
Abstract
Background:
The post-Soviet country of Georgia has recently decriminalized recreational cannabis use, yet implementation of screening for cannabis use in clinical practice remains unclear. This study assesses relevant knowledge, attitudes, and practices of primary health care physicians (PCPs) regarding recreational cannabis use in the country of Georgia.
Methods:
We conducted a mixed-method study, starting with a cross-sectional survey among PCPs practicing in Georgia. Quantitative data were received from 246 family physicians, using a structured anonymous questionnaire addressing legal awareness, health risk perception, and screening practices. Supplementary qualitative interviews were conducted among 10 PCPs exploring barriers to effective cannabis-related counseling and documentation.
Results:
Almost all (96.6%) respondents were female, and 55.7% were aged > 51 years. Only 35.6% of physicians reported being familiar with cannabis legislation. The majority associated cannabis use with mental health risks (97%) and increased accident risk (92.4%). Fewer than half acknowledged its legitimate medical applications (eg, chronic pain management). Screening rates were low – only 26.6% documented cannabis use in patient records, and 88.1% had never applied structured criteria to diagnose cannabis use disorders. The qualitative exploration found that time constraints, stigma, and lack of relevant training were the frequently cited barriers. Physicians expressed concern that insufficient knowledge undermines their ability to provide evidence-based counseling, potentially increasing public health risks.
Conclusion:
Primary care physicians’ preparedness to screen and counsel patients on cannabis use is insufficient in the country of Georgia. Targeted continuing medical education and system-level interventions are essential to bridge this gap and promote safe, informed care.
Introduction
Cannabis is one of the substances most commonly used for recreational purposes worldwide. 1 Cannabis use can cause adverse effects such as psychosis, anxiety, depression, respiratory distress, cannabinoid hyperemesis syndrome, and impaired cognitive performance. 2 Cannabis use is associated with other adverse mental health outcomes, like poor well-being and psychosocial functioning.3,4 Cannabis-linked impaired cognitive performance may be associated with increased risk of car accidents and poor educational attainment. Lung injury, increased risk of coronary artery disease, seizures, and recurrent strokes at young age are some of the other cannabis-use associated risks.5-8 Early and regular use of cannabis is correlated with elevated risks of suicidality and cannabis dependence.9-11
Besides the described health risks, cannabis has qualities that can benefit human health. For example, cannabis has been used in palliative care and in chronic condition symptom management (eg, chronic pain, cancer-related nausea, appetite loss). Medical cannabis has also been used to treat glaucoma, pediatric epilepsy, spasticity, gastrointestinal, and other conditions, as well as to support healthy aging and health maintenance. Research on long-term safety and efficacy is still ongoing.2,12-14
Despite the gradual liberalization of policies in a number of countries, significant knowledge gaps remain to guide evidence-based clinical care addressing cannabis use. Many physicians are hesitant to ask their patients about the topic or advise them about possible health effects. The lack of questioning is concerning for both doctors and patients. 15
Since 2018, recreational use of cannabis has been decriminalized in Georgia. However, retail or use in public spaces remained illegal. 16 Possession is also strictly regulated. The sources of cannabis for users were home-growing, peer sharing, and the illegal market. 17 The policy change didn’t result in a significant increase in lifetime or annual prevalence of use among Georgian emerging adults. (Nadareishvili, Rao and Otiashvili, 2025) Annual prevalence of cannabis use in 2022 was 18.1%, a statistically insignificant increase compared to 17.3% before legalization (in 2015). In 2022, past year prevalence of cannabis use in the 18 to 64 age population in Georgia was 20.9%. 18 The same year, 19% of people agreed that cannabis use should be prosecuted by imprisonment. However, 47% agreed that cannabis users should be fined financially. 18
Benefits of linking substance use services with primary care have been identified. 19 Introduction of Screening, Brief Intervention and Referral to Treatment (SBIRT) model was a significant development in addressing substance use behavior and mental health conditions in various settings, including in primary care.19-21 SBIRT is a comprehensive screening tool used to identify individuals who use substances at risky levels and accordingly suggests appropriate interventions. While the evidence is stronger for alcohol users, there is growing evidence in the literature indicating SBIRT’s effectiveness in reducing risky drug use. 20 While physicians often find SBIRT to be helpful, results of the studies on its modifying effect on cannabis use behaviors vary. The challenge of achieving behavioral change might be grounded in inconsistent provision of SBIRT for cannabis use in various contexts. 22 A recent study from the US reported that time limitations, confidentiality issues, resource constraints, training needs, and ambivalence to cannabis use among patients and providers represented some of the main barriers to implementation of cannabis focused SBIRT in primary care. 23
A part of the wider highly fragmented and privatized health system, primary care in Georgia has been characterized by underutilization and systemic weaknesses, including deep differences in resources allocation and infrastructure among the clinical facilities owned and operated by the numerous for-profit organizations.24-26 Primary care workforce has been characterized as aging and insufficiently structured, with only 1 nurse per 3 physicians practicing in primary care settings.27,28 Deregulation of licensure (ie, licenses issued for indefinite term), and insufficient postgraduate training health system (including Continuing Medical Education (CME) and Continuing Professional Development (CPD)) have been additional challenges.27,29 With a high prevalence of an aging workforce and poor infrastructure, rural areas have been particularly vulnerable.27,30 However, some initiatives, such as introducing telemedicine services in rural areas, contribute to the improvement of service delivery in primary care in rural areas. 31 A general primary care reform in Georgia was initiated in 2025.
