
Abstract
Introduction/Objectives:
This study aimed to clarify what primary care physicians (PCPs) in Japan understand of the role of physical therapists (PTs) through the experience of working with PTs in hospitals, and what roles PCPs expect for PTs in future primary care.
Methods:
Semi-structured interviews were conducted individually with 9 purposively sampled PCPs with sufficient experience of collaboration with PTs. Interview data were analyzed by theme analysis focusing on “What does the PCP understand about the role of PTs through the experience of working with PTs in hospitals?” and “What roles and purposes does the PCP wish for PTs in primary care settings?”
Results:
PCPs viewed PTs as providers of rehabilitation in the traditional medical model, and understood their role as an occupation having a mono-causal viewpoint, namely a specific and well-defined outcome for individual patients, and intervening with patients within a short clinical course with the aim of improvement or maintenance of the patient’s condition. With regard to future primary care, PCPs expected that PTs would interpret various factors related to patient lives from the viewpoint of causal interactions; become important stakeholders in the community; and respond flexibly to patients and the environmental factors around them with continued support to the individual.
Conclusions:
PCPs understood the role of PTs in hospitals as “Rehabilitation in the traditional medical model,” and expected the future role of PTs in primary care as “Rehabilitation in integrated community care.”
Introduction
While population aging is accelerating in many countries, a trend toward increasing complexity has been identified not only in disease-related issues such as the growth of elderly populations with multiple diseases,1,2 but also in biopsychosocial issues in community residents.3,4 For these reasons, the necessity for primary care, as well as for special treatments at large hospitals, has been increasing. Among the chief complaints of patients presenting at primary care clinics and hospitals are those related to non-internal medicine. 5 In particular, many patients suffer from skeletomuscular symptoms that can disturb their daily activities.6-8 Therefore, the primary care physician (PCP) is required to have a broad range of knowledge and skills, not only regarding medical interventions but also rehabilitation-related care, including daily activity guidance and advice on the living environment. However, there are limitations on the provision of rehabilitation-related guidance and advice for patient families, because physician-nurturing programs lack training about rehabilitation, 9 and per-patient consultation times in outpatient care are limited. In this situation, it is expected that physical therapists (PTs), who specialize in rehabilitation, will intervene not only in the care of hospitalized patients but also care for patients in need of primary care, including outpatients and homecare recipients, in collaboration with PCPs, to allow community residents to continue enjoying an active life even with diseases or disorders. In Japan, however, an appropriate role for PTs in primary care has not been established.
In this study, we used role theory 10 as a theoretical framework for thinking about the role of PTs in future primary care. In role theory, people are assumed to have mutual role expectations for the behavior of self and others as members of a group society. 11 To increase role performance efficiency based on role expectations with regard to relations with others, it is necessary to first understand the role expected by others. Utilizing role theory to clarify role expectations for professionals in the context of health care could prove a valuable framework for increasing role performance efficiency.12-14 Therefore, through this study, by clarifying the role that PCPs expect PTs to play in primary care, it may be possible for PTs to assume that role in primary care in the future. Previous studies have shown that PTs must advocate for regular physical activity as a key component of the treatment of chronic diseases in all patient interactions. 15 Consistent with this, PTs have been reported to assume role expectations in the prevention of chronic diseases, disorders, and early deaths in community residents, including physical activity approaches to patients with type 2 diabetes, anti-smoking counseling,16,17 and health promotion through improved physical activity in obese and other patients.18,19 However, many of these earlier studies reported the roles of the PT as expected by PTs themselves, and few published reports have considered the role expectations held for PTs by other primary care providers.
This study was designed to clarify what PCPs, as medical professionals with comprehensive and persistent relevance to patients and their families in actual primary care settings, understand of the role of PTs through the experience of working with PTs in hospitals, and what roles PCPs expect for PTs in future primary care. Clarification of role expectations for PTs in primary care held by PCPs is likely to help define roles deemed normative for PTs in the historical hospital model, and identify new roles that will contribute to the healthcare system in the coming era.
Present Status of PTs in Japan
The Japanese Physical Therapy Association was founded in 1966 and as of 2019 had 132 000 members (104.6 per 100 000 persons), of whom 37% were women. Their breakdown by workplace in descending order is hospitals (59%), homes (18%), nursing homes (9%), clinics (8%), and training and research facilities (2%). 20 In Japan, PTs cannot provide physical therapy interventions to patients/users without the direction of an attending physician. In addition, unlike the case in the United States and other countries, practice scope is restricted by legislation, and training for autonomous practice is not provided. Note that PTs are involved in home healthcare mainly in the form of home-visit rehabilitation; specifically, PTs affiliated with a hospital, clinic, home-visit nursing station or elsewhere visits the patient’s home under the direction of the attending physician and provide physical therapy at or near the home.
