
Abstract
Background:
Non-medical drivers of Health (NMDOH) (e.g., discrimination, income) influence the health status of individuals and their families. In primary care, where clinicians are trained to provide continuous, comprehensive care to patients, there is increasing recognition of the complexity to treat patients impacted by adverse NMDOH. Addressing complex needs requires coordinated support from both healthcare and social systems to overcome socioeconomic barriers and improve outcomes. The purpose of this project was to identify barriers that clinic team members encounter when referring patients to resources.
Methods:
Focus groups were conducted with Primary Care Providers and staff (e.g., Social Workers) regularly tasked with referring patients to community organizations. Interviews were audio-recorded, transcribed, and analyzed.
Results:
Participants described 3 themes related to barriers: (1) PCPs Are Unaware of Appropriate Referral Processes and Services/Scope of Services Available Internally, (2) Constant Fluctuation of Community Resources Limit Access, and (3) Cost, Communication, Transportation, and Paperwork Limit Patient Access to Services. A fourth theme included participants’ recommendations for Solutions to Improve the Referral Process and Communication.
Conclusion:
Understanding the barriers between healthcare providers and community organizations can provide a guide toward improving referral protocols and access to resources, thus ultimately leading toward a more equitable community.
Keywords
Introduction
Non-Medical Drivers of Health (NMDOH) (e.g., education, income, access to healthcare) strongly influence the health status of individuals and their families.1-3 Primary Care Physicians (PCPs), who are trained to provide continuous and comprehensive care to individuals and communities, are increasingly recognizing the challenges of treating patients affected by adverse NMDOH. Their longitudinal, trust-based relationships with patients uniquely position them to offer holistic support to those facing complex social and health needs.4,5 However, physicians report lacking skills and resources to navigate NMDOH conversations and address them within clinical settings. 6
Addressing these challenges requires intersectoral collaboration for more effective and sustainable improvements for community health outcomes. 7 The Socio-Ecological Model (SEM) provides a conceptual framework for understanding this dynamic, as it depicts multiple levels (individual, interpersonal, community and organizational, policy and societal) of influence on human health behavior, thus influencing health outcomes. 8 According to the SEM, community organizations and the health care system represent community-level environmental factors that serve as critical resources for supporting patient self-management or prevention of chronic conditions.
Creating linkages between medical institutions, particularly Primary Care Clinics (PCCs), and social services agencies can support positive patient health behavior and mutually benefit patients and clinicians. 9 One method of creating linkages includes referrals systems between medical institutions and community resources. Successful referrals generally depend on the presence of external infrastructures that exist to support referrals.10-12 Within the clinic setting, protocols are created for clinic and social staff (e.g., physician champions, patient navigators) to identify patients who require support for a range of socioeconomic (e.g., food insecurity) and/or health issues (e.g., diabetes, high blood pressure, obesity) that are frequently tailored to vulnerable populations such as pediatric groups, and racial and ethnic minority groups.10,12-15
Previous qualitative data exploring the process of connecting patients to socioeconomic resources have primarily focused on clinic systems with specialized services or programs such as HIV, mental health, food insecurity, and diabetes education.15-18 Beidler19,20 identified several barriers associated with social service referrals from medical providers from the perspective of higher-level administrators, including tailoring referrals to individual patient needs, technological limitations, varying levels of staff engagement, developing and maintaining resource list, and measuring efficacy of referrals. While these barriers have been documented, these interviews reflect the perspectives of higher-level administrators rather than frontline staff that conduct referrals frequently. Grgurevic 21 reviewed 28 international studies and identified various facilitators and barriers in connecting patients with community resources including intrapersonal characteristics of providers and patients, professional practice, work environment, relationships, and external influences. Despite these insights, limited research has used qualitative methods to examine how broader primary care settings connect patients to social services from the perspective of clinic staff. Therefore, our team employed qualitative methods to explore the experiences of PCC staff, aiming to address the following question: What are the barriers primary care clinic team members in Bexar County face when referring patients to local community resources? Findings from this project can inform PCC settings on potential barriers impeding patients from accessing community resources, and guide interventions or quality improvement initiatives to facilitate referrals.
