
Abstract
Patients generally access colorectal cancer (CRC) screening through primary care physicians. National guidelines recommend CRC screening for adults beginning at age 50, yet one-third of Americans are not up to date.
Keywords
Rates of colorectal cancer (CRC) testing in the United States have been slowly trending up.1-3 Data based on self-report indicate that about two-thirds of people aged 50 to 75 years in the United States have had either CRC testing, defined as fecal occult blood test (FOBT), within the past year or lower endoscopy within the past 10 years.1,3,4 These studies did not distinguish between flexible sigmoidoscopy and colonoscopy, so it is uncertain how many people actually met the most current screening guidelines.1,5
A study based on chart review completed in the Iowa Research Network in 2004 showed that 46% of patients were up to date on CRC testing and that 62% of these tests were prompted by patient symptoms rather than true screening examinations. 6
Several national organizations have guidelines for CRC screening.5,7-9 Studies based on previous versions of the guidelines have shown that there is variation among physicians when it comes to recommending CRC screening to their patients.6,10,11 Physician knowledge of CRC screening guidelines is variable.12-14
This article reports on the knowledge, perceptions, and practices of Iowa family physicians concerning CRC screening. Our sample comprised Iowa family physicians who attended an initial study meeting held at their medical office to learn about participating in a randomized clinical trial to improve CRC screening.
Methods
The University of Iowa Institutional Review Board approved the study and methods. Recruitment of family medicine practices was conducted through the Iowa Research Network, a practice-based research network with 307 family physician members from 150 offices in 72 of Iowa’s 99 counties. The network’s mission is to create new knowledge with relevance to rural primary care clinicians and their patients, with the outcome of improving the patients’ care. At the time of the start of the study in 2008, 58 network practices were interested in participating, and 16 were randomly selected from the 27 practices located in counties with median income levels below the state average.
Questionnaire
A questionnaire was developed by the principal investigator (B.T.L.) that assessed practices concerning CRC screening, knowledge of CRC screening guidelines, strategies that might help improve screening rates, perception of rates of screening for patients in various age groups (ages 50 to 64, 65 and over), and for which types of visits CRC screening is typically recommended. This questionnaire was modeled after the questionnaire used in another study of Iowa family physicians. 14 The questionnaire is available on request.
Study Information Visits
At the beginning of the study, 1 of the 2 lead study physicians visited each office and provided standardized information about the design of the funded randomized study, asked physicians to review and sign the informed consent document, and requested physicians to complete a baseline questionnaire. Once we collected the informed consent and the baseline questionnaire, we reviewed the current guidelines for CRC screening. Thus, the questionnaire was completed before any factual information was presented about the CRC screening guidelines. The meetings took approximately 50 minutes, and all office health care providers were invited to attend. At the beginning of the meeting, a folder of information was given to each provider that included the following: baseline physician survey, 2 informed consent documents (1 for the provider to keep), CRC screening pocket card, US Preventive Services Task Force 7 and American Gastroenterological Association 5 CRC screening guidelines, and a diagram showing the study design. Visits were conducted in 2008 and 2009. For those providers who were unable to attend the meeting, a folder with the information was given to the office administrator to distribute to them. Some health care providers who were unable to attend the meeting sent their informed consent and questionnaires in by mail.
Analyses
Data from the questionnaire were double entered and verified. Means and frequencies were completed in SAS 9.0. Perceptions of physicians regarding CRC screening were categorized as agree (4 or 5 on a 5-point scale) versus disagree (1, 2, or 3), and t-tests were run of the estimated percentage of eligible patients in their practice who have had CRC screened as recommended. Physicians were categorized as being in practices that either performed or did not perform lower endoscopy, and estimated screening rates were compared using t-tests.
Results
A total of 85 (65%) health care providers (physicians, physician assistants, and nurse practitioners) from 16 family medicine offices completed the baseline survey out of 131 who attended the recruitment meetings. Sixty-five (76%) were physicians; the others were physician assistants or nurse practitioners. Forty-nine (58%) were men. They had been in practice an average of 15 years.