Recent initiatives move Georgia toward better substance use management in primary care. This includes the adoption of several guidelines and protocols, including the protocol on substance use screening and management using SBIRT, by the government, development of locally adapted educational resources, and introduction of CME opportunities for primary care physicians.32,33 A guideline on Cannabis Use Disorder (CUD) management in both inpatient and outpatient settings was published in 2023. 34 Despite the progress in PCP training, little is known about the current knowledge, attitudes, and practices in Georgia’s primary care settings in relation to cannabis use counseling and intervention. The aim of this study was to assess the current cannabis-related counseling practices and physicians’ training needs in primary care in Georgia.
Methods
This was a mixed-method study, utilizing a descriptive cross-sectional survey and a qualitative exploration of cannabis related counseling practices.
Quantitative Study
We conducted a cross-sectional online survey among PCPs (family doctors) working in 6 cities (Tbilisi, Batumi, Rustavi, Kutaisi, Sachkhere, Telavi) of Georgia. We used a convenience sample, as a database of practicing primary care physicians was not available. We distributed the online survey link via available email address lists (eg, through professional associations and university clinical training facilities) and professional networks. The data was also collected through in-person visits to 7 primary care clinics in the capital city. We collected the survey data between January and March 2024.
A total of 246 respondents provided at least 1 non-missing response; however, 9 cases had high missingness of data, and 237 response data were included in the analytic dataset (overall N = 237). Because item nonresponse varied across questionnaire sections, valid N differs by item.
The questionnaire included 30 items and was programed in SurveyMonkey, an online survey platform. The first block of questions covered demographics (sex, age), medical school graduation year, workplace type (outpatient clinic, general hospital, specialized hospital), working location (the capital city of Tbilisi, other bigger cities, smaller towns and villages), clinical specialty (based on license), and knowledge of foreign languages sufficient to analyze evidence-based medical literature. The second block of questions assessed general knowledge on cannabis, the relevant legislation in Georgia, and the health-risks related to cannabis use. Questions were organized in matrix (describing specific health related statements) using a Likert scale. The next set of questions was organized around the history-taking process and cannabis use-related counseling practices. Respondents were asked about components of history taking, any screening tools used, counseling practices, using a Likert scale and checkboxes to mark several options simultaneously. We then asked about personal attitude (support, against, neutral) to cannabis decriminalization, full legalization, and medical cannabis use. The final set of questions asked about relevant Continuing Medical Education/Continuing Professional Development experience. The questionnaire is available as Supplemental Material.
Descriptive statistics (frequencies and percentages) were computed for all variables. We conducted inferential analyses to assess how physicians’ time in practice and past training on cannabis use influenced physicians’ counseling practice and knowledge. First, continuous and ordinal variables were summarized with means, standard deviations, medians, and frequencies. Composite knowledge (K-mean) and counseling (H-mean) scores were computed as row-wise means. Nonparametric tests—Mann–Whitney U for 2-level factors and Kruskal–Wallis for multi-level factors—were used to compare distributions. Spearman correlations evaluated associations among screening items. Following the significant Kruskal–Wallis result for cannabis history documenting by age group (P = .006), we performed post-hoc pairwise comparisons using Dunn’s test with Bonferroni correction. Chi-square tests assessed whether categorical groupings (eg, residence) were related to dichotomized screening outcomes (eg, frequent vs infrequent documenting). All analyses were conducted using Python (version 3.11). For the statistical analysis, we used P < .05 as a cut-off criterium for statistical significance, and for post-hoc analysis, where applicable.