Methods
Setting
The activities were conducted at a PCC in San Antonio, Texas. Majority (60%) of the population in Bexar County are Hispanic. 22 The clinic is located in a low-income area ($23,231 is the median household income) in which residents face a 20-year lower life expectancy in comparison to more affluent areas in San Antonio, some of which are located roughly 5 miles from the clinic.23,24
Sample
Focus groups were conducted with staff members that are regularly tasked with referring patients to community organizations for social services, along with PCPs. Although not originally part of the recruitment plan, PCPs were included based on staff recommendations. PCPs identify patients in need and refer them to staff, who subsequently connect patients to community resources, positioning PCPs as the first step in the referral process. Each group (e.g., social workers, community health workers) was approached by the project investigator in person or through email to request their participation in the project. Participants were interviewed in groups based on their departmental division or teams, resulting in 4 different groups: 1 group of 3 social workers, a second group with 8 Community Health Workers (CHWs), a third group named “Advanced Primary Care” (APC) consisting of a variety of roles (e.g., case manager, Licensed Vocational Nurse) that provide additional support to patients with complex conditions; and the fourth group with 10 PCPs. The PCPs invited were chosen based on varied clinical experience, from second year resident physicians to faculty with more than 10 years of experience. We approached 33 potential participants, and 24 agreed to participate.
Procedure
As part of a quality improvement initiative, our team conducted an evaluation of the clinic’s connections to local community resources. We initially conducted focus groups to identify community organizations that had established relationships with the clinic, assess the strength of those relationships, and gather recommendations on organizations where ties should be strengthened or created. This information was intended to deepen our understanding of the clinic’s existing network and to inform more intentional partnerships. However, during the focus groups, participants primarily discussed the barriers they faced when referring patients to community resources rather than current organizational ties. Project activities were completed between November 2022 and February 2023. Participants completed focus group interviews in either English or Spanish, lasting between 45 min and 1.5 h. Participants consented to audio recording of the focus groups and were paid $60 for their time. The Institutional Review Board (IRB) at The University of Texas Health Science Center at San Antonio approved this project: HSC 20220234NRR.
Analysis
The team consisted of a bilingual (English and Spanish) Researcher and DrPH student, along with a faculty research mentor. Interviews were transcribed by a trained intern. All interviewers were de-identified. A thematic analysis was used to analyze focus group data and explore emerging themes based on participants’ responses, using ATLAS.ti software. Thematic Analysis has been employed to evaluate a variety of public health and clinical related topics, and when applied correctly has shown dependable and confirmable data. 25 Inductive and deductive approaches were employed to guide development of the codebook.
