
Abstract
Keywords
Physician-driven transformation of health care delivery is a key pillar of the 2010 health care reforms.1,2 The Affordable Care Act seeks to improve health care quality, access, and equity while lowering costs through the effective deployment of primary care. It is critical to strengthen the role of primary care physicians (PCPs), majority of who are employed in group practice settings. Salaried PCPs’ practice behaviors may differ from those of solo physicians/practice owners because the former are not directly affected by clinic-level financial incentives such as pay for performance, and, therefore, may be more concerned about delivering high-quality care. 3 This study examines salaried PCPs’ self-reported ability to provide high-quality care under individual PCP-targeted financial incentives.
Financial Incentives in Primary Care
Financial incentives targeting physicians are widely used 4 with varying effectiveness documented in primary care settings. One study reported improvements in several patient outcomes and a reversal of the achieved improvements on withdrawing the incentive. 5 Other studies report marginal to insignificant impacts of financial incentives on immunization rates,6-8 tobacco cessation,9,10 cancer screening services, 11 and patients’ subjective experience of care quality. 12 A meta-analysis reported a positive effect of financial incentives among both solo physicians and group practices. 13 Many factors may drive the contradictory observations noted above, notably the following: depth of practice behavior change being targeted (single outcome focused incentives vs incentives requiring pervasive changes in practice mind-set), aspect of practice targeted (business profitability focused vs patient welfare focused), practice climate (orientation to innovation and change), 14 clinic’s orientation to patient care (comprehensive vs episodic approach), and a real possibility that physicians’ reported reactions to an incentive may diverge from empirically observable practice behaviors.
The importance of aligning financial incentives with the desired behavior change is well recognized.15,16 However, the empirical association of financial incentives with the global quality of are assessed by the PCPs themselves has not been studied. Our study question is “Do financial incentives targeting care quality/care content affect the ability to provide high-quality care differently compared with incentives targeting productivity increases, after accounting for patient-centered medical home (PCMH)–consistent practice climate?” The conceptual framework driving our study is presented in Figure 1, drawing on elements of health care quality determinants postulated by Hogg et al. 17