Qualitative Study
To gain additional insights into participants’ perspectives and experiences, we conducted semi-structured interviews with a subset of survey respondents (n = 10). The participants were licensed family physicians and practiced in the same specialty (which is the core specialty in Georgian primary care system). We used a purposive sampling approach, aiming to cover the country geographically and have respondents employed both at large and small-scale medical facilities, both in the big cities and smaller towns. We recruited the respondents based on the database formed during the quantitative survey.
The interview guide included open-ended questions on the general substance use environment as perceived by the family physicians, opinions on recreational cannabis use, encounters with patients using cannabis, and perceptions of challenges posed by cannabis use to the populations. We explored screening, counseling, and intervention practices. We also asked about any potential barriers to screen for cannabis use, provide necessary care, and the physician’s wishes and needs regarding continuing education and development. The interviews were held remotely, using Zoom, and took 35 to 45 min to complete. All but 1 interview were held by a single interviewer; 1 interview had 2 researchers interviewing.
We transcribed the audio recordings verbatim in Georgian. Two researchers independently coded the transcribed data, compared and discussed the codes before analysis. Although the qualitative data did not yield extensive new themes, we conducted a brief content analysis to identify recurring patterns that could help interpret or expand upon the quantitative findings. Two researchers independently reviewed the transcripts and drafted summary memos. A few illustrative quotes are presented in the Results section to highlight points of convergence or divergence with the survey data.
Ethical Statement
Following the review of the study aims, design, and potential outcomes, ethical approval for this study was obtained from the David Tvildiani Medical University Ethics Committee (#2/23, January 9, 2023). All participants received written and oral information regarding the study objectives, background, and how the data would be used and treated. The quantitative component participants expressed their own consent to participate by continuing to the first page of the survey. The interview participants gave their own consent verbally, following the introduction to the study and prior to the interview itself. We took measures to ensure confidentiality and anonymity throughout the research process.
Results
Quantitative Survey Results
Sample Descriptives
We received 237 valid responses to the survey (96.6%, n = 228, of the respondents were female). In terms of age distribution, 28.3% were over 60 years old, 27.4% were between 51 and 60, 35.9% were aged 41 to 50 years, and 8.4% were 40 years or less. The demographics of our sample reflect the overall demographics of the primary care workforce in Georgia. Regarding workplace distribution, 87.8% (n = 208) were employed as family doctors in outpatient clinics, 9.3% (n = 22) worked in multiprofile hospitals, and 3% (n = 7) in specialized clinics. The majority of respondents (80.2%, n = 190) were from the capital city, 13.1% (n = 31) were based in small towns or villages, and 6.8% (n = 16) lived in other bigger cities. The detailed sample descriptive statistics are reported in Table 1.
Descriptive Statistics of the Surveyed Sample.

Knowledge on Cannabis and Relevant Legislation
Regarding the information about legislative changes, 64.3% have indicated that, they are not aware or have only fragmented information about the cannabis use liberalization which took place in Georgia in 2018.
Regarding terminology, 67.9% of respondents believe that cannabis, marijuana, and hashish are the same, 20.7% said these are different things, while 11.4% stated that they do not know the exact definitions.