Fifty-six (66%) were aware of the joint guidelines published in 2008 by the American Gastroenterological Association and the American Cancer Society (ACS). 5 Eighty-two providers (97%) reported 50 as the age at which the average-risk man or women should begin CRC screening. The remaining 3 thought screening should begin at age 40 or 45.
Seventy-seven (91%) correctly answered that the interval for screening depends on the test chosen. All providers said that a test for occult blood in the stool should be conducted annually; 83 (98%) said that colonoscopy should be completed every 10 years; 75 (88%) said that flexible sigmoidoscopy should be completed every 5 years; 70 (82%) said that the barium enema should be completed every 5 years; and 39 (46%) said that the computed tomography colonography should be completed every 5 years. Eighty-three (98%) said that the recommended follow-up test for a positive FOBT is a colonoscopy.
Regarding office policies and practices related to CRC screening, 7 providers (8%) agreed that their practice had a written policy regarding CRC screening, and 15 (18%) agreed that their practice used chart reminders to let the provider know when a patient is due for CRC screening. Twenty-seven providers (32%) felt that their charts were organized such that they could easily determine a patient’s CRC screening status. Thirty-two (38%) felt that their practice encouraged office staff to help facilitate CRC screening through activities such as identifying eligible patients and explaining the tests and preparation. Fifty-nine (70%) felt that it would be helpful to have a nurse educator or other office staff member discuss CRC screening with patients and order appropriate screening tests.
Information on provider attitudes toward CRC screening is shown in Table 1. Eight-two providers (96%) agreed that colon cancer can largely be prevented or cured if caught early, and 72 (86%) agreed with and tried to follow CRC screening guidelines. Only 4 (5%) felt that they did not have time to adequately discuss CRC with patients, but 30 (36%) said that they sometimes forget to discuss screening with eligible patients.
Provider Attitudes Toward Colorectal Cancer Screening (N = 85)

Abbreviations: CRC, colorectal cancer; ACS, American Cancer Society.
Concerning their own practice, providers estimate that they recommend CRC screening to 75% of eligible patients between the ages of 55 and 80. Providers report recommending screening for patients starting at age 50. Those who recommend discontinuation of screening at a certain age (68%) do so at an average age of 81; a third never recommend discontinuation of screening based on age. Providers estimated that 49% of men and 54% of women aged 50 to 64 years and 54% of men and 57% of women 65 and older in their practice are actually up to date with CRC screening.
Health care providers estimated the percentage of patients due for CRC screening with whom they discuss CRC screening options at different types of visits. Eighty-seven percent had such discussions during health maintenance visits; 50% did so during chronic care visits; and 12% brought up CRC screening during acute care visits. Providers report they typically spend 4 minutes on average discussing CRC screening with eligible patients but would prefer to have 7 minutes available for these discussions.
Twenty-six providers (31%) report having an immediate family member with colon cancer or polyps, and 31 providers (36%) have a family member or close friend who was diagnosed with colon cancer through screening.
Ten providers (12%) perform flexible sigmoidoscopy themselves, and 22 (26%) have partners who do flexible sigmoidoscopy. Only 1 provider in the study performs colonoscopies, but 15 (18%) have partners who do so.
Table 2 summarizes providers’ responses to true/false questions regarding current CRC screening guidelines. These questions were answered before the investigators provided factual information about CRC screening guidelines to the attendees. Sixty-seven providers (79%) felt that colonoscopy is the preferred screening test for average-risk patients based on ACS guidelines, while it is actually one of several acceptable options.5,7,9 Twenty-one providers (25%) mistakenly thought that a single in-office stool sample for fecal occult blood done annually is an acceptable screening test for CRC.5,15,16
Providers’ Knowledge of Colorectal Cancer Screening Guidelines, No. (%)

Abbreviations: CRC, colorectal cancer; ACS, American Cancer Society.
Providers were asked to prioritize their CRC screening recommendations based on patient insurance status. Forty-seven providers (55%) said that the FOBT would be their first choice for screening in patients with no insurance, while 20 (24%) would recommend colonoscopy. In contrast, for patients with “best insurance,” 80 providers (94%) said that their first choice for screening would be colonoscopy.