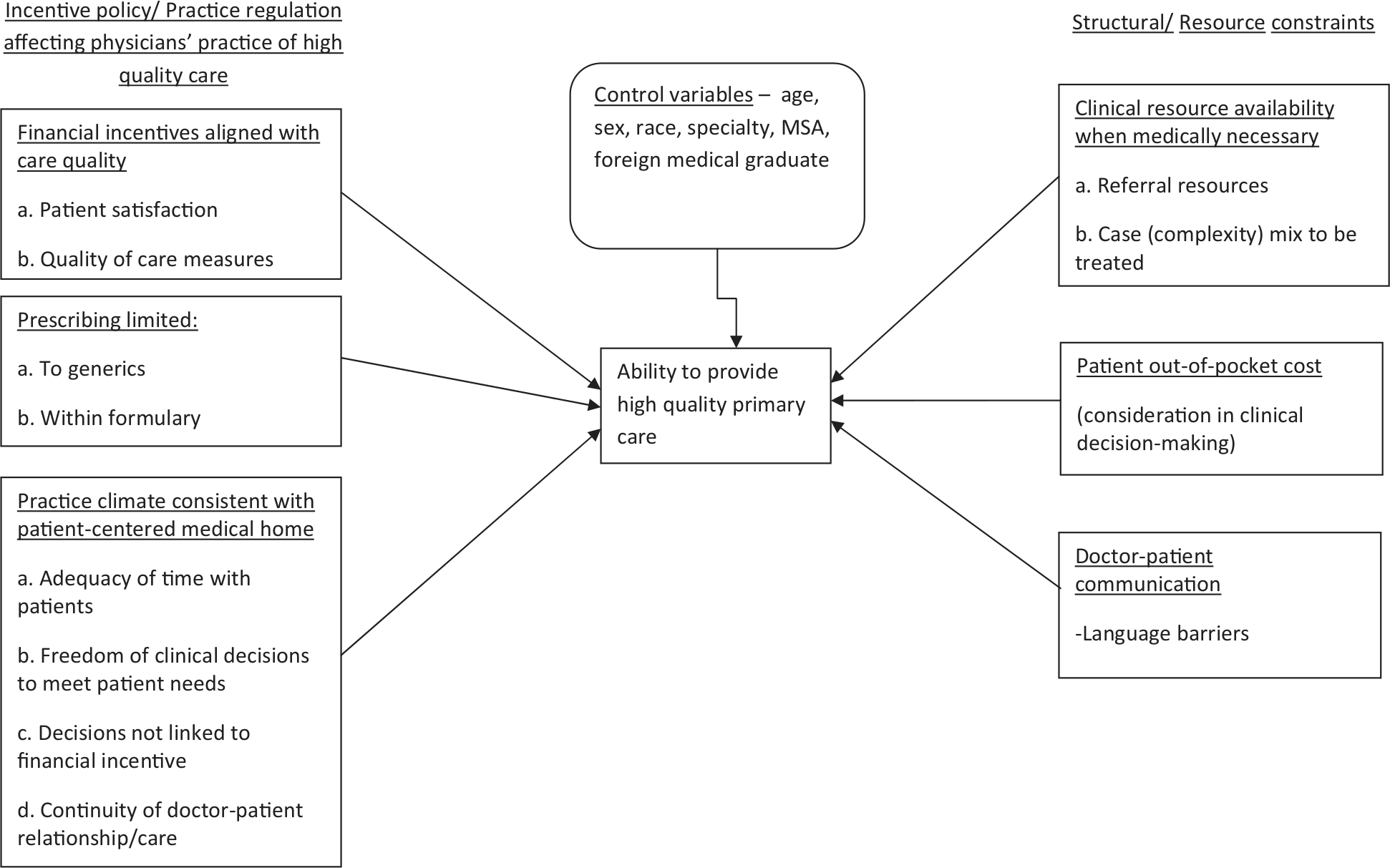
Schematic model tested in the study: Impact of organizational policies targeting practice behavior and practice climate on primary care physicians’ ability to provide quality care.
Methods
We conducted a cross-sectional analysis of secondary data on nonfederal, practicing PCPs from the 2004-2005 Community Tracking Study Physician Survey (members of the American Medical Association and American Osteopathy Association in 60 randomly selected US communities). 18 Of total PCPs 1733 were study eligible, being salaried, reporting family medicine, internal medicine, or pediatrics as their specialty, and not a solo practice owner.
Dependent Variable: Ability to Provide Quality Care
Because most measured health care outcomes are very specific, they are inadequate proxies to measure changes in practice mind-set, the real target of most change initiatives. Management’s focus on specific, incentive-linked outcomes may cause inadvertent neglect of unmonitored diagnoses or care items resulting in poorer global care quality, despite an ostensible improvement in the measured indicators targeted by the incentive. To address this issue, this study examines global care quality judged by PCPs as the dependent variable of interest, measured as ability to provide high-quality care on a 5-point scale. Responses were recoded into 3 categories (“strongly disagree and disagree,” “neutral to agree,” and “strongly agree”), to separate clearly negative responses (disagree and strongly disagree) from the unequivocally positive response (strongly agree), with a middle category, neutral/agree representing mediocre (but not poor) quality of care. Another pragmatic reason for merging response groups was the small number of neutral responses (n = 40).
Financial Incentives and Practice Climate Context
Financial incentives were defined based on 5 survey items on PCP salary compensation policies. The survey measured each financial incentive by its importance in determining the PCP’s total compensation (1 = not at all important to 5 = very important). The performance outcomes linked to financial incentives were revenue or number of patients per day, overall practice financial performance, patient satisfaction, quality of care, and comparative practice profiling.