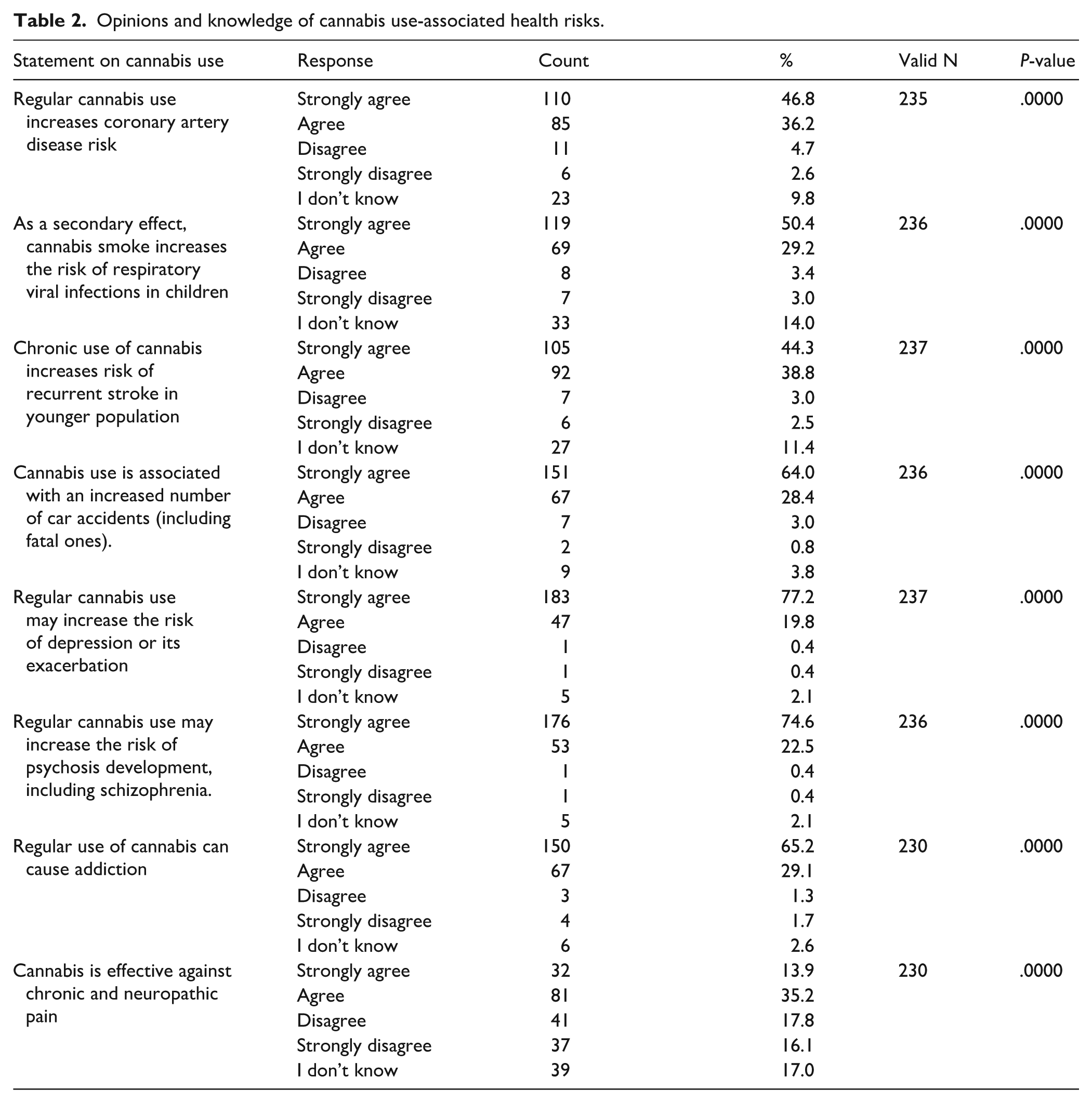
Most family doctors acknowledge the risks associated with regular cannabis use. Almost all (97%) agreed that there is sufficient medical evidence indicating that regular use may increase the risk of depression or exacerbate existing depression. Similarly, 97.1% (n = 229) believed that cannabis use raises the risk of psychosis, including schizophrenia. The knowledge that cannabis use is linked to a higher incidence of car accidents, including fatal ones, was also very common (92.4%, n = 218, agreed fully or almost). The respondents agreed that cannabis use can result in addiction (65.2%, n = 150, fully agreed, while 29.1%, n = 67, mostly agreed with this statement). Fewer respondents (49.1%, n = 113) thought cannabis could be useful for chronic pain management. Response categories in all the items deviated significantly from uniformity (unadjusted per-item p-values < .001). We again observed significant departures from uniformity across all items when categorizing the responses in 3 categories (Agree, Disagree, Don’t know). The data on opinions and knowledge related to health risks are reported in Table 2.
Opinions and knowledge of cannabis use-associated health risks.
Dedicated CME courses on cannabis use and its health implications were not available in the national database of government-accredited CME courses. Over half (54.1%) of our respondents reported that they completed at least 3 CME courses in the past 5 years. However, only a few (6.2%) respondents reported taking CME on cannabis use and its health implications in the past 5 years, with 92% reporting not completing a relevant CME in the specified period. Furthermore, 77.7% said they had never received any CME training in addiction medicine, while 14.5% stated that addiction-related topics were covered in other CME courses.