Providers report that the average distance to the colonoscopy facility that they use is 1.8 miles. From time of referral, it takes patients 13 days on average to receive a colonoscopy.
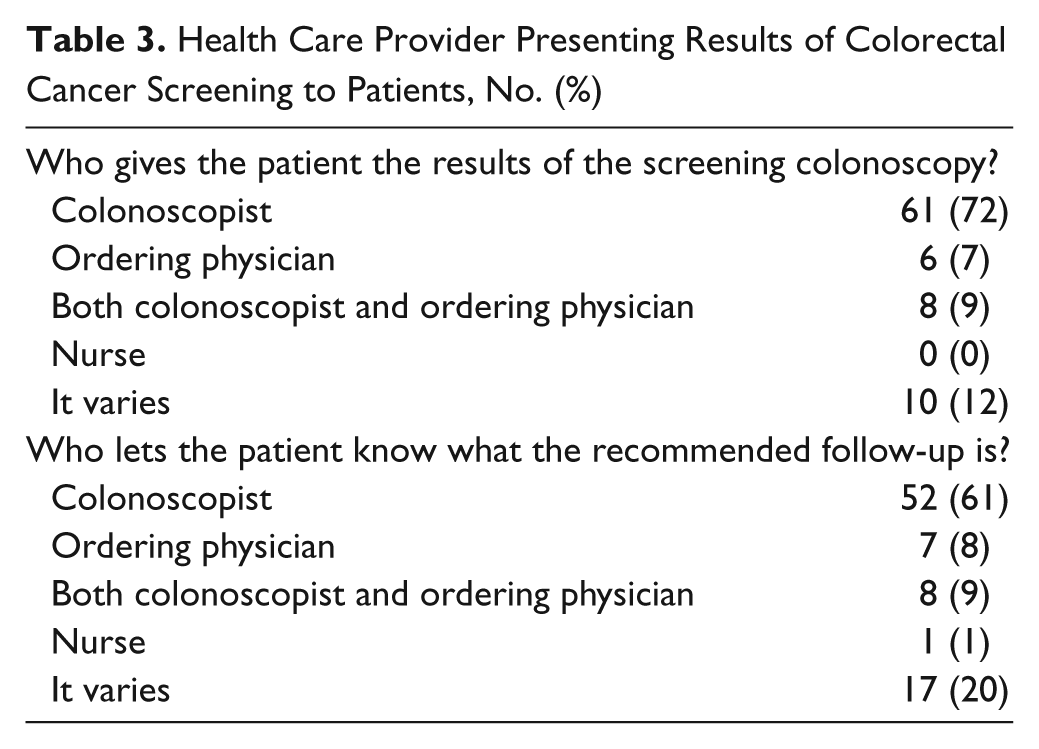
Table 3 shows how results and recommended follow-up of colonoscopies are communicated to patients. Sixty-one (72%) and 52 (61%) providers said that the colonoscopist was responsible for giving the patient results and communicating follow-up recommendations, respectively. Ten (12%) and 17 (20%) providers said that the person who communicated colonoscopy results and recommended follow-up was variable, respectively.
Health Care Provider Presenting Results of Colorectal Cancer Screening to Patients, No. (%)
With regard to perceptions concerning CRC screening, those who agreed that they encourage their office staff to participate in screening estimated that they offer screening to more patients than those who disagreed (82.8% vs 70.2%, P < .0001); in addition, those who agree with and try to follow the ACS guidelines estimated that they offer screening to more patients than those who disagree (77.4% vs 60.5%, P = .004). There was no association with estimated screening rates and agreement with any of the following statements: “My practice has a written policy concerning CRC screening,” “My practice uses a chart reminder to alert the physician when patients are due for CRC screening,” “Our charts are organized to easily determine a patient’s CRC screening status,” “It would be helpful to have a nurse educator or other member of my office staff discuss and order screening tests for patients,” “I am well informed about the ACS screening guidelines for CRC,” “I feel well prepared to adequately discuss CRC screening with my patients,” “I sometimes forget to discuss CRC screening,” “My patients are generally receptive to being screened for CRC after I talk with them,” “I do not have time to adequately discuss CRC screening,” “My patients find the CRC screening prep/procedure to be uncomfortable,” “Most patients have to be talked into CRC screening,” “Colon cancer is a disease that can be prevented or cured if caught early,” “It is easy to get average risk patients to agree to a flexible sigmoidoscopy,” and “It is easy to get average risk patients to agree to a colonoscopy.”