Because of the potential importance of PCMH climate in primary care, and its possible role in moderating the quality impact of financial incentives, this study controlled for PCMH features of the practice. We identified 4 Community Tracking Study survey items allied with current conceptualizations of PCMH. 19 The items were (a) possible to maintain a long-term relationship with patients such as to promote high-quality care, (b) freedom to make clinical decisions in the best interest of patients without jeopardizing personal income, (c) spending enough time with patients during typical office visits, and (d) having clinical freedom to make decisions to meet patients’ needs (1 = strongly disagree to 5 = strongly agree). These items are consistent with a widely endorsed definition of PCMH, “a model of care that strengthens the clinician-patient relationship by replacing episodic care with coordinated care and a long-term healing relationship.” 20
Decisions regarding fostering a PCMH-consistent practice climate and regarding financial incentives reflect the clinic management’s policy. We conducted an exploratory factor analysis of the above nine survey items on PCMH and financial incentives to evaluate the empirical validity of these theoretical constructs. Using promax rotation, we extracted 3 factors (with eigenvalue >1) that explained 61.5% of the total variance in item responses (Table 1). Two were financial incentive constructs and were named (a) financial incentives aligned with care quality/content (patient satisfaction scores, quality of care indicators, and physician practice profiling) and (b) financial incentives aligned with productivity/profitability (physician productivity and practice financial performance). The third factor was PCMH-consistent practice climate that showed high loadings on all 4 PCMH items. Factor loadings showed a simple structure suggesting robust empirical validity of the constructs. A composite score for each factor was calculated by adding the respective item scores.
Primary Care Practice Policies on Financial Incentives and Fostering a Patient-Centered Medical Home Practice Climate: Exploratory Factor Analysis Results.
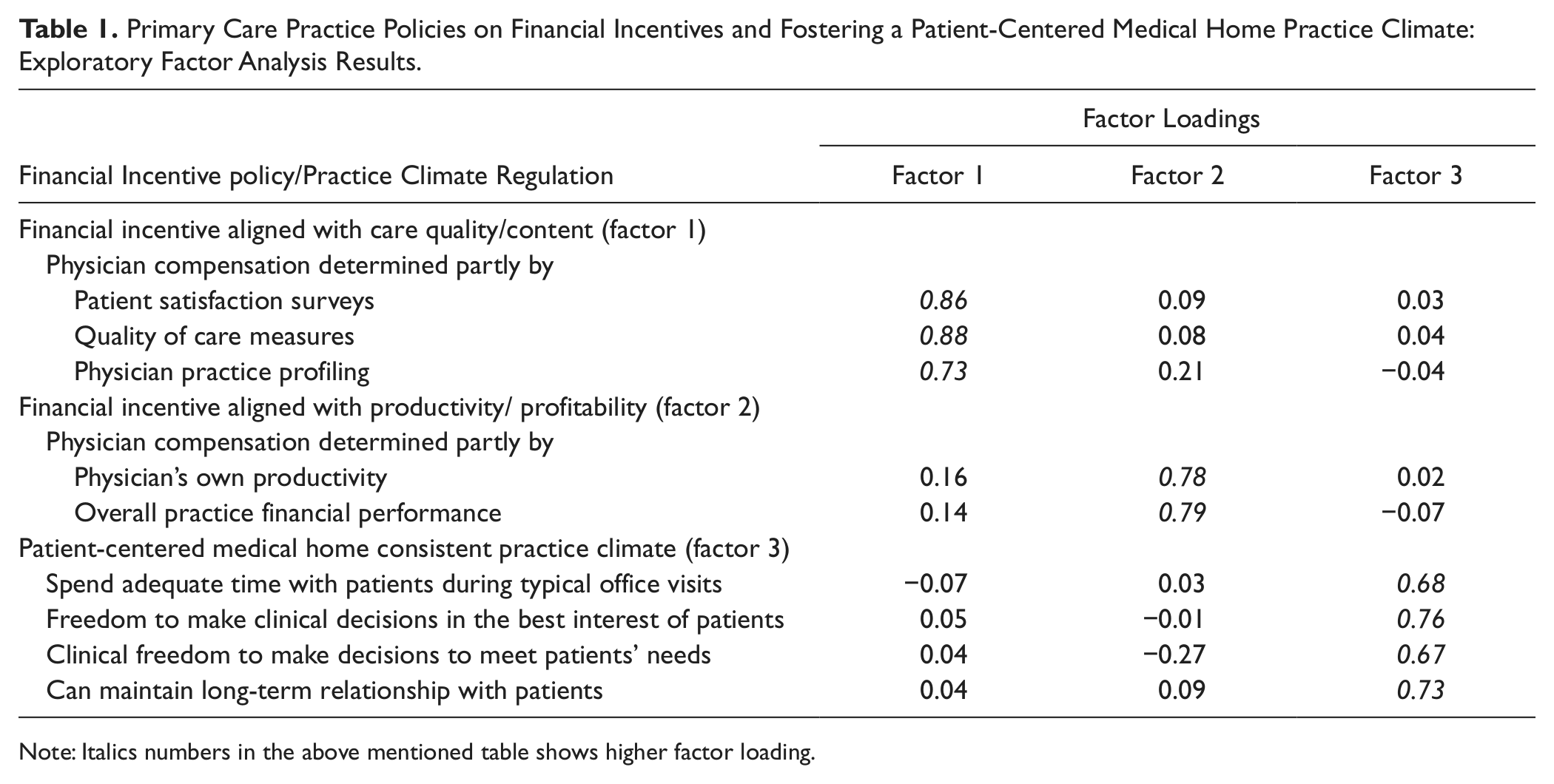
Note: Italics numbers in the above mentioned table shows higher factor loading.
Other Control Variables