History Taking and Counseling
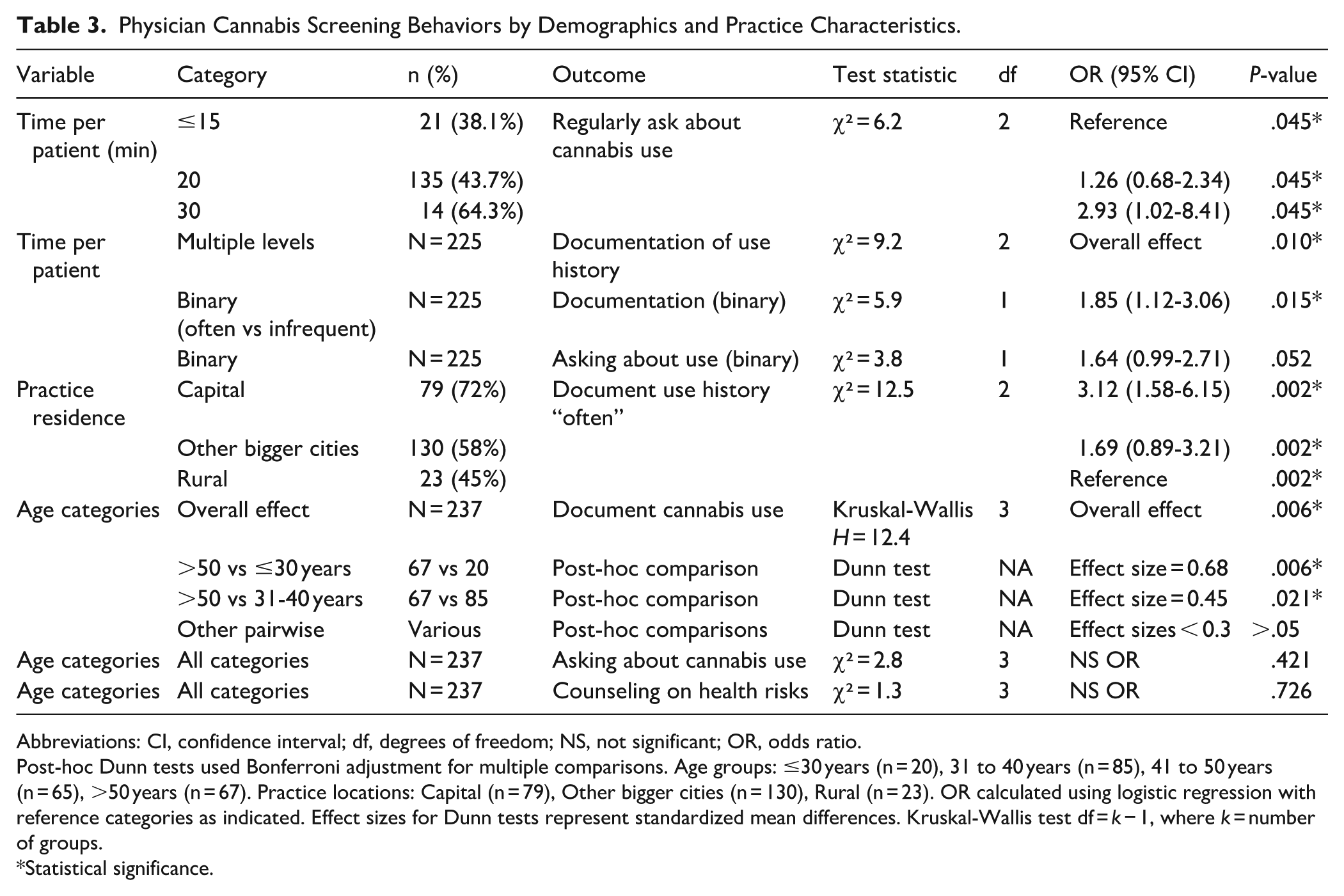
As reported by 42% (n = 95) of the respondents, people rarely disclose cannabis use on their own during medical history taking. A further 18.6% (n = 42) said it never happens. Of those who had 15 min or less allocated for each patient, 38.1% said they asked about cannabis use always or often. This increased to 43.7% for those who had 20 min, and 64.3% for those who had 30 min per patient. While almost half of the respondents said they ask about cannabis use, only 26.6% (n = 60) said they document substance use in medical records, and 36.9% (n = 83) reported that they never note cannabis use in patients’ records.
