and E-values, the study provides bias sensitive estimates that increase confidence in observed associations without implying causality. Programmatically, the results highlight potential priorities, including scaling mental health and psychosocial support through task shifting and culturally adapted delivery, and addressing camp-level determinants such as shelter, water, sanitation, and security that sustain distress. The findings offer a credible baseline for adaptive service planning and for future work that links individual outcomes to standardized environmental metrics.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251406840 – Supplemental material for Anxiety and Depression Among Internally Displaced Persons in North Central Nigeria: Prevalence, Correlates, and Policy Implications
Supplemental material, sj-docx-1-jpc-10.1177_21501319251406840 for Anxiety and Depression Among Internally Displaced Persons in North Central Nigeria: Prevalence, Correlates, and Policy Implications by Andem Effiong Etim Duke, Bala I. Harri, Ihoghosa Iyamu, Chisom Obi-Jeff, Asmau M. C. Dahiru, Tunde M. Ojo, Umar Baba Musami, Jidda Said, Vincent I. O. Agyapong, Rita Orji, Sanni Yaya and Ejemai Eboreime in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
Andem Effiong Etim Duke’s work was supported by the Dr. Patrick Madore Traineeship through the Dalhousie Faculty of Medicine 2025 Graduate Studentship program.
ORCID iDs
Ethical Considerations
The study received ethical approval from Nigeria’s National Health Research Ethics Committee (NHREC/01/01/2007-18/01/2024) and the Health Sciences Research Ethics Board at Dalhousie University (REB #2024-7085). All procedures adhered to established human-subjects protections, including voluntary participation, culturally appropriate consent and assent procedures, strict confidentiality safeguards, and referral pathways for participants who reported distress or requested additional support.
Consent to Participate
This is an REB-approved study, all participant information was de-identified. and patient consent was not required. Informed consent was obtained from all participants and/or their legal guardian(s), with assent secured for minors (ages 13-17). Design, translation, and consent procedures were co-developed with IDP leaders and bilingual facilitators, consistent with the 2024 revision of the Declaration of Helsinki mandating meaningful participant engagement. 50 Participants who endorsed high distress or requested assistance were provided brief on-site support and referral information for mental health and social services. Participant data will not be shared with third parties.
Author Contributions
Andem Effiong Etim Duke: Writing – original draft, Writing – review & editing, Writing – final draft, Visualization, Methodology, Investigation, Formal analysis, Data curation, Project administration, Validation, Conceptualization. Bala I. Harri: Writing – review & editing, Validation. Ihoghosa Iyamu: Writing – review & editing, Validation. Chisom Obi-Jeff: Writing – review & editing, Validation. Asmau M. C. Dahiru: Writing – review & editing, Validation. Tunde M. Ojo: Writing – review & editing, Validation. Umar Baba Musami: Writing – review & editing, Validation. Jidda Said: Writing – review & editing, Validation. Vincent I. O. Agyapong: Writing – review & editing, Investigation. Rita Orji: Writing – review & editing, Validation, Investigation, Supervision. Sanni Yaya: Writing – review & editing, Validation, Investigation. Ejemai Eboreime: Writing – review & editing, Investigation, Conceptualization, Project administration, Funding acquisition, Validation, Resources, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Creating Hope in Conflict: a Humanitarian Grand Challenge; a partnership of the United States Agency for International Development (USAID), the Foreign, Commonwealth & Development Office, United Kingdom of Great Britain and Northern Ireland (FCDO), the Stabilization and Humanitarian Aid Department, Ministry of Foreign Affairs, of the Netherlands (NL MFA), and His Majesty the King in right of Canada (“His Majesty”) represented by the Minister for International Development of Global Affairs Canada acting through The Department of Foreign Affairs, Trade and Development of Global Affairs Canada (“DFATD”) with support from Grand Challenges Canada (grant number R-HGC-POC-2408-67370); and the Government of Canada, Canadian Institutes of Health Research, Institute of Population and Public Health (grant number PAA-192178). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset generated and analyzed during this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.