Present Status of Primary Care and Related Physicians in Japan
The Japanese medical system lacks the type of registration scheme that is applied in primary care systems outside Japan. Since the patient is allowed to freely select and change physicians and medical facilities, it is difficult to maintain practice continuity under the control of any one physician. In addition, hospitals now provide primary and secondary medical services, since hospital medicine has long been the mainstream of medical care in Japan. This is reflected in the fact that 30% of the approximately 7 million estimated outpatients per year present at hospitals. 21 A new 2-year residency training system started in 2004 allows trainees to undergo rotational training at various departments in a hospital, and to acquire essential skills for medical practice. To nurture physicians with the essential abilities of primary care, primary care specialists have been certified since 2010 through Japan Primary Care Association (JPCA)-accredited senior training for 3 to 4 years. This certification includes opportunities to learn rehabilitation with a focus on primary care. At present, 1067 certified family physicians are engaged in outpatient/inpatient practice, home healthcare, and other tasks. 22
Methods
Research Methodology
This study used a general inductive approach for the analysis of qualitative data based on semi-structured individual interviews.
Research Setting and Participants
Purposive sampling was adapted. The subjects were board-certified members of the JPCA or JPCA-certified family physicians who were engaged in primary care in Japan, and had sufficient experience of collaboration with PTs in hospitals. Nine PCPs were purposively selected using email based on community characteristics, faculty of practice, and years of experience. In Japan, although there are few PCPs working with PTs who meet the inclusion criteria, individual in-depth interviews were conducted by one of the researchers (JH or SO). At the start of the interview, they were fully informed of the objective of the study and that they would not be disadvantaged if they declined participation.
Data Collection
The first author (RG) is a PT, and the co-authors (JH and SO) are PCPs. RG and SO received training in qualitative research after obtaining their PhD degrees, while JH received this training as part of a PhD program. One of the co-authors (JH or SO) conducted each semi-structured individual interview (Figure 1) face-to-face or via videophone between November 2018 and February 2019. To minimize differences among interviewers, the 2 interviewers underwent adequate training, which included prechecking interview contents and alternating roll-playing as interviewer and interviewee.

Interview guide.
Interviews lasted 33 to 86 min. The participants were asked how they viewed the PT profession, why they felt so, and what roles they expected of PTs in primary care settings. Data were collected until saturation was reached, and all audio records of each interview were transcribed verbatim, which the researchers commissioned to agencies that specialize in transcribing. The verbatim record was analyzed by the first author (RG). RG generated the initial codes, and the validity of the findings was discussed with a co-author (JH). All authors then discussed the codes and themes, and reached an agreement on the final themes. Interview data were analyzed by theme analysis 23 focusing on “What does the PCP understand about the role of PTs through the experience of working with PTs in hospitals?” and “What roles and purposes does the PCP wish for PTs in primary care settings?” (Supplemental Table S1).
Ethics Approval
This study was approved by the Ethics Committee of the Faculty of Medicine, University of Tsukuba (approval number: 1327). All study participants provided informed consent, both in writing and verbally, after being given an explanation about the purpose and methodology of the study, that study participation was voluntary, and the protection of personal information.
Results
Participant profiles are listed in Table 1. The mean duration of clinical experience was 13.3 years. One theme emerged through the analysis of (a) How do PCPs understand the role of PTs through their experience of working with PTs in hospitals?: (1) Rehabilitation in the traditional medical model. In addition, 3 sub-themes were extracted from this theme. In contrast, one theme was explored for (b) What roles do PCPs wish for PTs to take and for what purposes in primary care settings?: (1) Rehabilitation in integrated community care. Three sub-themes were extracted from this theme also (Tables 2 and 3).
Profile of Research Participants.

F, female; M, male.
Theme, Sub-theme, and Representative Texts (a).