Structural and resource constraints faced by PCPs in providing what they perceive as appropriate care (eg, inability to obtain referral services) also affect the quality of care. The factors adjusted for are as follows: availability of supportive/referral clinical resources, measured by 4 items (dichotomous responses, yes/no, added into a single summary score) regarding ability to obtain specialist referrals, nonemergency hospital admissions, high-quality diagnostic imaging services, and high-quality mental health services; having to consider patient’s out-of-pocket financial burden when selecting tests and type of care (inpatient vs outpatient, 1 = never to 5 = always); and requirement to comply with drug prescribing guidelines (generic drug use, 1 = never to 5 = always) and formulary use (1 = less than 20% to 5 = more than 80%). Finally, we accounted for current clinical complexity of patients expected to be treated without specialist referral compared with before (1 = much lesser to 5 = much greater than before). We conceptualize structural/resource constraints as providing the context within which financial incentives facilitates or impedes high-quality primary care. Physician demographic and practice characteristics (age, gender, race, metropolitan statistical area, specialty, practice type, foreign MD degree, and percentage of patients speaking a different language) were also controlled for.
Statistical Analyses
Univariate statistics are presented on the sample distribution on demographic and study variables of interest. Generalized multinomial logit regression that does not assume proportional odds between levels of the dependent variable was used to explore the study question. Higher levels of the dependent variable (strongly agree, and neutral/agree) are compared with the referent level (strongly disagree/disagree).
Results
Sample Characteristics
Table 2 presents the PCP sample characteristics. Mean PCPs’ age was 45 years, 60% were male, 40% were family/general practitioners, and 83% were practicing in large metropolitan cities. In all, 21.0% of the sample PCPs strongly agreed with the statement, “I am able to provide high-quality care to all of my patients,” 38.5% disagreed or strongly disagreed, and 40.5% were neutral/agreed with the statement.
Distribution of the Physician Sample by Demographic and Study Variables of Interest.