When asked about questioning patients regarding cannabis use, 44.7% (n = 101) said they do always or often, while 33.6% said they rarely or never ask about cannabis use. To compare, 86.7% (n = 196) of the respondents said they regularly asked about tobacco use, while 85.3% (n = 193) of the respondents reported that they always or often inquired about alcohol use. A chi-square test revealed a significant association between practice residence (Capital, Other bigger cities, Rural) and documentation of cannabis-use history (χ² = 12.5, P = .002). Physicians in the capital documented use of history “often” at a rate of 72%, compared with 58% for the other bigger cities and 45% for rural practitioners. This suggests that urban PCPs are more likely to record patients’ cannabis-use history in their notes compared to their suburban or rural counterparts.
Physicians with longer time allocated per patient in practice reported significantly different distributions of inquiring about cannabis use frequency (P = .045) and documenting use history (P = .010). The chi-square test on the binary classification of documentation (often vs infrequent) confirmed the finding (P = .015), though the difference for cannabis use history taking was marginally insignificant (P = .052).
Documenting cannabis use was significantly different across age categories (P = .006). Dunn’s test revealed that respondents aged > 50 years documented cannabis history significantly more often compared to those ≤30 years (P = .006) and to those 31 to 40 years (P = .0207). No other pairwise comparisons reached significance after adjustment. No significant age-related differences were found for asking about cannabis use (P = .421) or counseling on health risks (P = .726). Comparing the counseling practices by the history of having formal continuing medical education background on cannabis use was not possible due to the low number of respondents who reported such experience.
When documenting cannabis use, family doctors commonly noted frequency (22.4%) and duration of use (21.1%), while only 5.1% recorded the amount consumed per occasion. Additionally, 41.4% said they don’t document cannabis use, and 6.3% said they had never encountered a person who used cannabis in their practice. Most family doctors (88.1%) said they had never used Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 criteria to diagnose or refer patients with cannabis-induced disorders. Only 4% said they regularly use the DSM-5 criteria. Having completed a cannabis use relevant CME didn’t differ by the DSM-5 use categories (P = .919; Table 3).
Physician Cannabis Screening Behaviors by Demographics and Practice Characteristics.
Abbreviations: CI, confidence interval; df, degrees of freedom; NS, not significant; OR, odds ratio.
Post-hoc Dunn tests used Bonferroni adjustment for multiple comparisons. Age groups: ≤30 years (n = 20), 31 to 40 years (n = 85), 41 to 50 years (n = 65), >50 years (n = 67). Practice locations: Capital (n = 79), Other bigger cities (n = 130), Rural (n = 23). OR calculated using logistic regression with reference categories as indicated. Effect sizes for Dunn tests represent standardized mean differences. Kruskal-Wallis test df = k − 1, where k = number of groups.
Statistical significance.
Qualitative Exploration Results
Limited Knowledge and Awareness
The complementary qualitative exploration revealed that the interviewed physicians perceived that cannabis use became highly prevalent, particularly in the last few years, including among young adults and teenagers. One physician stated: “Youth commonly use cannabis, even the school children. I would say most of the people who use cannabis are under 50.” Another physician said: “So many people use cannabis, it is everywhere. It is a huge problem for our people.” However, the qualitative exploration respondents were poorly informed about cannabis effects on human health, the legal status of cannabis use, or the screening and counseling practices for cannabis or other substance use. Respondents expressed concern over cannabis use related health risks, highlighting symptoms such as sleep disturbances, gastrointestinal issues, and anxiety.
Stigma and Communication Challenges
While younger patients were generally more open about their cannabis use, stigma led many, especially older patients, to avoid discussing it. Moreover, doctors themselves reported difficulty in broaching the subject, particularly with older or more seriously ill patients. They found it challenging to ask about cannabis use directly, and the lack of screening tools made medical history-taking more difficult and chaotic. Some physicians use tobacco related questions to open the discussion of substance use with the patients and then transition to the conversation about cannabis. “When I ask about tobacco use, it is easy to ask and afterward, they may themselves start to talk about cannabis use. I choose whom to ask this question to, in the younger population, it is easier to start a conversation about cannabis use. However, for example in older patients or persons who are highly ranked at their work, it is very hard to ask any questions about this,” reported one respondent. During the interview, family doctors also noted that substance use is usually identified during diagnostic investigations for various health conditions, most commonly neurologic ones. “Patients often come with neurological complaints, and we sometimes suspect cannabis use. It can be later confirmed by medical history and further diagnostic investigations.” said one of the respondents. Sometimes, patient complaints are the results of health complications and secondary effects of cannabis use, and cannabis use is identified while diagnosing the reasons for such health conditions, rather than through preventive screening.