During the first round of coding, the researcher reviewed transcripts line by line, applying codes as patterns arose, and discussing codes with faculty mentor. A second round of coding involved grouping similar codes, eliminating duplications, and reviewing the literature to refine codes. Themes were created through the grouping of codes. The final themes were reinforced with illustrative quotes from transcripts, a literature review, and descriptions to conceptualize the final themes.
Results
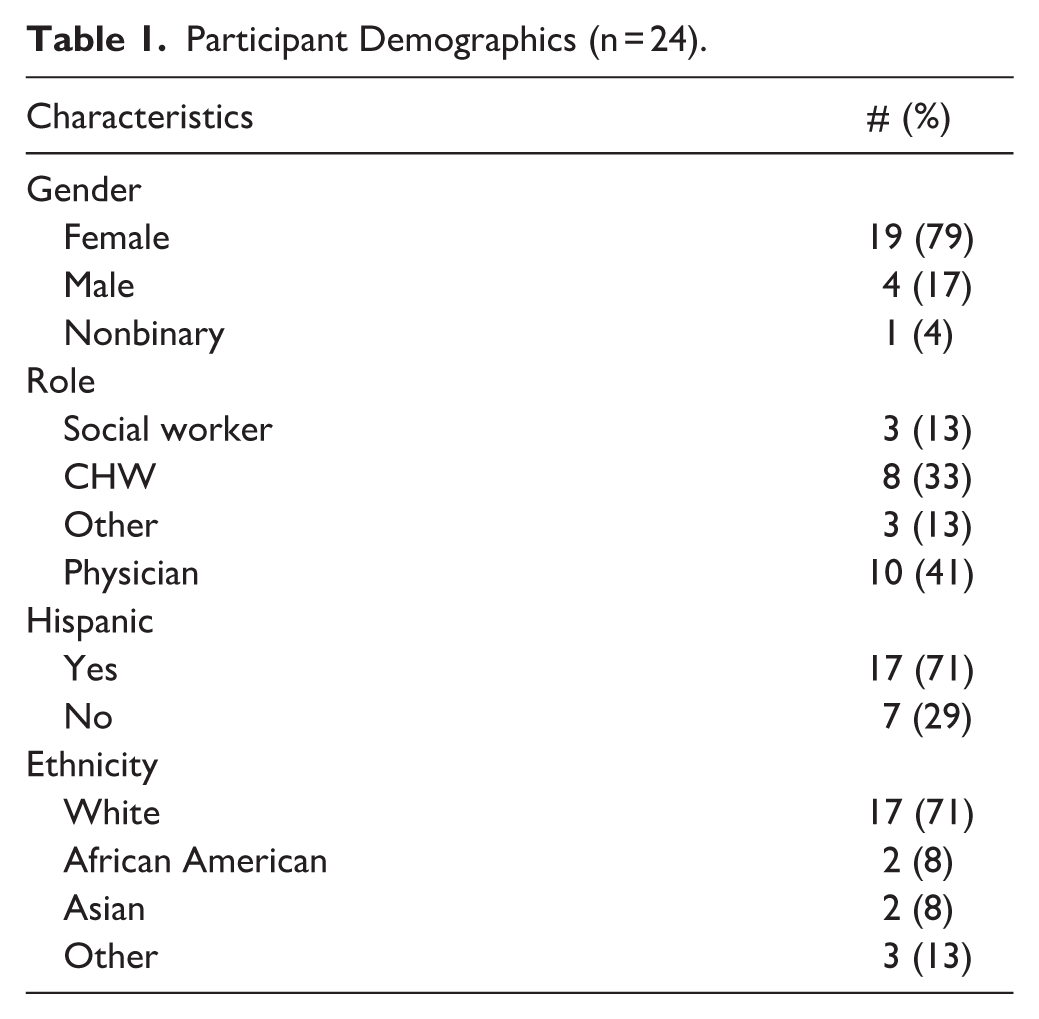
A total of 24 participants participated in focus groups including 8 CHWs, 10 PCPs, 3 social workers, an LVN, a case manager, and a health educator. Most participants identified as female (79%) and Hispanic (71%). Table 1 includes additional demographic information of participants.
Participant Demographics (n = 24).
Participants described 3 themes related to barriers: (1) PCPs Are Unaware of Appropriate Referral Processes and Services/Scope of Services Available Internally, (2) Constant Fluctuation of Community Resources Limit Access, and (3) Cost, Communication, Transportation, and Paperwork Limit Patient Access to Services. A fourth theme included participants’ recommendations for Solutions to Improve the Referral Process and Communication.
Theme 1: PCPs Are Unaware of Appropriate Referral Processes and Services/Scope of Services Available Internally
Staff described disconnect in receiving internal referrals from PCPs. For example, PCPs referred patients to staff without instruction. This places an additional burden on staff to figure out the reason the patient has been referred before addressing the patient’s problem:
The frustrating part.. [PCPs] send a blank referral. They don’t tell you what they are sending [the patient] for. [Patients] don’t know what they came for, so now we play twenty questions. . . I want to be efficient. Social Worker 1
Another form of disconnect from PCPs is in understanding the realities of the resources available and the extent these services will solve patient needs:
[PCPs] tend to think that there is a lot more help than there is. That’s. . .the assumption, they assume that a clearly disabled person will get disability, they assume that someone on disability can survive on it, they assume that someone asking for help that [is] getting evicted is going to have plenty of time to find rental help, and a lot of the time it seems like a reasonable request [but] it’s actually not. Social Worker 3
This assumption leads to PCPs referring patients to staff misguidedly. Social Worker 1 describes patients lining up at the social work department expecting their concerns to be immediately resolved:
. . . Patients. . .show up to the department and state “the doctor said you can get me disability or SNAP”. [The PCPs] are passing the buck for patients to argue with staff members, placing another burden onto their daily tasks by having to emotionally manage and de-escalate frustrated patients who believed staff members were going to solve their immediate needs.
PCPs, themselves admit to this disconnect in understanding how to properly refer patients. Provider 9, resident physician, admits “I don’t know where [patients] go to. I hope. . . if I refer to social worker, I just pray and hope. . . they’re going to someone who can take care of that issue.”