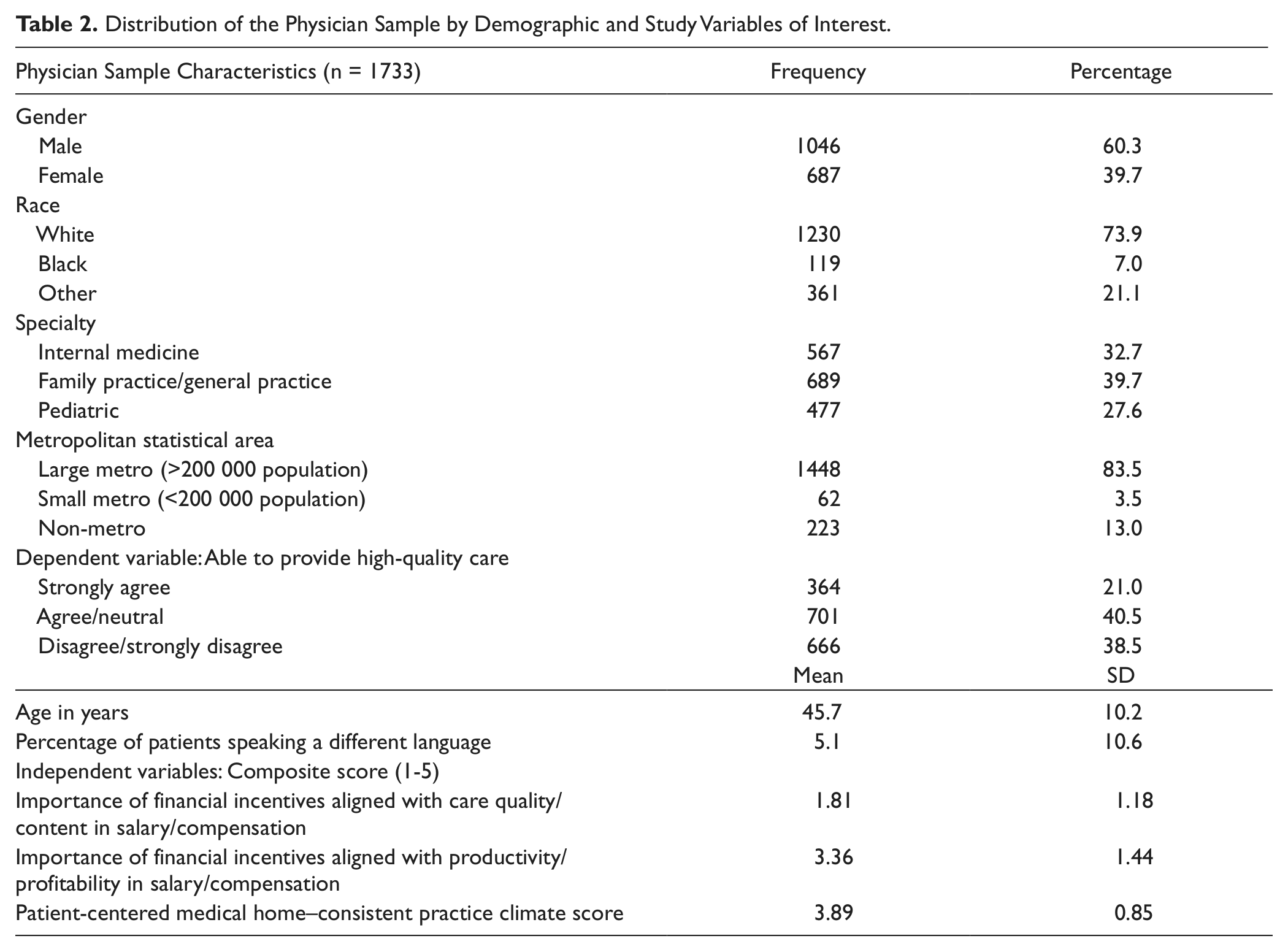
Financial incentives of sample PCPs were heavily weighted toward productivity with the mean score of 3.36 on the composite score (1-5) rather than care quality/content (1.81). The two types of financial incentives were positively correlated (r = 0.32) Sample PCPs perceived their practice setting to be highly oriented to PCMH (mean = 3.89 from the composite variable).