Gaps in Training and Resources
Respondents noted a gap in education and training for family doctors regarding the health effects of cannabis and supported an idea of enhanced training, creation of regional specialized care facilities, and application of screening tools to better identify substance use during consultations. All respondents talked about the need for education and establishing screening resources: “Even though we are in the era of access to information, for example, we can easily read about health impact, we still lack evidence-based knowledge about the risks. I think it is a matter of stigma and insufficient education,” said a physician.
Urge for Nationally Adapted Screening Tools and Structured Referral Pathways
The respondents were unable to discuss the topic of SBIRT application in their clinical practice, and were not aware of the standardized and widely accepted screening and diagnostic instruments. Unaware of the existence of Georgian versions of such inventories as ASSIST, the respondents expressed a wish to have access to screening inventories and questionnaires to help identify substance use among patients. They believe that such inventories would make it easier to address the issue during consultations, including screening as a routine practice, in a formal manner. This could be helpful to avoid awkward situations and potential negative reactions from the patients. One of the doctors also mentioned the challenges of referring patients for treatment: “Yes of course it will be helpful to have screening tools, but again, we, family physicians are primary caregivers, primary assessors of patients. After the primary assessment, if we identified a problem of substance use, we should be able to refer patients to specialists like psychiatrists and addiction specialists.”
Discussion
Our findings suggest that the surveyed PCPs in Georgia were unprepared, both in terms of knowledge about cannabis and the application of that knowledge to screen and counsel patients on cannabis use. This might be particularly important in light of the recreational cannabis use limited liberalization in the country, of which most of our respondents considered themselves to be insufficiently informed. At the same time, the majority regarded recreational cannabis consumption as associated with severe health risks, yet fewer than half recognized its approved role in chronic pain management (which, similarly to other medical applications of cannabis, has not been studied or reported in Georgia). The self-reported prevalence of those who asked patients about cannabis use was about half compared to tobacco or alcohol. Together, these findings suggest that, despite widespread concern about cannabis-related harms, physicians did not prioritize the topic during the patient visits, lack the legal and clinical knowledge necessary to integrate recreational cannabis use screening and counseling appropriately into patient care, which may lead to failure to use it in case of indication. With no local medical research on cannabis and its health effects, and in the context of limited CME/CPD and life-long-learning practice in Georgian health workforce, further academic, educational, and technical work is required to inform screening and counseling practice for cannabis use.
International body of knowledge on counseling practices in primary care and attitudes to recreational cannabis use among PCPs is limited. Studies on medical cannabis reported that relevant clinical training is still a major challenge in countries such as Canada and the US, where states and territories have largely legalized medical and recreational cannabis use.35,36 An international survey of healthcare professionals found high concern about cannabis-based therapies, yet a strong demand for more robust clinical trial evidence before confident recommendation. These conflicting beliefs – viewing cannabis as both dangerous and potentially therapeutic – highlight the need for balanced, evidence-based curricula that cover both risks and indications. 37 A recent implementation feasibility study from the US suggested that challenges in SBIRT implementation are common, perhaps particularly in rural communities. However, different approaches and tools, including digital formats of training, could be useful to address such challenges. 38 In Georgia, further studies on SBIRT, or only Screening and Brief Intervention (SBI), implementation, and research about any potential implementation gaps, would benefit the process of wide-scale integration of SBIRT in primary care. Suggested by the SBIRT chain, establishing a referral system could be the most complex objective, and closer investigation and mapping of available treatment capacities is recommended.22,39,40 These data further emphasize developing and systematically applying user-friendly screening tools to evaluate cannabis use and its risks, mainly in primary healthcare systems. 41 Short inventories, such as the Single-Item Screen-Cannabis, should be considered for validation in the local context. 42
While documentation of cannabis use inquiry is rare (26.6%), and not always done when cannabis use is actually asked about, that is probably not unique to our sample, as a study from the US reported documentation of counseling done usually when patients screen positive for moderate-to high risk of substance use. 38 Even less common application of DSM-5 criteria for cannabis use related disorders diagnosis or referral undermines the value of detecting and recording this information in the patient’s history. Systematic implementation and documentation of cannabis use screening and screening results in medical records could be a rich source of data for epidemiologic surveillance of cannabis use behavior and its burden on population health. 43 In Georgia, the gradual improvement of health information systems and electronic health records ecosystems could be an opportunity to enhance relevant data quality and availability.