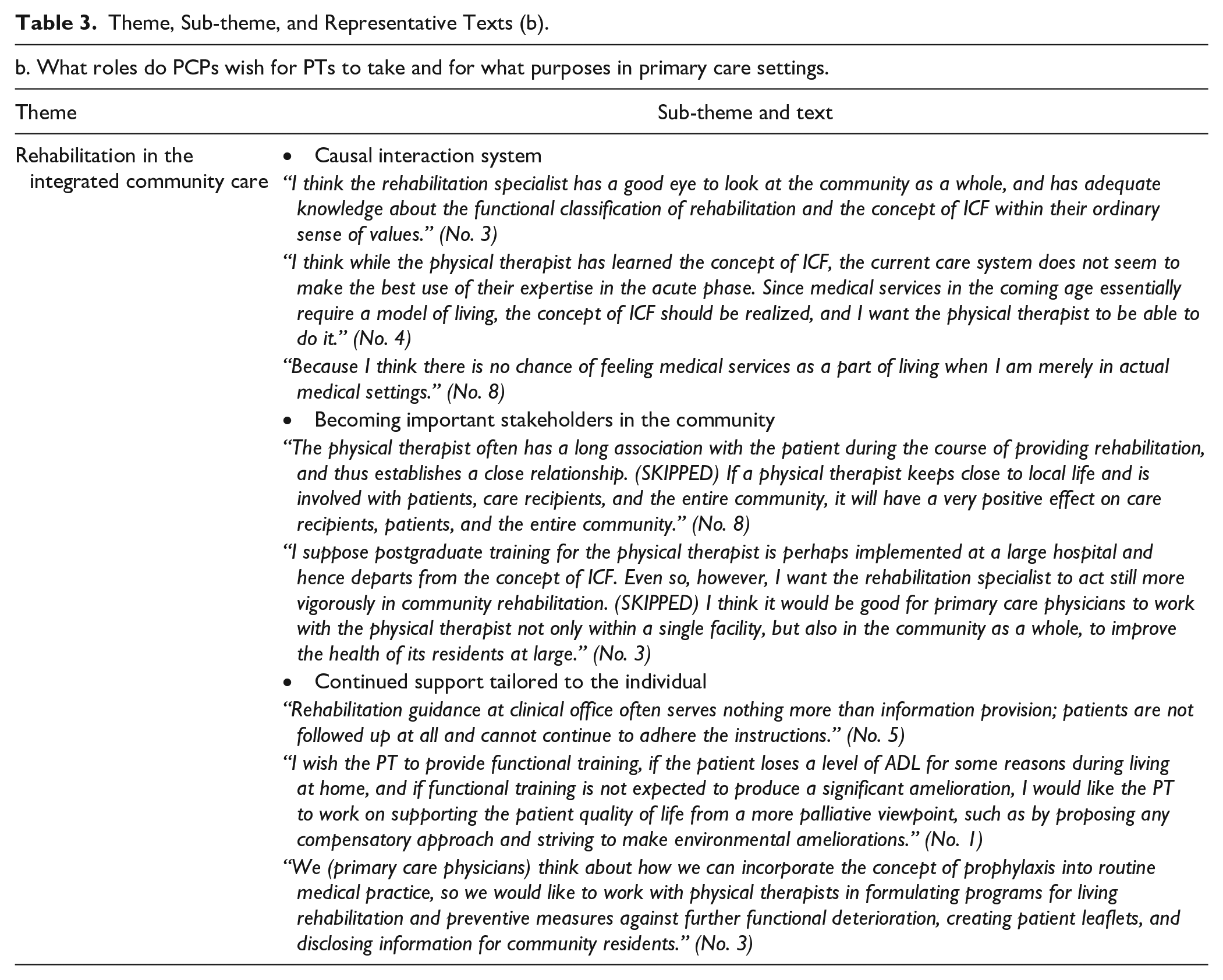
Theme, Sub-theme, and Representative Texts (b).
How Do PCPs Understand the Role of PTs Through Their Experience of Working with PTs in Hospitals?
Although the PCPs who participated in this study shared the same experience of having undergone their initial training mainly at hospitals, their current workplaces ranged widely, including clinics and hospitals. They were asked to remember their collaborations with PTs at hospitals, including during their training period, and to respond to some questions about their understanding of the PTs’ roles. As a result, “rehabilitation in the traditional medical model” was identified as a study theme. The theme was divided into 3 subthemes: (I) mono-causal system, (II) specific and well-defined outcome for the individual, and (III) short clinical course for improvement or maintenance.
Mono-causal system
The PCPs perceived the PT as a specialist in physical structural aspects, such as muscle strength and joint range of motion and action capabilities, such as walking, within the typical medical model in which hospital specialties are often sub-divided. In particular, those working with PTs at hospitals understood physical therapy as a specialized occupation engaged in patient care from a mono-causal viewpoint between physical structures and action capabilities. Namely, PCPs considered the role of PTs as increasing the walking and other mobility capabilities of patients with deficits in these areas due to hospitalization or other reasons through training to improve physical function.