Bivariate associations between financial incentives and PCPs’ ability to provide quality care are presented in Table 3. Financial incentive aligned with care quality/content was significantly associated with self-reported ability to provide quality primary care (unadjusted odds ratio [OR] = 1.19; P < .05 for strongly agree), and productivity-/profitability-linked incentive is not significantly associated.
Unadjusted and Adjusted Odds Ratios of Primary Care Physicians’ Ability to Provide High-Quality Care Under Financial Incentives (n = 1733).
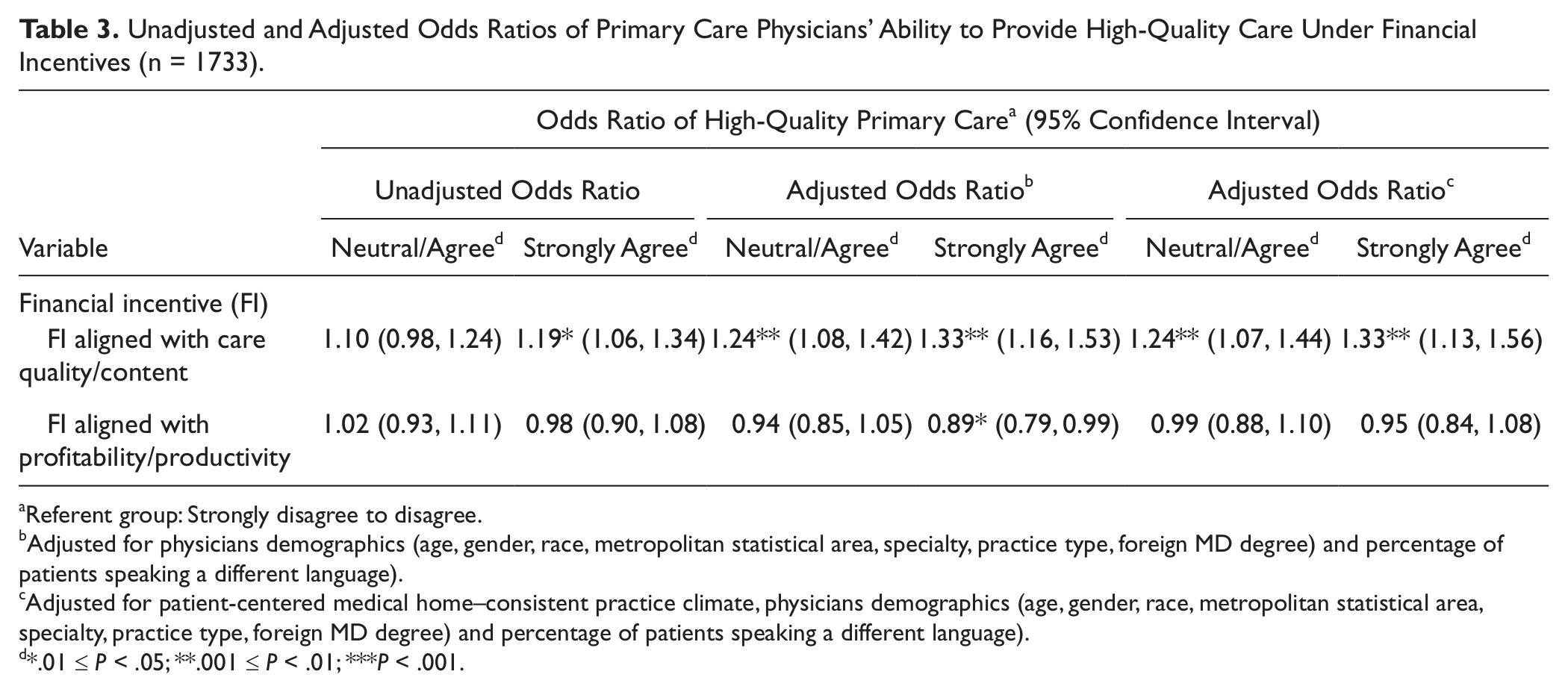
Referent group: Strongly disagree to disagree.