This study suggests that screening, counseling, and note-taking/documenting practices differ, as some physicians, who enquire about cannabis use, don’t eventually note this in patient histories. The differences between counseling and documentation could be explained by a lack of knowledge and physicians’ concern about potential legal and social consequences of recorded cannabis use in medical records (majority of surveyed PCPs lacked information on cannabis use policy in Georgia). Widespread stigma could be another explanation. While up to 20% of the respondents mentioned that they normally don’t encounter patients with cannabis use, it is difficult to estimate it without systemized use of valid screening tools for identification of such use. These dynamics highlight how stigma and legal uncertainty can interact with medical documentation, further limiting accurate record-keeping and effective counseling in primary care.
Our findings of limited knowledge and application of widely-recognized screening instruments and SBI approaches could be explained by the limited professional development and medical training opportunities available prior to the data collection period (first half of 2024) in this regard. Previous studies had demonstrated that SBIRT training improved screening behavior, knowledge, and attitude among clinicians. 44 Up to now, the surveyed practitioners in Georgia have had little opportunity to acquire relevant knowledge and skills (which also points to ways to address the gap). However, initiatives such as the CME on substance use screening and prevention in primary care, accredited in April 2025, offer an opportunity to improve providers’ readiness. 33 Gradual re-introduction of CME/CPD requirements and periodic medical licence review practices in Georgia should facilitate continuing training of the personnel, and promote life-long learning in the primary care workforce.
We observed higher screening and documentation of cannabis use among clinicians with more time per visit (which was similar to time allocated per patient in other settings). 45 This supports the notion that competing priorities in brief primary care encounters can displace substance use assessment. Practical steps such as health workforce strengthening (including interprofessional teams), pre-visit questionnaires, single-click documentation, or electronic medical records prompts may help when visit length cannot be extended. As time costs are a major component of healthcare costs, solutions to the limitations seen in primary care need to be considered in the wider health policy and systems context. Application of artificial intelligence-based tools to contribute to administrative tasks and notes-taking duties is another area to explore. 46 We should note that the introduction of structured, time-efficient screening and counseling instruments helps save time in itself.21,47
Limitations
We could not establish causality due to the cross-sectional design of the study. The observed differences in screening and counseling practices should be interpreted as associations rather than causal effects; unmeasured workflow or organizational factors may contribute. The use of non-probability sampling techniques to collect the survey data, and the design of the qualitative exploration limits the generalizability of our findings to the respondent individuals. The survey instrument was not validated. We could not calculate the response rate, as we don’t know the exact number of practitioners who received the questionnaire.
Conclusions
The respondent Georgian primary care physicians in this study report insufficient readiness to provide screening and counseling for recreational cannabis use. While international evidence supporting SBIRT’s effectiveness to address cannabis use is still limited, we recommend further studies to identify the counseling approaches which could be implemented in the country. Additional situational assessment and identification of barriers to provide structured counseling, and possibly SBIRT, for cannabis, is also recommended. Further academic work would inform educational and technical interventions to enhance screening and counseling practice for cannabis use in primary care settings in the country.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251394522 – Supplemental material for Primary Care Physicians’ Knowledge and Counseling on Cannabis Use in the Country of Georgia: Results of a Mixed-Method Exploratory Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319251394522 for Primary Care Physicians’ Knowledge and Counseling on Cannabis Use in the Country of Georgia: Results of a Mixed-Method Exploratory Study by Aleksandra Nadiradze, Ketevani Khetsuriani, Tamari Talakvadze, Mariam Gulbani, Elene Ratiani, Anano Nebieridze, Nino Gaprindashvili, Nino Tabagari, Karsten Lunze and Ilia Nadareishvili in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank Luka Kiguradze for his contribution to the manuscript.
Ethical Considerations
Following the review of the study aims, design, and potential outcomes, an ethical approval for this study was obtained from David Tvildiani Medical University Ethics Committee (#2/23, January 9, 2023). All participants received written and oral information regarding the study objectives, backgrounds, and how the data would be used and treated. The quantitative component participants expressed their own consent to participate by continuing to the first page of the survey. The interview participants gave their own consent verbally, following the introduction to the study and prior to the interview itself. We took measures to ensure confidentiality and anonymity throughout the research process.
Author Contributions
I.N., K.L., N.T., and AL.N. conceived and planned the study. I.N., K.L. and N.T. obtained funding. All authors carried out data collection. I.N. and AL.N. performed data analysis and wrote the first draft of the manuscript. All authors contributed to the interpretation of the results. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Shota Rustaveli National Science Foundation of Georgia (SRNSFG) [grant number YS-22-814].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Quantitative data is available upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.