“I imagine the physical therapist works to simply strengthen muscles, and to provide training for walking and fall prevention.” (No. 9)
Specific and well-defined outcome for the individual
The PCPs clearly perceived physical therapy as “an occupation providing exercise therapy to promote the post-discharge life of inpatients,” and considered that the major outcome that should be targeted by physical therapy was to improve the patient’s walking ability. Physicians viewed inpatients in the context of discharge as the target outcome. They evaluate the patient function of “walking” as a criterion for making a discharge decision. They may have expected the PT to attain this easy-to-understand outcome of “walking.” This situation was interpreted as follows: the PCPs repeatedly experienced sharing information on walking outcomes with the PT; and as a result, they might have developed their role recognition of PTs on this basis.
“I think the main specialty of the physical therapist concerns walking. I am convinced that the physical therapist is thinking about “how to make the patient able to walk and conditions in which the patient can walk.” (No. 2)
Short clinical course for improvement or maintenance
The PCPs viewed PT as a specialized occupation which aims to improve (or maintain) the patient’s physical functions within the specified hospital stay in acute-phase hospitals which implement the Diagnosis Procedure Combination (DPC) system. The DPC system is Japan’s flat-fee payment system for acute inpatient care. Introduced in April 2003, it specifies a hospitalization period for each disease.
24
Accordingly, the PCPs who had been trained at hospitals expected PTs to work to improve the activities of daily living (ADL) of patients who had been affected by acute disease. The hospital environment may have created an ideal specialist style of PT which leads to an ideal linear amelioration of physical functions directed at the short-term goal of hospital discharge.
“The physical therapist works for inpatients to prevent disuse syndrome by helping them to expand or maintain the range of motion early after admission and increase muscle power within a condition of an overall improvement in health, and to retain muscle power for ADL prior to entering the nutrition phase.” (No. 4)
What Roles Do PCPs Wish for PTs to Take and For What Purposes in Primary Care Settings?
PCPs with long clinical experience in various primary care settings felt that the role required of PTs in actual primary care settings would differ from that in hospitals; namely, the theme of rehabilitation in integrated community care. This theme was classified into 3 subcategories: (I) causal interaction system, (II) becoming important stakeholders in the community, and (III) continued support to the individual.
Causal interaction system
Actual settings of primary care provide increased opportunities to be involved in the lives of patients and their families from a position of greater visibility. These settings also allow manifestion of the International Classification of Functioning, Disability and Health (ICF) viewpoint, in which various factors related to living as a whole are viewed as interactions. These are likely to be overlooked in hospital settings—which are distinct from normal living—during the limited length of hospitalization. Accordingly, the PCPs expected PTs to be involved not only in approaches to the physical function and personal factors of the patients and community residents they care for, but also in multifaceted approaches to environmental factors, such as proposals to ameliorate the living environment.
“I think the rehabilitation specialist has a good eye to look at the community as a whole, and has adequate knowledge about the functional classification of rehabilitation and the concept of ICF within their ordinary sense of values.” (No. 3)
Become important stakeholders in the community
Actual settings in primary care provide increased opportunities to conduct community health promotions and to suggest disease prevention approaches to the national and local governments. Consistent with this, the PCPs understood the position of PTs with whom they worked in hospital care and home healthcare as able to build close relationships with patients during their daily access to individual patients and families. They expected that PTs would make the best use of their position in the wider community to become important stakeholders in understanding the life of community residents, and serve as mediators to raise awareness of the concept of rehabilitation among individual community residents.
“The physical therapist often has a long association with the patient during the course of providing rehabilitation, and thus establishes a close relationship. (SKIPPED) If a physical therapist keeps close to local life and is involved with patients, care recipients, and the entire community, it will have a very positive effect on care recipients, patients, and the entire community.” (No. 8)
Continued support to the individual
In actual settings of primary care, there are increasing opportunities to undertake personal approaches to prevention of physical dysfunction arising from both degenerative change and the living environment, as part of the ongoing relationship with the patient and family. However, because primary care physicians, who are in relatively short supply, have limited knowledge about rehabilitation outside of medical practice, or sufficient time to utilize such knowledge, they encounter difficulty acting for patients and community residents under a directly patient-oriented concept of rehabilitation. Given that their involvement with individual patients is often ongoing, PCPs may consider preventive rehabilitation for patients with chronic knee pain and interventional rehabilitation for acute low back pain. Palliative rehabilitation may be provided to allow community residents to maintain a relatively good quality of life (QOL). PCPs expect PTs to play a role in working with PCPs to promote the patient’s activities and social participation, and to flexibly respond to environmental factors around the patient.