Theme 2: Constant Fluctuation of Community Resources Limit Access
Participants identified several causes of community referral disconnect, including the frequent fluctuation of community resources. Staff noted that at times services are often unavailable or limited. CHW 4 describes “They have a lot of places with services but when you call, they never have it. . . my patients. . . don’t get help because they run out of funding.”
Another frustration related to the constant fluctuation of resources is the lack of communication when services have been depleted or reached capacity. If staff members are aware, they’ll reprioritize other forms of assistance:
There is no communication of what there is and. . . isn’t . . . we know that organizations run dry but let us know, because if we don’t know, we’re going to keep calling. CHW 2
When asked if having a point of contact at a community organization increased chances of patients receiving services, participants reported this rarely facilitated access. One reason being that staff turnover rates are high among community organizations. Social Worker 3 describes “Some folks drop out so often. The changeovers. [In one organization], my contacts are not the same, [they] have gone through three company names, two ownership changes. Six months ago, it was completely different.”
Theme 3: Cost, Communication, Transportation, and Paperwork Limit Patient Access to Services
The clinic staff members reported that many patients experienced their own barriers such as cost of services. Although community organizations offer low-cost services, the cost may still be deemed too high as individuals seeking services already have financial limitations:
I mean the resources are there, its just not sufficient. . .they cost money and folks don’t have money. . . I have had folks who say, “I’m not going to pay $20 for counseling.” Social Worker 2
Reliable transportation is another barrier for patients with financial constraints. The need to arrange transportation, through personal networks or local services, adds an additional burden and reduces the likelihood the patient will seek necessary services:
. . .some that don’t have transportation to get to these places. And that’s the hard part. . .[the patient will say] “yeah, you’re gonna send me here, I’ve been sent there before but how am I gonna get there?” LVN 1
Another barrier reported by participants is patients feeling frustrated about having to continuously follow up with community organizations. CHW 3 describes “When you call by phone, lot of the patients get anxious, if they have mental problems and they tell us they are calling and no one is answering. . .and are left with answering machine.” Services are often sought during times of immediate need, making it particularly overwhelming for patients when follow-up efforts are met with no or delayed responses.
Paperwork can be overwhelming as many patients with low socioeconomic status also experience low literacy, and the complexity of required paperwork can deter them from seeking services. Health Educator 1 describes “a lot of them. . . go and they get help but there’s so much paperwork they have to sign, they don’t want to do it. And then it falls off and then we’re back at square one with them again.”
Theme 4: Solutions to Improve the Referral Process and Communication
Participants discussed wanting to have bidirectional information on patient progress. Staff would like to know if patients received services from the organizations referred to and the outcome of these services. Such information could support more effective follow-up and allow for reassessment of patients’ immediate needs based on the success and scope of services received by the patient:
You just want to know the outcome, like what happened. . .? Yes, [patient] took the services. No, they didn’t. . .That’s pretty much. . . the extent of feedback we get. LVN 1
PCPs voiced similar feedback as they would like status updates when referring patients internally (e.g., social workers) and to know outcome of referrals:
If there could be. . .where [it] tells you the status of everything just like for other referrals. [For medical] referrals, it’ll say pending or. . .appointment made. . . PCP 2, resident physician.
PCPs also suggested implementing a team-based approach by training the entire clinic to complete referrals when coming across patients with socioeconomic needs:
We should do all a team-based approach. . . I think we should train the whole team from intake [registration], [Medical Assistants]. Everyone should be. . . getting opportunity to do referrals. . . PCP 1, faculty physician.
A few participants indicated there should be an updated directory with currently available resources. As resources are depleted or restructured, communication on funding shifts will be essential to an efficient patient referral process:
Have a list [of resources].. that are actualized. . .But there is no communication within the agencies, and I think that is very important. They can say, [they] ran out of money, [so] can we refer to others. . .. CHW 2
Discussion
Our team explored the challenges of clinic staff and PCPs in connecting patients to community resources. Four main themes emerged: (1) lack of clarity among PCPs on referral procedures and internal services; (2) the instability of community resources; (3) systemic and patient-level barriers including cost, transportation, communication challenges, and burdensome paperwork, and (4) solutions recommended. Together, these themes highlight a fragmented referral system that complicates efforts to address patients’ social needs.