There was no association with estimated screening rates and having an immediate family member with colon cancer or polyps (yes vs no), nor was there an association with having a family member or close friend diagnosed with colon cancer through screening. Physicians in practices who performed lower endoscopies had higher estimated screening rates than did those in practices who did not perform lower endoscopies (79.3% vs 72.1%, P = .07).
Discussion
Providers in this study generally understood that CRC screening intervals depend on the test chosen, and they reported accurately that a FOBT should be done annually and that colonoscopy should be done every 10 years. Nearly all providers (99%) correctly answered that CRC screening should be offered, even in the absence of symptoms. However, 25% of providers answered incorrectly that a single in-office stool sample for fecal occult blood done annually is an acceptable screening test for CRC. Nadel and colleagues also found that 25% of his national sample of providers indicated that they used an in-office single-sample FOBT. 15 This mechanism is not supported in the current CRC screening guidelines, because this type of test misses 95% of neoplasias.5,17 In addition, nearly 80% of providers feel that the guidelines promote colonoscopy as the preferred test, when the guidelines actually indicate that any one of several tests are acceptable.5,7-9 There is no difference in life years gained by a screening strategy of colonoscopy every 10 years versus an annual FOBT using a sensitive test. 18 Sensitive FOBTs done annually or biennially reduce mortality from CRC by 15%. 19 The newer fecal immunochemical tests have higher sensitivity (61% to 91%) than nonrehydrated Hemoccult II (25% to 38%). 8
Our results demonstrate a striking lack of a systems approach for CRC screening in these practices and the difficulty physicians have in ascertaining screening status. Physicians who stated that their practice encourages office staff to facilitate screening and that they agree with and follow ACS guidelines estimated significantly higher screening rates than those who disagreed with these statements. In addition, physicians in practices where lower endoscopies were performed estimated higher screening rates, which may be due to the fact that physicians in practices where endoscopy is performed have a higher level of awareness of CRC screening guidelines.
About one-third stated that their medical records were organized to easily determine a patient’s screening status. Practices desiring to follow CRC screening guidelines may want to consider having a specific policy for providers regarding CRC screening, since few (8%) reported having this available. In addition, only 18% reported use of chart reminders for screening. Klabunde et al also found only 30% of 1266 physicians in a national survey had a reminder system for CRC screening. 20 Establishing or improving an office reminder prompt system, in addition to making it easy to ascertain a patient’s CRC screening status, may reduce the number of times that a physician simply forgets to bring up CRC screening with an eligible patient.11,21 Many electronic medical records have the capability to provide a reminder “pop-up” message when a patient’s record is opened. Adding a reminder that the patient is due for CRC screening has increased CRC screening rates. Reminder letters to screen-eligible patients accompanied by a FOBT (or an easy way to obtain one) is one type of system support that has been shown to increase CRC screening rates.22-24
Family physician offices could also implement systems for increased participation by office staff in facilitating screening. Only 38% felt that their practice encouraged participation by office staff in facilitating screening, while 70% agreed that it would be helpful to have a nurse educator discuss and order CRC screening for appropriate patients. Physicians who agreed that their practice encourages office staff to facilitate screening estimated that a higher proportion of their patients were screened for CRC. A unique randomized controlled trial was conducted in 6 community health clinics serving multiethnic patients with low baseline CRC screening rates; this program randomized eligible individuals either to an FOBT with an influenza vaccine or to an influenza vaccine only. 25 The odds of receiving CRC screening was 2.22 in the combined FOBT-influenza group compared with the influenza-only group. 25 The CRC screening rate increased from 32.5% to 45.5% (increase of 13 percentage points) in the combined FOBT-influenza group and from 31.3% to 35.6% (increase of 4.3 percentage points) in the influenza-only group (P = .018 for change difference). Office systems that systematically target CRC screening have great promise for improving screening rates.23,26