Adjusted for physicians demographics (age, gender, race, metropolitan statistical area, specialty, practice type, foreign MD degree) and percentage of patients speaking a different language).
Adjusted for patient-centered medical home–consistent practice climate, physicians demographics (age, gender, race, metropolitan statistical area, specialty, practice type, foreign MD degree) and percentage of patients speaking a different language).
*.01 ≤ P < .05; **.001 ≤ P < .01; ***P < .001.
Generalized Multinomial Logit Regression
Table 3 also presents adjusted associations using 2 multiple regression models. The first model adjusted for PCP demographic variables and practice characteristics noted above, structural constraints, and the proportion of patients speaking a different language. In this model, financial incentive aligned with care quality is positively associated with PCPs’ self-reported ability to provide high-quality care, and financial incentive aligned with productivity/practice profitability shows a negative association with the ability to provide high-quality care (OR = 0.89, P < .03 for strongly agree vs strongly disagree/disagree). The second model additionally adjusted for the practice PCMH score. In this model, quality-linked financial incentive remains positively associated with the ability to provide high-quality care at identical ORs as before (OR = 1.24, P <.01 for agree/neutral; OR = 1.33, P < .01 for strongly agree), but productivity-linked financial incentive is no longer significantly associated with quality care.
Discussion
This study explored how financial incentives affect PCPs’ ability to provide high-quality care. Financial incentives linked to care quality/content were associated with greater confidence in providing quality care, after adjusting for PCMH practice climate and other structural constraints. This finding is generally consistent with past studies, except for a few apparent contradictions. This contradictions are readily resolved if a careful distinction is drawn between financial incentives triggered by achieving certain minimum service/coverage thresholds, and incentives for continuous quality improvement. The former were less likely to produce the target outcomes14,21-24 whereas the latter were effective in achieving and maintaining the target improvements.12,25 The latter studies’ outcome variables are more consistent with our study.
Hospital studies of payer-driven pay-for-performance report improved care quality associated with the incentive. 26 Other studies noted that such quality improvement was mediated by organizational policies supporting care coordination, system change, and innovation. 27 Our study validates their findings in primary care settings, showing that both PCMH-consistent practice climate and quality-linked financial incentives were positively associated with PCPs’ ability to provide high-quality care. An important finding is that beyond the positive effect of a PCMH environment, quality-linked financial incentives increase salaried PCPs’ ability to provide quality care.
Another important finding is that productivity-linked financial incentive was negatively associated with the ability to provide quality care, but it lost significance once PCMH practice climate was included in the model, suggesting that a PCMH practice climate mitigates the negative effect. This finding is important because physician productivity is critical for financial viability of group practices. Productivity-linked incentives remain an inevitable feature of practice financial management. Our study suggests that reconfiguring practices to a PCMH model can mitigate the adverse effects of such incentives. A previous study reported a negative effect of productivity-linked incentives on physicians’ self-reported ability to practice good-quality medicine (all specialties, mean sample age 52 years), and noted mitigation of negative affect by the duration of physician exposure to HMO/cost-conscious practice during medical training. 28 Our sample mean age of 45.5 years may reflect greater exposure to HMOs during medical training relative to the earlier study.
The study has some limitations. It did not account for HMO exposure of the practice, an important determinant of physician-perceived quality of care. However, the constraining effect of HMOs is likely captured in our measures of structural constraints. Another potential limitation is common method variance bias due to sourcing data on the dependent variable (subjective judgment about high-quality care) and independent variables from the same source, causing inflated estimates of associations. 29 However, such bias is reported to be insignificant.29,30 To address our study question, physicians remain the most appropriate source for most variables—global quality of care, compensation package, PCMH climate, and structural constraints in practicing medicine. Finally, being limited to salaried PCPs, our study findings may not generalize to solo practice owners and to specialists. Notwithstanding the limitations, our findings suggest that appropriately designed financial incentives, along with PCMH implementation can improve the quality of primary care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.