“We (primary care physicians) think about how we can incorporate the concept of prophylaxis into routine medical practice, so we would like to work with physical therapists in formulating programs for living rehabilitation and preventive measures against further functional deterioration, creating patient leaflets, and disclosing information for community residents.” (No. 3)
Discussion
In this study, we clarified that PCPs understood the role of PTs in hospitals to be “Rehabilitation in the traditional medical model,” and expected the future role of PTs in primary care to be “Rehabilitation in integrated community care.” These findings required that the roles fulfilled by PTs to date within the traditional medical model be adapted to future primary care, and may provide directions for PTs in associating with communities and patients in the aging society.
PCPs understand the major role of PTs to be the provision of rehabilitation in the traditional medical model. This fact is considered to be based on the background fact that many physicians became physicians through 2-year residency training at hospital after graduating from university, 25 and also on the unification and socialization of physicians’ roles in the medical model through experience in treating patients with acute disease. 26 Medicine has long been based on disease models 27 ; the pathologic model of acute disease generally works well for acute diseases in otherwise healthy subjects because such conditions most often involve a single organ system and have a short and well-defined clinical course (eg, trauma, infections, and many others). 28 Our present results showed that PCPs understood the roles of PTs under a mono-causal system, namely a specific and well-defined outcome for the individual, and adapted to a short clinical course for improvement or maintenance. This is similar to the pathologic model of acute disease. This may represent the individual physician’s experience in working with PTs and the process of interactions during hospital training for socialization as physicians while learning about disease models. Hence, physicians may possibly regard PTs as specialist actors within this disease model, and consider PT roles in the model as “normative” through interactions between the physician—who directs the PT to perform rehabilitation—and the PT—who provides feedback on rehabilitation outcomes to the physician.
Primary care in the future must be able to handle multiple factors, not only with regard to biological aspects but also other factors, from a multifaceted viewpoint. 28 The PCPs who were the subjects of this study expected PTs in future primary care to concern themselves not only with individual patients, but also in an ongoing manner with the community as a whole, and in a way which makes the best use of their expertise. This situation is considered to be built upon the viewpoint of medical generalism, 29 which PCPs consider important. Medical generalism, an approach to the delivery of healthcare no matter whether to individuals, families, groups or communities, involves the concepts of “seeing the person as a whole and in the context of their family and wider social environment” and “engaging in effective multi-professional working and co-learning.” Hence, it seems that when looking at not only the disease, but also the patient’s/family’s living and social environment, PCPs considered the presence of PTs as essential for implementing medical generalism, and expected that PTs would exhibit their expertise not only in individual approaches to walking and other physical functions, at which the PT is skilled, but also to view patient/family lives as a whole, in primary care settings.
This study is subject to some limitations. First, there was variation in the relationship between the interviewee and interviewer. It is possible that the interview was unable to derive meaningful content at the first meeting. However, the interviews were made in accordance with a guideline, enabling us to minimize any variation in content. Second, a considerable amount of time has elapsed post data collection, and the role of PTs may have changed in the context of social changes over the past few years. Third, with regard to the role expectations of PTs held by the PCPs and their potential to contribute to future primary care, the answers essentially excluded limitations on medical service systems and authorities. Therefore, the results of this study might not be directly applicable to clinical practices. In addition, given the limited small and purposive sample, caution might be necessary in applying the findings to non-Japanese contexts. On the other hand, while the expertise of physical therapists in the hospital setting is internationally established, it is also true that there is no consensus on the role of physical therapists in the primary care setting. In this regard, it is significant that the role expectations of physical therapists in primary care have been clarified. Particularly considering that the number of professionals in primary care areas such as physical therapists is limited, flexible professional role contributions are required, and professionals need to understand, acquire, and fulfill the roles expected of them by others. We hope that this type of research will also be conducted for other professions. Our next study is expected to investigate how the behaviors of PTs changes after the develop a deeper understanding of the roles expected of them by others.
Conclusion
PCPs, through experience of working with PTs at hospitals, viewed PTs as providers of rehabilitation in the traditional medical model. Meanwhile, PCPs anticipated that PTs would play a role in maintaining and coordinating individuals and environments within integrated community-based care, and become important stakeholders in the community. These findings provide directions for PTs in associating with primary care in the aging society, and may be useful in the development of curricula for PTs in future.
Supplemental Material
sj-xlsx-1-jpc-10.1177_21501319221124316 – Supplemental material for What Role Expectations Do Primary Care Physicians in Japan Hold for Physical Therapists Regarding Primary Care?
Supplemental material, sj-xlsx-1-jpc-10.1177_21501319221124316 for What Role Expectations Do Primary Care Physicians in Japan Hold for Physical Therapists Regarding Primary Care? by Ryohei Goto, Junji Haruta and Sachiko Ozone in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japanese Physical Therapy Association (JPTAH30-A28).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.