Similar to Valaitis, 26 PCPs and clinic staff often experienced frustration when attempting to address patients’ social needs due to external barriers such as patients’ financial constraints and transportation issues, fluctuations in the availability of community services, and associated paperwork. Consistent with research by Give, 27 participants emphasized the need for feedback loops between referring clinics and receiving organizations—suggesting that timely updates on referral outcomes are critical for effective follow-up care. Additionally, our participants revealed that PCPs’ limited understanding of referrals and the scope of available services placed an added burden on staff, who must not only address patients’ care needs but also bridge gaps in provider knowledge to ensure appropriate referrals are made.
These challenges can be further understood through the lens of the conceptual model proposed by Grembowski. 28 In the context of our project, this complexity emerges when the healthcare system’s capacity to address NMDOH falls short, thus resulting in gaps in care and unmet patient needs. Our findings illustrate how limited provider knowledge, inconsistent community resource availability, and patient-level barriers all contribute to this misalignment.
To address these challenges, participants recommended solutions such as team-based training on referral protocol, maintaining a regularly updated directory of community resources, and implementing feedback mechanisms to track referral status. These changes could improve coordination and ensure that referrals lead to meaningful outcomes. Furthermore, in line with Lian, 29 our results suggest that the structure of community services (e.g., availability of walk-in or phone-visit) can significantly influence patient follow-through. Community resources requiring multiple steps (e.g., applications, proof of documentation) were perceived as more difficult for patients to navigate, especially those facing literacy, language, or transportation barriers. Community resources, when well-integrated and easily accessible, can serve as a bridge to close the service gap for patients facing socioeconomic challenges.
Limitations
Limitations of this project include recruitment from a single clinic site and many of the participants were representative of San Antonio, Texas, a majority Latino population. Transferability of results may only extend to similar clinical or community settings. In addition, given that the focus groups were conducted within 1 clinic, social desirability or power differentials within groups may affect the disclosure of information. To help mitigate this potential limitation, we stratified the focus groups by role.
Public Health Significance
Guided by the SEM, this project reinforces that patients cannot manage health conditions independently; but require sustained support from multiple interacting levels to improve health outcomes. 8 Patients face a variety of barriers in their daily life to implement positive health behaviors, particularly individuals facing adverse NMDOH. There is vast literature on improving patient health outcomes through education on positive health behaviors (e.g., fruit and vegetable consumption, physical activity) and overall improving health literacy. 30 At the interpersonal level, social networks play a pivotal role in influencing health behaviors, as these relationships can either provide a supportive or negative social environment for patients to achieve their health goals. 31 At the organizational level, our findings highlight the influential role of healthcare systems on patients’ ability to access and utilize resources that can help support positive health behaviors. A fragmented referral infrastructure and internal processes within healthcare organizations contribute to delays in patient access to community-based services. In addition, this fragmented system extends to community relationships. At the community level, strengthening partnerships and networks between healthcare organizations and community-based services can streamline referral pathways and lessen the burden placed on patients to navigate complex systems independently. Improved coordination at this level supports more timely and equitable access to resources. 13 Further research should examine interventions that strengthen both internal organizational processes and external community partnerships to optimize referral systems. Lastly, at the societal level, policies that fund and support community-clinical pathway implementation and evaluation provide an opportunity for a systemic level solution toward improving community health outcomes. 32
Footnotes
Acknowledgements
The authors would like to acknowledge Ludivina Hernandez for sharing feedback on interview guide based off her experience as a Community Health Worker.
Ethical Considerations
The Institutional Review Board (IRB) at The University of Texas Health Science Center at San Antonio approved this project: HSC 20220234NRR.
Consent to Participate
All participants verbally consented to participate in the interviews.
Consent for Publication
Not applicable.
Author Contributions
Jasmine Rodriguez, MPH designed and implemented project, and led manuscript development.
Tharani Ravi, MD assisted with manuscript writing.
Erika L. Thompson, PhD assisted with manuscript editing and feedback.
Robert L. Ferrer, MD, MPH provided feedback on project design, assisted with analysis, and feedback on manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this work was made possible by a Community Engagement Small Project Grant (CESPG) Award from the Institute for the Integration of Medicine & Science (IIMS) at UT Health San Antonio.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Participants did not authorize for sharing of their data.