Offices may want to develop a standard protocol for ensuring receipt of reports from the colonoscopist and encourage their colonoscopist to routinely provide information on the recommended follow-up interval. Physicians in this study generally felt that it was the colonoscopist’s job to provide the results to patients (72%) and to communicate the follow-up interval to patients (61%). There are published guidelines for standardized colonoscopy reporting that include “documentation of colonoscopy results with the patient and referring clinician, including pathology results and recommendations for follow-up.”27,28 A study conducted among Iowa family physician practices reviewed 581 family medicine medical records indicating that a colonoscopy had been completed; among those, 89 (15%) did not have a copy of the colonoscopy report. Only 223 (45%) listed the follow-up interval for next colonoscopy. 29 A study by Greene et al found that in a colonoscopy registry project, polyps could be matched with histology only 50% of the time. 30 It is important that patients who undergo screening receive their results and understand their recommended follow-up interval. However, there is no agreed-on standard for whether the colonoscopist or the referring physician should provide the results of the colonoscopy to patients. Family physicians in the present study were involved up to 28% of the time in providing patients with results and up to 37% of the time in letting patients know their recommended follow-up. Thus, a family physician should be well versed on CRC screening and adenoma follow-up guidelines, and colonoscopists should provide patients and referring physicians with easily understood reports so that results and appropriate follow-up intervals are clearly stated.
The results of the present study were similar to those found in a survey of Iowa family physicians in 2003. 14 In both studies, physicians generally felt comfortable with CRC screening guidelines and tried to follow them in their practices. However, a minority in each study had systems in place that facilitated screening, such as a practice policy, chart reminders, or an ancillary staff. Both studies also found that physicians were much more likely to discuss CRC screening during health maintenance visits versus acute or chronic care visits. Patients who choose not to come for health maintenance visits or whose insurance does not cover such visits may be missing out on receiving up-to-date CRC screening recommendations.
New York City primary care providers were more likely to recommend colonoscopy in areas with high socioeconomic status and FOBT in low areas of low socioeconomic status. 31 This is similar to our finding that colonoscopy is providers’ first choice for CRC screening in patients with the “best” insurance, while FOBT testing is their first choice for uninsured patients. Given that annual testing with a sensitive FOBT offers similar life years gained when compared with colonoscopy every 10 years, 18 it makes sense to offer a sensitive FOBT to patients with limited financial resources.32,33
A limitation of this study is the selection bias of receiving surveys from a relatively small sample of physicians practicing in a single Midwestern state who had agreed to participate in a randomized clinical intervention study to improve CRC screening and who were willing to attend a lunch meeting held at their practice. 23 These physicians are likely more motivated than the average physician to make sure that CRC screening occurs. For this report, the questionnaire was completed by the physicians before any discussion of the current guidelines took place; thus, they were not “quizzed” immediately after a presentation on CRC screening. There was no verification of the patient rates of CRC screening.
Conclusions
Physicians were generally knowledgeable about CRC screening guidelines, but a quarter mistakenly felt that single-sample in-office fecal testing was appropriate. There was a striking lack of office systems for identifying eligible patients and facilitating CRC screening. The majority of physicians felt that having office staff discuss and facilitate CRC screening with patients would be helpful. Physicians reported that some patients continue to be reluctant and find excuses not to comply. Family physicians vary in their opinions about who should provide colonoscopy results to the patient, with most feeling that the colonoscopist is responsible. Future work is needed to make sure that physicians understand the current CRC screening guidelines and to ensure that colonoscopy results are provided to patients in a way that they can understand.
Footnotes
Acknowledgements
We gratefully acknowledge the support of the American Cancer Society (Research Scholar Grant Targeted-08-148-01-CPPB; B.T.L.) and the University of Iowa, Department of Family Medicine.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.